Download presentation
Presentation is loading. Please wait.

1
Examination of the Eye & Ear
Professor Janet M. Galiczewski RN,CCRN,MSN,ANP

2
A & P Outer Eye

3
External Eye Eyelid: Distributes tears, limits light entering eye, protects eye. Upper lid covers 2-3 mm of iris but NOT pupil. The lower lid sits directly on the lower ring of the iris Palpebral Fissure: Opening between eyelids. Conjunctiva: Thin membrane covering most of the anterior surface of eye & eyelid, protects eye.

4
Lacrimal Gland: located in temporal region of eyelid
Lacrimal Gland: located in temporal region of eyelid. Produces tears ( drain into lacrimal sac from puncta to nasolacrimal duct to nasopharynx). Puncta is the only visible portion of the lacrimal apparatus.
. Puncta is the only visible portion of the lacrimal apparatus.")
5
Eye Muscles (EOM’s) EOM’s are responsible for eye movement 4 Rectus
2 Oblique Innervated by CN III, CN IV, CN VI Levator palpebrae muscle which raises upper eyelid innervated by CN III

6
A&P Inner Eye

7
Internal Eye Sclera: “White of the Eye,” protective, provides structure. The optic nerve is attached to it at the back of the eye. Cornea: continuous with sclera, transparent dome shaped window that covers iris, pupil,& anterior chamber. Provides most of the eyes optical power. 1. Refracts light 2. Eye focus (fixed) 3. Protects - nerve endings sensitive to touch, temp, & chemicals
 3. Protects - nerve endings sensitive to touch, temp, & chemicals.")
8
Aqueous Humor: Fluid produced by ciliary body that flows from posterior chamber through pupil to anterior chamber. Controls pressure inside eye. Iris: Circular, contractile muscular disc containing pigmented cells. Regulates the light levels inside eye. Pupil:Center of iris.Tiny sphincter muscles constrict pupil to light & tiny dilator muscles dilates eye in dim light.

9
Lens:Their purpose is to focus light on the retina
Lens:Their purpose is to focus light on the retina. The lens have ability to change shape and to adjust to close & distant vision. This is called accommodation. Retina: Sensory network that lines the back of the eye, transforms light impulses to electrical impulses.Impulses travel via optic nerve to cerebral cortex. Here they are transformed into images. 1. Cones:macula portion of retina, central vision, bright light, color appreciation 2. Rods: spread throughout peripheral retina, peripheral & night vision, dim light

10
Mechanisms of Vision Vision depends on light rays which enter eye, passes through cornea & pupil, then focus on retina by the lens. Vision may be altered from local or systemic disease.

11
Examination of the Eye Review of systems
Inspection of external structures. Measurement of visual acuity. Determination of visual fields. Evaluation of Extraocular Movement. Estimation of Intraocular pressure. Exploration of Ocular Fundus.

12
Review of Systems Start with open ended questions….
Onset of problem gradual or sudden? Problem seeing close work or distance? Pain or headaches? Last eye exam Glasses or contact lens Sty: Eyelash follicles become infected. Chalazion:cystlike mass of eyelid; consistsof collecte debris obstr. meibomian gland.

13
Inspection of External Structures
Eyelids: Inspect blinking, external surface for lesions, superficial vascularity, edema. Ptosis Check position of lids for Eversion, Inversion. Check Enophthalmos, Exophthalmos Ptosis: Eyelid falls belows iris. Eversion:turning outward of the lower lid. Inversion: turning inward of the lower lid.

14
Eyelids (cont). Check for corneal drying Palpate for ocular tension.
Check Lacrimal apparatus Eyebrows, Eyelashes: note quantity, distribution, color, texture. Sty Chalazion

15
Conjunctiva & Sclera Examine palpebral conjunctiva lining the lids & bulbar conjunctiva covering sclera. Note: color, vascular patterns, nodules, swelling. Conjunctivitis

16
Cornea, Lens & Iris Using oblique lighting note: scars, irregularities, foreign bodies, opacities Check iris for crescent shadow on medial side of iris (no shadow should be seen). Arcus Senilis
. Arcus Senilis.")
17
Pupils Note: size, shape, equality (slight inequality may be normal (anisocoria). Check pupillary reaction to light. Look for Direct reaction Consensual reaction Identify as: prompt or brisk (normal), sluggish, or absent.
, sluggish, or absent.")
18
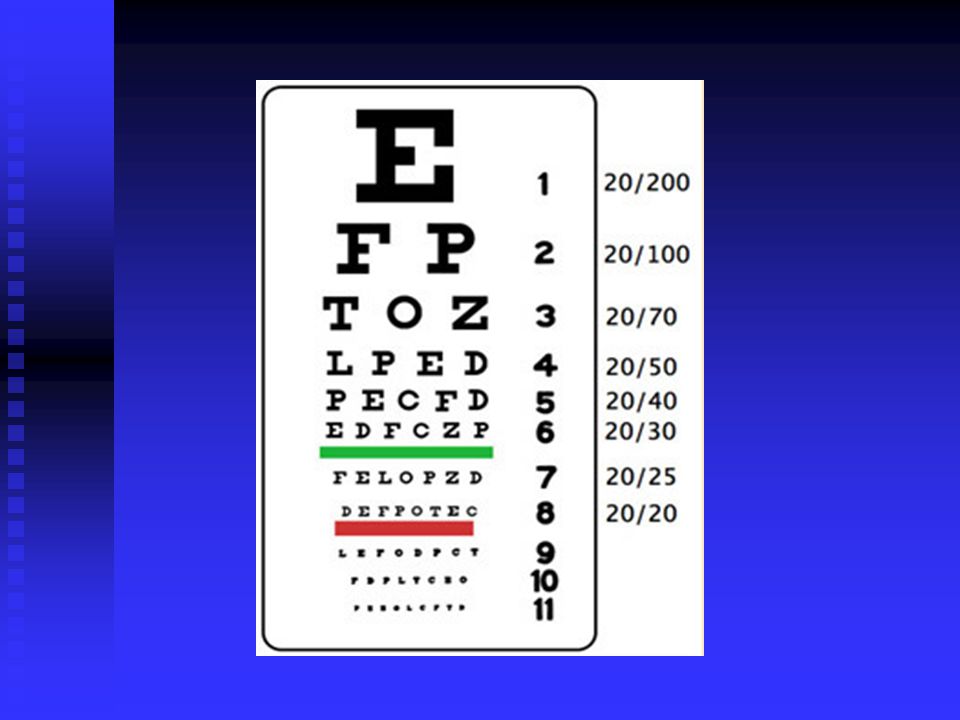
Visual Acuity Snellen Chart-Check distant visual acuity, color.
Ex. 20/30 vision. 20=distance from chart. 30=distance at which normal eye can read that line of letters. Presbyopia Myopia (near-sightedness) Hyperopia (far-sightedness) Presbyopia: Impaired near vision Myopia: Impaired far vision OS, OD, OU
 Hyperopia (far-sightedness) Presbyopia: Impaired near vision. Myopia: Impaired far vision. OS, OD, OU.")
20
Visual Fields Defined as the entire area seen by an eye when its gaze is fixed on a central point. Superficially tested by comparing the pts. peripheral vision with your own. Technique: “Confrontation”Visual Fields Confrontation 2 feet away Cover one eye, cover your eye directly opposite.

21
Extraocular Movements (EOM)
To detect weakness or paralysis of extraocular muscles. Corneal Light Reflex EOM’S “H” Pause to detect nystagmus (fine rhythmic oscillation of the eyes). Combine with convergence. Check for lidlag. Corneal light reflex: 2 ft. in front, reflection of pt. Corneas “H” pause on upward and extreme lateral gaze.
. Combine with convergence. Check for lidlag. Corneal light reflex: 2 ft. in front, reflection of pt. Corneas. H pause on upward and extreme lateral gaze.")
22
Opthalmoscopy (Fundoscopy)
Important in evaluation of local disorders (cataract, retinal detachment, or systemic disease) The light beam passes through the cornea to aqueous humor of the anterior chamber to lens to the vitreous humor, strikes the retina & structures that make up fundus of the eye. Fundus-internal surface of the retina
 The light beam passes through the cornea to aqueous humor of the anterior chamber to lens to the vitreous humor, strikes the retina & structures that make up fundus of the eye. Fundus-internal surface of the retina.")
23
Opthalmoscopy (Fundoscopy)cont.
Image of the optic disc, blood vessels, retina, macula, fovea. Technique- if you wear glasses leave on or correct for deficit with ophthalmoscope. Turn lens disc to “O” Keep index finger on lens disc to focus during exam.

24
Opthalmoscopy (Fundoscopy)cont.
Darken room-dimly lit, switch on ophthalmoscope light to round beam of white light. Use your Right hand & Right eye for pts. Right eye. Same for Left. You & pts. Eyes should be at same level. Instruct pt to look up & over your shoulder at a fixed point on the wall.

25
Opthalmoscopy (Fundoscopy)cont.
From about 15 inches away from pt & 15 degrees lateral to pt. Line of vision Shine light beam into pupil You will see Red Reflex (orange, red glow in pupil) Cataract will interrupt. Keep beam on red reflex, move in 15 degrees to pts line of sight, until scope is close. You will see the OPTIC DISC.(yellow /orange or creamy pink; oval or round).
 Cataract will interrupt. Keep beam on red reflex, move in 15 degrees to pts line of sight, until scope is close. You will see the OPTIC DISC.(yellow /orange or creamy pink; oval or round).")
26
Ophthalmoscopy (Fundoscopy)cont.
If only vessels seen trace back to disc (bring disc into sharp focus) Pattern of Exam:Red Reflex, Disc, Vessels, Retina including Macula. Red Reflex: note opacities, dark lines, black spots. Disc Color: yellow, orange to creamy pink, disc diameter is about 1.5 mm
 Pattern of Exam:Red Reflex, Disc, Vessels, Retina including Macula. Red Reflex: note opacities, dark lines, black spots. Disc Color: yellow, orange to creamy pink, disc diameter is about 1.5 mm.")
27
Vessels Arteries Color: Light Red
Size: Smaller Diameter (2/3 less than vein). Light Reflex: Bright Veins Color: Dark Red Size: Larger Light Reflex: Less bright or absent
. Light Reflex: Bright. Veins. Color: Dark Red. Size: Larger. Light Reflex: Less bright or absent.")
28
Fundoscopy (cont). HTN: arterioles become narrow & tortuous,
Ratio (A/V) decreases to 1:2 or 1:3 (Normal 2:3, 4:5). AV Nicking-Kinking or indentation of the venule at a crossing. Retina: Note-lesions, size, shape, color, distribution. Hemorrhage: may appear flame shaped, deep red spots.
 decreases to 1:2 or 1:3 (Normal 2:3, 4:5). AV Nicking-Kinking or indentation of the venule at a crossing. Retina: Note-lesions, size, shape, color, distribution. Hemorrhage: may appear flame shaped, deep red spots.")
29
Fundoscopy (cont). Exudates: Hard or soft
Soft:”cotton wool exudates” fluffy, fuzzy outline Hard: smaller with discrete borders Next, move laterally to inspect macula (temporal) Fovea tiny pinpoint of bright in center of macula.
 Fovea tiny pinpoint of bright in center of macula.")
30
Fundoscopy (cont). Senile Macular Degeneration:important cause of impaired central vision in elderly. Look for hemorrhage, exudate, cysts. Degree of retinal changes direct relationship to severity of disease.

31
A & P of the EAR Sensory organ:Function is to identify, locate interpret sound. Maintain equilibrium. Divided into 3 parts:External,Middle,Inner.

32
External Ear Auricle: varies size & shape.
Should be = in height & size Structural landmarks of the auricle: Helix: prominent outer ridge. Antihelix: parallel & anterior to helix. Tragus: anterior to auditory canal. Antitragus: opposite auditory canal opening. Lobule: Soft, lobe at bottom of auricle.

33
External Auditory Canal: 2
External Auditory Canal: 2.5-3cm length narrows toward mid-portion & widens near eardrum. “S” shaped pathway leads to middle ear. Consists of bone & cartilage covered with thin sensitive skin. Mastoid process: bone behind & below the ear canal ( mastoid part of temporal bone).
.")
34
Middle Ear Air filled cavity in temporal bone separated from external ear by tympanic membrane. TM (Eardrum): shiny, translucent & pearly grey. Sound transmitted by 3 tiny bones: (ossicles) malleous, incus, stapes. Eustachian tube leads to nasopharynx allows for equalization of air pressure with atmospheric pressure (swallowing).
 malleous, incus, stapes. Eustachian tube leads to nasopharynx allows for equalization of air pressure with atmospheric pressure (swallowing).")
35
Middle Ear TM visualized (otoscope) as an oblique membrane pulled inward at its center by the malleus. You can locate: Handle of malleous Short process of malleous Umbo Cone of light Pars flaccida Pars tensa

36
Inner Ear A curved cavity within a bony labyrinth
Consists of a vestibule, semicircular canals, cochlea. Cochlea contains the organ of corti which transmits sound impulses to the Cranial Nerve VIII (Acoustic).
.")
37
Physiology of Hearing Vibrations of sound are transmitted to the external ear, then to the eardrum, to the ossicles of middle ear to the cochlea (of inner ear). Vibrations of cochlea cause the organ of corti to stimulate impulses in CN VIII which are transmitted to temporal lobe for interpretation . Normal hearing pathway: Air Conduction
. Vibrations of cochlea cause the organ of corti to stimulate impulses in CN VIII which are transmitted to temporal lobe for interpretation . Normal hearing pathway: Air Conduction.")
38
Types of Hearing Loss Conductive Hearing Loss: Occurs when changes in outer or middle ear impairs conduction of sound to inner ear. Air conduction is impeded d/t Excessive cerumen, foreign body, otitis media, tumor of middle ear, otitis externa, fluid in middle ear (more common in < 40 years old).
.")
39
Types of Hearing Loss Sensorineural Hearing Loss: Occurs with impairment of organ of corti. EX: Sustained exposure to loud noise, ototoxicity d/t drugs (aminoglycosides, antibiotics, chemo, lasix) syphilis, DM More common in older people Loss often mid to high frequency range. Mixed Hearing Loss: Both types combined.
 syphilis, DM. More common in older people. Loss often mid to high frequency range. Mixed Hearing Loss: Both types combined.")
40
Technique for Ear Examination
External Ear : Inspection, Palpation Middle Ear: Inspection Auditory Acuity: Whisper Watch Weber Rinne

41
Technique for Ear Exam External Ear
Inspection : Each auricle & surrounding tissue. Note: deformities, lumps, discharge, may see tophi(deposits of uric acid crystals in helix; occurs with gout). Palpate: External ear for tenderness, masses. should be smooth, non tender. Otitis Externa- tender, swollen, narrowed moist external canal Otitis Media- non tender
. Palpate: External ear for tenderness, masses. should be smooth, non tender. Otitis Externa- tender, swollen, narrowed moist external canal. Otitis Media- non tender.")
42
Palpate mastoid process for tenderness, swelling, bruising.
Palpate tragus.

43
Ear Canal & Drum : Otoscope
Grasp auricle & have pt. Tilt head to opposite side Adult: Pull helix up, back & slightly out. Insert largest speculum that ear will accommodate. Brace hand against pts. Head Insert otoscope into canal-down & forward (reposition head if you can’t visualize landmarks) Inspect & identify any discharge or foreign bodies in ear canal. Note: redness, swelling. Cerumen may obstruct view.
 Inspect & identify any discharge or foreign bodies in ear canal. Note: redness, swelling. Cerumen may obstruct view.")
44
Otoscope (cont). Inspect eardrum: note color, contour
Otitis Media: red, bulging drum, loss of landmarks, dilated blood vessels may cause spontaneous rupture & conductive hearing loss. Identify bony landmarks: cone of light 7 o’clock -Left Ear 5 o’clock – Right Ear

45
Otoscope (cont). Move speculum: view as much of drum as possible.
Identify: Pars flaccida superiorly, margins of pars tensa, look for perforation.

46
Auditory Acuity CN VIII
Test one ear at a time. Ask pt. To occlude 1 ear with finger or hand. Whisper Test: Stand 1-2 ft. away (behind pt). Exhale & whisper 2 syllable words. Ex. Baseball Ticking Watch: Same procedure as whisper. Pt. Can hear ticking watch from 2ft. away equally. Weber Test: (Lateralization) Set tuning fork into light motion (vibration)
. Exhale & whisper 2 syllable words. Ex. Baseball. Ticking Watch: Same procedure as whisper. Pt. Can hear ticking watch from 2ft. away equally. Weber Test: (Lateralization) Set tuning fork into light motion (vibration)")
47
Auditory Acuity CN VIII
Weber Test (cont). Place tuning fork on top of pts. head or forehead. Ask pt. Where he hears it, one or both sides Normal = midline Conductive Hearing loss:Sound lateralizes to impaired ear. Sensorineural Loss: Sound heard in good ear.
. Place tuning fork on top of pts. head or forehead. Ask pt. Where he hears it, one or both sides. Normal = midline. Conductive Hearing loss:Sound lateralizes to impaired ear. Sensorineural Loss: Sound heard in good ear.")
48
Auditory Acuity CN VIII
Rinne Test Compares air & bone conduction . Place vibrating fork at base of mastoid (bone behind ear) When sound no longer heard- place ear canal & see if pt. can hear. Normal: AC > BC Conductive Hearing Loss: BC=AC or BC>AC Sensorineural Hearing loss: Sound heard longer through air. AC>BC (Normal)
 When sound no longer heard- place ear canal & see if pt. can hear. Normal: AC > BC. Conductive Hearing Loss: BC=AC or BC>AC. Sensorineural Hearing loss: Sound heard longer through air. AC>BC (Normal)")
Similar presentations








 separated by the palpebral fissue Eyelashes Tarsal glands Lacrimal apparatus Vision Accessory structures.>")








 Click here to launch video Click here to download print activity.>")
 than.>")
