Download presentation
Presentation is loading. Please wait.

1
Workshop 4: “Il late-presenter”
Moderatori: G. Ippolito, M. Moroni Discussant: R. Iardino Overview epidemiologica e razionale della terapia A. Lazzarin

2
Overwiev epidemiologica e razionale della terapia
Roma, dicembre 2010 Guidelines and Clinical Expertise Overwiev epidemiologica e razionale della terapia Prof. Adriano Lazzarin Università Vita-Salute San Raffaele, Milano

3
Late presenters = persons who present late to care, because unaware of their HIV positive status What’s ‘late’? late in respect of the recommended timing of therapy initiation

4
Linee guida di terapia antiretrovirale
Clinical category CD4 (cells/mm3) HIV RNA copies/mL EACS 2008 DHSS 2009 BHIVA 2008 CNA- SIMIT 2010 AIDS-defining or symptoms Any value Treat Asymptomatic < 200 200–350 Treat when pt ready 350–500 ≥ 100,000 Consider treatment Individual basis Consider trial* Consider treatment* > 350 < 100,000 Defer treatment Individual basis Consider trial
 HIV RNA copies/mL. EACS DHSS BHIVA CNA- SIMIT AIDS-defining or symptoms. Any value. Treat. Asymptomatic. < –350. Treat when pt ready. 350–500. ≥ 100,000. Consider treatment. Individual. basis. Consider trial* Consider treatment* > 350. < 100,000. Defer treatment. Individual basis. Consider trial.")
6
Late Presenter: Definizioni
Recentemente nel corso della Conferenza ‘HIV in Europe’ a Stoccolma è stato proposto di definire come Late Presenter i pazienti con valore di CD4 < 350/mmc V-LP (Very Late Presenter): pazienti con valore all’arruolamento di linfociti CD4+ <200/mmc o AIDS alla diagnosi LP (Late Presenter): pazienti con valore all’arruolamento di linfociti CD4+ <350/mmc o AIDS alla diagnosi
: pazienti con valore all’arruolamento di linfociti CD4+ <200/mmc o AIDS alla diagnosi. LP (Late Presenter): pazienti con valore all’arruolamento di linfociti CD4+ <350/mmc o AIDS alla diagnosi.")
7
Recorded prevalence of late presentation varies across Europe
Country Year of study n Definition % Spain1 1994–2000 30,778 AIDS < 1 month 28% France2 1996–2006 6805 CD4 < 200 cells/μL, AIDS < 1 year 30% Croatia3 2004–2006 161 CD4 < 200 cells/μL, AIDS, no seroconversion within 5 years 28% of MSM, 59% among heterosexuals UK4 2003 977 CD4 < 200 cells/μL 33% Italy5 1997–1998, 2000 968 CD4 < 200 cells/μL, AIDS 39% Switzerland6 1998–2007 1915 31% UK7 1996–2002 719 CD4 < 50 cells/μL 15% 10% 1. Castilla et al. AIDS 2002;16: Delpierre. Eur J Pub Health 2007;18: Begovac et al. AIDS Behav 2008;12:S Sullivan. BMJ 2005;330: Girardi et al. JAIDS 2004; 36: Wolbers. HIV Med 2008;9: Sabin. AIDS 2004;18:2145 7 7

8
Choice of definition complicates measurement of prevalence
Basis of definition: AIDS CD4 Both 14.0% 34.0% New patients presenting late (%) Survey carried out in September 2007 31.0% 8.9% 30.0% 15.0% 16.0% 26.7% Belarus, Estonia, Moldova, Portugal, Slovakia, and Slovenia did not report prevalence Belgium, Cyprus, Finland, Ireland, Latvia, Lithuania, Luxemburg, Romania, Sweden did not respond to survey 20.0% 38.0% 14.1% Adler et al. AIDS Care 2008:1 8
 Survey carried out in September % 8.9% 30.0% 15.0% 16.0% 26.7% Belarus, Estonia, Moldova, Portugal, Slovakia, and Slovenia did not report prevalence. Belgium, Cyprus, Finland, Ireland, Latvia, Lithuania, Luxemburg, Romania, Sweden did not respond to survey. 20.0% 38.0% 14.1% Adler et al. AIDS Care 2008:1. 8.")
9
Prevalenza V LP per area geografica 2000-2002 15,04% 2003-2005 11,2%
,04% ,2% ,8% * 17,6% ,5% ,2% ,5% * 11,5% ,1% ,1% ,6% * 1,02%

10
Persone che scoprono di essere HIV positive alla diagnosi di AIDS

11
Andamento late presenter dal 2000 al 2010 (giugno)
")
12
Presentazione tardiva nei pazienti afferenti presso l’Osservatorio Epidemiologico HIV di Modena
% La percentuale di persone AIDS presenters o con compromissione dello stato immunitario (LP ≤ 200 o LP ≤ 350) non hanno subito modificazioni significative nei periodi osservati. p=0.25 p=0.19 p=0.06
 non hanno subito modificazioni significative nei periodi osservati. p=0.25. p=0.19. p=0.06.")
13
Most frequent AIDS-defining illnesses

14
Un’alta proporzione di decessi in pazienti
con HIV è associata la ritardo diagnostico BHIVA audit: scenario leading to death n = 387 deaths between October 2004 and September 2005 Death not directly related to HIV Diagnosed too late for effective treatment Under care but had untreatable complication Treatment ineffective due to poor adherence Chose not to receive treatment HIV+ve, irregular care, re-presented too late MDR HIV, run out of options Successful treatment but suffered catastrophic event Unable to take treatment – toxicity/intolerance Died in community without seeking care Treatment delayed/ineligible for NHS Other Not known/not stated Percentage of deaths Lucas SB. Clin Med 2008;8:250 14 14

15
Nuove diagnosi di HIV nel Lazio Studio SENDIH 2004-2008
CD4 alla Diagnosi AIDS alla Diagnosi Late Presentation (AIDS e/o<350 CD4) 51% Advanced HIV disease (AIDS e/o<200 CD4) 32%
 51% Advanced HIV disease (AIDS e/o<200 CD4) 32%")
16
Numero CD4 alla diagnosi

17
In Summary By current definitions, many patients with HIV infection still present late Late presentation is associated with increased morbidity, mortality, and healthcare resource use, and may lead to increased disease transmission Guidelines are shifting towards earlier treatment Further strategies to encourage and facilitate earlier diagnosis and treatment are needed

18
HIV in Europe: ‘optimal testing and earlier care’
‘Late presenters and the infected not yet diagnosed population’ project2 to Study the epidemiology for persons presenting late with HIV over time, compared with those presenting early for care Develop methodologies that are able to estimate the size of the undiagnosed yet infected pool of persons European Parliament resolution 20 November 20081 ‘ensure accurate monitoring and surveillance by the European Centre for Disease Prevention and Control, including more precise estimates (size, characteristics, etc.) of the undiagnosed population’ A common definition would support these goals 1. European Parliament resolution of 20 November 2008 on HIV/AIDS: early diagnosis and early care. P6_TA(2008) [accessed September 2009]. 18
 of the undiagnosed population’ A common definition would support these goals. 1. European Parliament resolution of 20 November 2008 on HIV/AIDS: early diagnosis and early care. P6_TA(2008) [accessed September 2009]. 18.")
19
The test and treat strategy

20
Late diagnosis is common among migrants in Western Europe
Proportion of AIDS cases who were unaware of their HIV infection at the time of AIDS diagnosis in Italy ( ) Source: Not Ist Super Sanità, 2010; 23(4 suppl. 1) 20 20
 Source: Not Ist Super Sanità, 2010; 23(4 suppl. 1)")
21
GP/Emergency/Hospital/TB clinic/ Migrants services
The time between arrival to host country and HIV testing is about 3 years ARRIVE IN HOST COUNTRY WELL Paucity of information on HIV (including risk, prevention and treatment options) Informal networks / Word-of-mouth Lack of perceived risk of HIV Lack of perceived benefit in knowing HIV status (e.g. treatment options, eligibility to care) Pregnant Priorities: family Housing Visa/permit of stay Money/empolyment Antenatal services HIV test Institutional barriers (e.g. appointment system) Stigma Immigration concerns UNWELL fear of disclosure stigma political and legal consideration GP/Emergency/Hospital/TB clinic/ Migrants services HIV care Referral for an HIV test 21 Source: Burns FM et al. AIDS care, 2007; 19(1): 21
 Informal networks / Word-of-mouth. Lack of perceived risk of HIV. Lack of perceived benefit in knowing HIV status (e.g. treatment options, eligibility to care) Pregnant. Priorities: family. Housing. Visa/permit of stay. Money/empolyment. Antenatal services. HIV test. Institutional barriers (e.g. appointment system) Stigma. Immigration concerns. UNWELL. fear of disclosure. stigma. political and legal. consideration. GP/Emergency/Hospital/TB clinic/ Migrants services. HIV care. Referral for an HIV test. 21. Source: Burns FM et al. AIDS care, 2007; 19(1):")
22
Persone che scoprono di essere HIV positive alla diagnosi di AIDS: modalità di esposizione

23
Conclusioni

26
Main gaps in advanced naive treatment
Late diagnosis of HIV infection Under/mis-evaluation of HIV associated symptoms Lack of data on combined treatment of HIV and associated pathologies … and superfluos suggestion to observe the indication of guide-lines

27
Limit of SOC in AIDS-presenters: main concerns
THE cART EFFICACY WORST ENEMIES Time Tumours Toxicity Waiting time for resistance and loss of CD4 PI friendly treatment combination for EKS Short term side effects (rash) and PI-DDI with anti-TB therapy
 and PI-DDI with anti-TB therapy.")
28
SAPiT: Increased Survival With Concurrent HIV and TB Treatment
1.00 Early ART Sequential ART 0.95 0.90 Survival 0.85 0.80 ART, antiretroviral therapy; SAPiT, Starting Antiretrovirals at Three Points in Tuberculosis; TB, tuberculosis. The curves shown on this slide describe survival during the course of intensive, continuous, and post‑TB treatment. The orange line represents patients who started antiretrovirals after completing TB therapy. It is clear that the survival curves of patients who received early vs sequential antiretroviral therapy diverged, but the divergence was greatest following completion of TB therapy. It is interesting that most of the survival difference between the 2 treatment groups seemed to occur somewhat late. As mentioned earlier, data assessing whether there is a survival difference between patients treated with antiretrovirals during the intensive phase vs the continuous phase of TB therapy are awaited. Intensive phase of TB treatment 0.75 Continuation phase of TB treatment Post-TB treatment 0.70 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 Months Postrandomization Abdool Karim SS, et al. CROI Abstract 36a. Graphic reproduced with permission. 28

29
Prevalence of Late presenters according to definition in 1,902 patients with new HIV diagnosis at enrollment in Icona AD= AIDS or CD4<=200/cmm LP= AIDS or CD4<=350/cmm 43%, n=821 61%, n=1,168 AIDS presenters 16%, n=296

30
Long term risk of death associated with being LP (Cox regression model)
Separate models with fixed comparator = AIDS-free patients with a CD4 at baseline>350 cells/l (n=734) Late presenter Adjusted RH* 95% CI p-value Definition LP (n=1,168) AD (n=821) AIDS (n=296) AD (n=797) LP (n=1,154) *Adjusted for: age, gender, mode of HIV transmission, calendar year at baseline, hepatitis co-infection, nationality viral load and whether previously started ART
 Late presenter Adjusted RH* 95% CI p-value. Definition. LP (n=1,168) AD (n=821) AIDS (n=296) AD (n=797) LP (n=1,154) *Adjusted for: age, gender, mode of HIV transmission, calendar year at baseline, hepatitis co-infection, nationality viral load and whether previously started ART.")
31
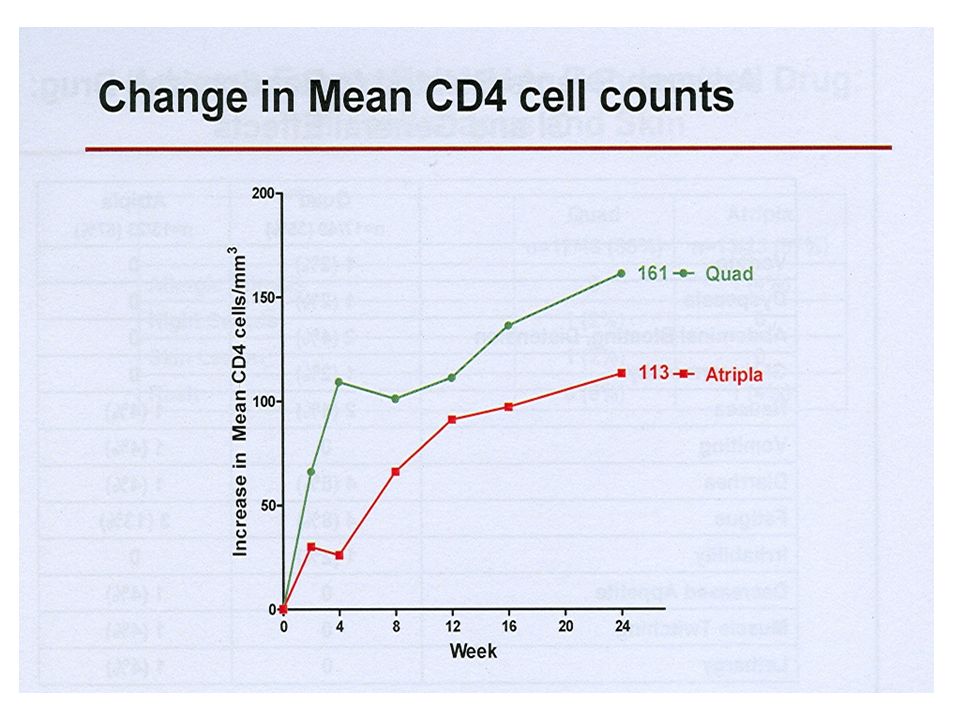
Short-term increases may be sufficient to control opportunistic infections
Battegay, Lancet 2006 3/27/2017

32
Distribution of non-AD events according to baseline CD4 counts
% of events VLP = very late presenters = CD4 < 250 LP = late presenters = CD NLP = non-late presenters = CD4 > 350

33
HIV therapy principal goals in advanced naive/AIDS presenters
AIDS reversion (in symptomatic patients) Rapid HIV/RNA decay Fast immunerecovery Block of reservoir replenishment Avoid short term toxicity
 Rapid HIV/RNA decay. Fast immunerecovery. Block of reservoir replenishment. Avoid short term toxicity.")
34
Early ART Decreases Survival in HIV+ Patients With Cryptococcal Meningitis
HIV-infected African patients diagnosed with cryptococcal meningitis randomized to receive 10 wks of fluconazole 800 mg QD + ART (n = 26) or fluconazole alone (n = 28) After 10 wks, all patients received fluconazole 200 mg QD + ART 1.00 Delayed ART 0.75 Early ART Survival 0.50 0.25 P = .028 0.00 200 400 600 800 ART, antiretroviral therapy; QD, once daily. This slide depicts the results of a similar study in HIV-infected patients with cryptococcal meningitis in Africa, where the standard of care is not amphotericin B and flucytosine as in the developed world but rather is fluconazole because of resource limitations. Mortality in HIV-infected patients with cryptococcal meningitis in this region is considerably higher than in developed nations. This may be partly because of the lack of amphotericin B and flucytosine therapy and partly because patients are presenting and being diagnosed later and receiving less supportive care during the course of therapy. This study included 54 HIV-infected patients, a relatively small number, who were diagnosed with cryptococcal meningitis and were randomized to receive an initial 10 weeks of fluconazole at 800 mg daily either with or without antiretroviral therapy. Treatment was initiated within the first several days of diagnosis and after 10 weeks of randomized treatment, all patients received fluconazole plus antiretroviral therapy. The curves on this slide reveal that there was a markedly increased risk of mortality, reaching 87% after 2 years of follow-up, among patients who received antiretroviral therapy within the first few days of starting fluconazole vs those who deferred HIV-1 treatment for 10 weeks. This was a dramatic finding: Mortality was high in both groups but much higher in those who started antiretroviral therapy earlier. The presenter speculated on the explanations for this outcome. It is certainly conceivable that early antiretroviral therapy was associated with an increased incidence of IRIS and that the mortality may have been even higher in this setting because of the inability to manage complications such as increased intracranial hypertension. However, the investigators were not able to specify how many patients died with IRIS. Other possibilities included unexpected drug‑drug interactions since patients in this study received a regimen, which included nevirapine and fluconazole, that has been shown to increase nevirapine levels. Although the reason for the outcome of this study is not clear, it appears that initiation of antiretroviral therapy within the first few days of treating cryptococcal meningitis with fluconazole is associated with a markedly increased risk of mortality. Time to Death (in Days) After 2 yrs of follow-up: 23 deaths in early ART group (87% mortality rate) vs 9 deaths in delayed ART group (37% mortality rate) (P = .002) Median survival, early ART vs delayed ART: 35 vs 274 days (P = .028) Makadzange AT, et al. CROI Abstract 36cLB. Graphic reproduced with permission. 34
 or fluconazole alone (n = 28) After 10 wks, all patients received fluconazole 200 mg QD + ART Delayed ART Early ART. Survival P = ART, antiretroviral therapy; QD, once daily. This slide depicts the results of a similar study in HIV-infected patients with cryptococcal meningitis in Africa, where the standard of care is not amphotericin B and flucytosine as in the developed world but rather is fluconazole because of resource limitations. Mortality in HIV-infected patients with cryptococcal meningitis in this region is considerably higher than in developed nations. This may be partly because of the lack of amphotericin B and flucytosine therapy and partly because patients are presenting and being diagnosed later and receiving less supportive care during the course of therapy. This study included 54 HIV-infected patients, a relatively small number, who were diagnosed with cryptococcal meningitis and were randomized to receive an initial 10 weeks of fluconazole at 800 mg daily either with or without antiretroviral therapy. Treatment was initiated within the first several days of diagnosis and after 10 weeks of randomized treatment, all patients received fluconazole plus antiretroviral therapy. The curves on this slide reveal that there was a markedly increased risk of mortality, reaching 87% after 2 years of follow-up, among patients who received antiretroviral therapy within the first few days of starting fluconazole vs those who deferred HIV-1 treatment for 10 weeks. This was a dramatic finding: Mortality was high in both groups but much higher in those who started antiretroviral therapy earlier. The presenter speculated on the explanations for this outcome. It is certainly conceivable that early antiretroviral therapy was associated with an increased incidence of IRIS and that the mortality may have been even higher in this setting because of the inability to manage complications such as increased intracranial hypertension. However, the investigators were not able to specify how many patients died with IRIS. Other possibilities included unexpected drug‑drug interactions since patients in this study received a regimen, which included nevirapine and fluconazole, that has been shown to increase nevirapine levels. Although the reason for the outcome of this study is not clear, it appears that initiation of antiretroviral therapy within the first few days of treating cryptococcal meningitis with fluconazole is associated with a markedly increased risk of mortality. Time to Death (in Days) After 2 yrs of follow-up: 23 deaths in early ART group (87% mortality rate) vs 9 deaths in delayed ART group (37% mortality rate) (P = .002) Median survival, early ART vs delayed ART: 35 vs 274 days (P = .028) Makadzange AT, et al. CROI Abstract 36cLB. Graphic reproduced with permission. 34.")
35
Advanced HIV disease with low CD4 T cells count and
high pathogen endemicity are well-known risk factors for IRIS Advanced HIV disease with low CD4 T cells count and high pathogen endemicity are well-known risk factors for IRIS. Due to very low CD4 T cell counts, CD4- and/or CD8-mediated cellular immune responses are likely to be strongly impaired and defence inflammatory reactions may not develop. Consequently, the threshold for clinically manifested disease is not crossed. Following ART initiation, viral load rapidly decreases and cellular immune functions improve within days or weeks, leading to an increased pathogen-specific immunity, which becomes apparent as an inflammatory reaction. Of course, such a reaction is recognizable only if a pathogen is present. Battegay M et al. J. Antimicrob. Chemother. 2008;62:41-44

36
Persone che scoprono di essere HIV positive alla diagnosi di AIDS: uso di terapie antiretrovirali e regime terapeutico pre-AIDS

37
V LP e regime terapeutico iniziale
%

38
Poor Initial CD4+ Recovery With Antiretroviral Therapy Prolongs Immune Depletion and Increases Risk for AIDS and Non-AIDS Diseases Baker at al., JAIDS 2008;48:541 3/27/2017

39
CD4 recovery is greater in patients treated with PI/r and without HCV infection
Castagna, Antiviral Ther 2010;15:165 3/27/2017

40
The new classes of drugs could help us to ameliorate results of therapy in AIDS presenters or advanced naive patients? Consider Rapid decay of viral load Short term tolerability Good DDI More evident immunereconstitution

44
Cost of care after HIV diagnosis, Canada
25000 20000 Mean cost (C$) 15000 CD4 < 200 CD4 > 200 10000 In questa diapositiva, che si riferisce ad uno studio canadese, sono riportati i costi dei diversi tipi di attività assistenziale per i pazienti stratificati a seconda di un numero di CD4 superiore (barre verdi) o inferiore (barre azzurre) a 200. In generale, in tutti i casi, i bassi livelli di CD4 coincidono con costi più elevati. 5000 <1 year >1 year <1 year >1 year <1 year >1 year <1 year >1 year Total Inpatient Outpatient ARV drugs Gill WJ, Krentz HB. Poster 12C th European AIDS Meeting, Madrid, October, 2007 44
 CD4 < 200. CD4 > In questa diapositiva, che si riferisce ad uno studio canadese, sono riportati i costi dei diversi tipi di attività assistenziale per i pazienti stratificati a seconda di un numero di CD4 superiore (barre verdi) o inferiore (barre azzurre) a 200. In generale, in tutti i casi, i bassi livelli di CD4 coincidono con costi più elevati <1 year. >1 year. <1 year. >1 year. <1 year. >1 year. <1 year. >1 year. Total. Inpatient. Outpatient. ARV drugs. Gill WJ, Krentz HB. Poster 12C th European AIDS Meeting, Madrid, October,")
45
cART in late presenters: features
Pros AIDS/Symptoms recovery Patients compliance Patients motivations Cons Therapy of associated pathologies High risk of mortality or fast progression Patients depression Drug convenience …….and finally lack of data …….

Similar presentations