Download presentation
Presentation is loading. Please wait.

1
Physical Assessment of the Newborn

2
Assessment Two fundamental types of exams Periodic comprehensive exam
Problem specific exam

3
Assessment Gathering accurate, detailed data that includes four components Review history Review results of physical exam Review available data Formulating an impression and plan

4
Comprehensive History
Prerequisite for adequate assessment Alerts examiner to potential problems and may indicate the need for more frequent exam Gives clues to potential pathology

5
Medical History Demographics Past Maternal illness & surgeries
Maternal conditions Family History of congenital conditions Reproductive Hx Antepartum Hx Intrapartum Hx Social Hx

6
Prenatal Factors Affecting the Newborn
Diabetes Mellitus Hyperthyroid PKU Systemic Lupus Erythematosus Hypertension Smoking & substance abuse

7
Principles of Physical Assessment
Assess infant for clues for potential pathology Auscultate in a quiet environment Keep the infant WARM & calm during the exam Handle gently! Record & report abnormalities

8
Refresh your anatomy

11
Techniques of Physical Assessment
Observation / Inspection Palpation Percussion Auscultation Inspection Auscultation Palpation Percussion

12
Inspection / Observation
Most important technique to master Alerts examiner to areas needing more thorough assessment General / Visual Auditory Olfactory

13
Palpation Using the sense of touch Superficial Deep

14
Percussion The body’s structures differ in density.
To discern the location, size and density of a structure. Tympany Resonance Hyperresonance Dullness

15
Percussion techniques
Direct Indirect Blunt Not use frequently in the neonate

16
Auscultation Listening to sounds produced by internal body structures
Indirect - using the appropriate stethoscope Direct - audible

17
Order of Examination General observation Head and neck region Facies
Nose Mouth Ears

18
Order of Examination Trunk Cardiopulmonary systems Abdomen Back
Genitalia and rectum

19
Order of Examination Extremities Neurologic exam Eye Exam

20
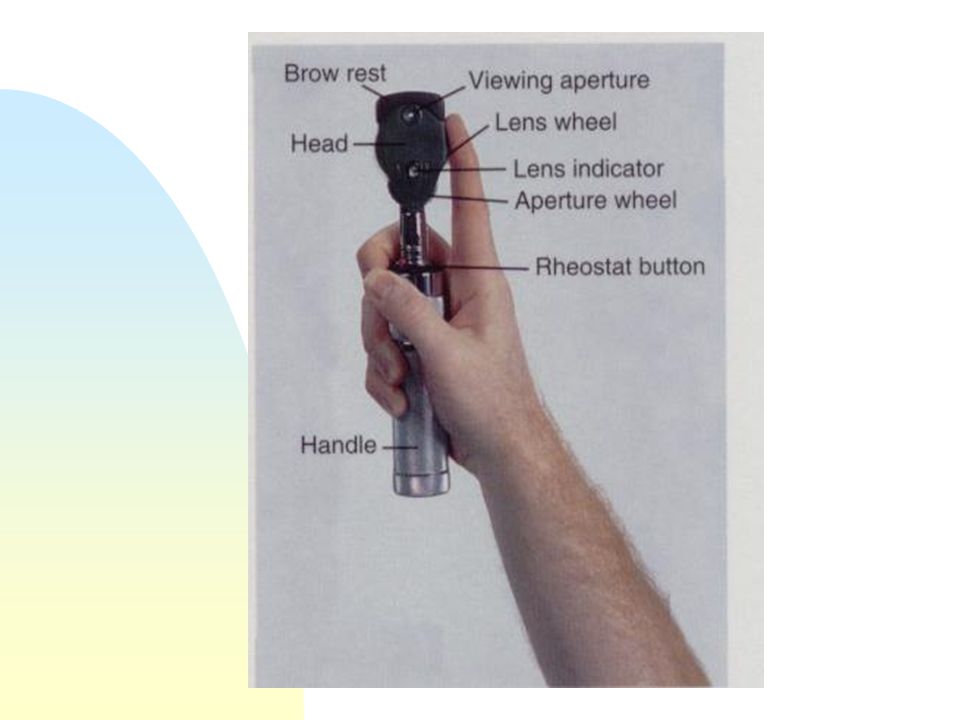
Equipment Ophthalmoscope Stethoscope Otoscope Transilluminater

22
1958 1 2 1 min 5 min APGAR Activity (Muscle tone) Pulse (HR)
1 2 1 min 5 min Activity (Muscle tone) Floppy Some flexion Well Flexed Pulse (HR) <100 >100 Grimace (reflex irritability) No response Grimace Cough or sneeze Appearance (Color) Blue or pale Pink AC Pink all over Respirations Absent Slow, irregular, weak cry Good, strong cry 1958
 Floppy. Some flexion. Well Flexed. Pulse (HR) <100. >100. Grimace (reflex irritability) No response. Grimace. Cough or sneeze. Appearance (Color) Blue or pale. Pink AC. Pink all over. Respirations. Absent. Slow, irregular, weak cry. Good, strong cry")
23
Baby A Born SVD to a G2 P2 26yo, no complications
At 1 min: Comes out crying and vigorous but color is still blue. When you bulb syringe the baby he gets mad! At 5 min: Crying off and on, pink with blue hands and feet, good flexion, HR 140’s.

24
Baby A 8 9 1 min 5 min Activity (Muscle tone) Flexed - 2 Flexed - 2
Pulse (HR) HR> HR > Grimace (reflex irritability) Coughed with bulb - 2 Cough with bulb - 2 Appearance (Color) Blue – 0 Pink with AC - 1 Respirations Crying – 2 Crying - 2 Total 8 9
 HR> HR > Grimace (reflex irritability) Coughed with bulb - 2. Cough with bulb - 2. Appearance (Color) Blue – 0. Pink with AC - 1. Respirations. Crying – 2. Crying - 2. Total")
25
Baby B Mom 35, G1P1, PIH induction. Having “lates”, vacuum assisted delivery. At 1 min: Infant is floppy, HR 120, when you bulb syringe baby turns away, color is blue and the breathing is slow & irregular. At 5 min: There is now some flexion, HR 180, coughing, pink with AC, good breathing but not crying.

26
Baby B 4 8 1 min 5 min Activity (Muscle tone) Floppy - 0
Some flexion - 1 Pulse (HR) Grimace (reflex irritability) Turns away from bulb - 1 Coughs - 2 Appearance (Color) Blue - 0 Blue with AC - 1 Respirations Slow, irregular - 1 Good, not crying - 2 Total 4 8
 Grimace (reflex irritability) Turns away from bulb - 1. Coughs - 2. Appearance (Color) Blue - 0. Blue with AC - 1. Respirations. Slow, irregular - 1. Good, not crying - 2. Total")
27
Apgar score may be influenced by
Preterm birth Administration of maternal drugs Congenital anomalies

28
Before leaving the DR Inspect for birth injuries/anomalies
Evaluate pulmonary & cardiovascular stability Inspect extremities Inspect genitalia

29
Evaluating Transition

30
Transition requires significant adjustments to tolerate the relatively stable fluid filled environment where nutrition and respiration are provided through the placenta and amniotic fluid to an environment where the newborn is physiologically independent in a few hours

32
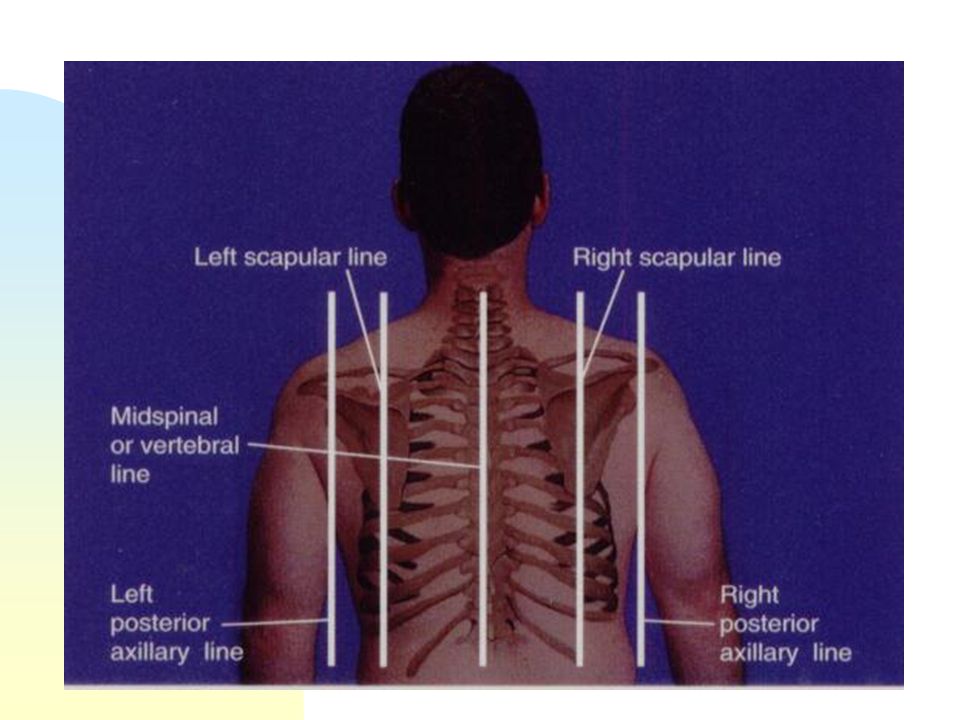
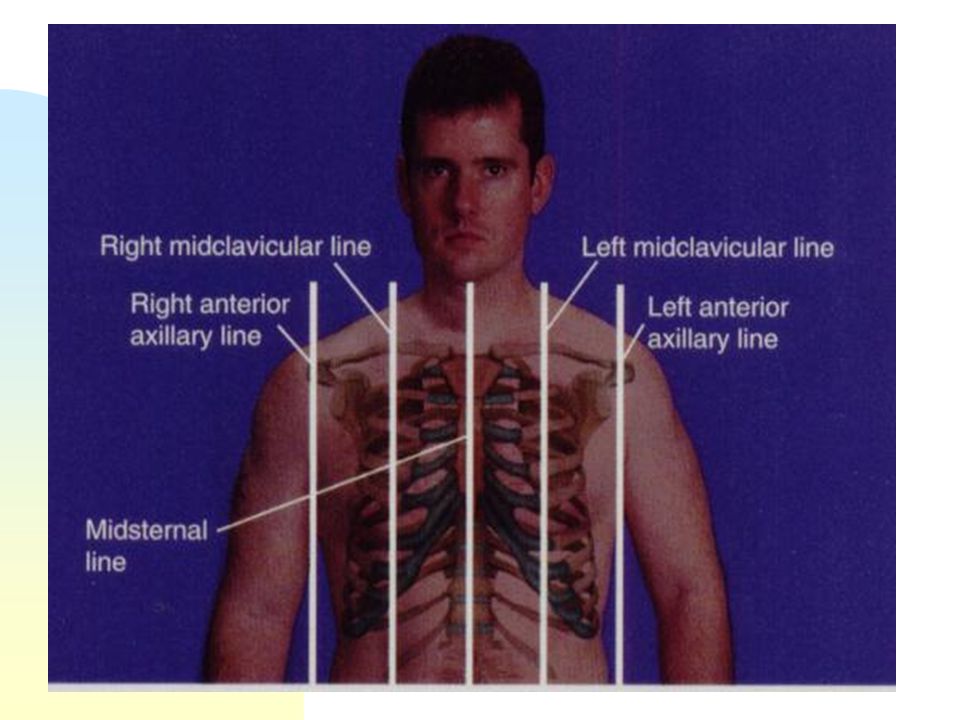
Circulation changes from fetal to neonatal routes
Brief period when oxygen saturation of the blood going to the head, upper body, and right arm are significantly higher than the lower body Line of demarcation across the chest

33
Evaluating Transition
Auscultate the chest - Is there sufficient air exchange? Evaluate the cry - Describe the quality of the cry. Lusty or weak? Is there an obstruction or narrowing of the airway? Is the infant vigorous? What is the perfusion, oxygenation and appropriateness of state?

34
Evaluating Transition
Term newborns generally complete transition in a few hours Premature infant take a longer period of time to complete transition and may require external assistance to complete the process

35
Evaluating Transition
Monitor vital signs Observe general alertness Color Signs of respiratory distress Cardiac rhythm and rate Ability to suck and swallow Handling of secretions

36
Erythema neonatorum Blushed or bright red color Few hours after birth
Last several minutes to an hour Signals the successful completion of fetal to neonatal transition of the cardiopulmonary system

37
Three particular observations are reassurances of a healthy baby
Normal variations in behavior state Comfortable respiratory effort with intermittent vigorous cry Transitional blush or erythema neonatorum

38
Periods of Reactivity Sympathetic activity Color Respiration
Heart Rate Behavioral state Gastrointestinal function Temperature

39
Periods of Reactivity Initial Period of reactivity (birth to 30 min)
Period of relative inactivity (30 m -2 hours after) Second period of reactivity (2-6 hours after) Stability period (6-24 hours) Actual times vary by baby, but there should always be a pattern of activity/sleep/activity. The presence of periods of reactivity indicate a positive adjustment to extrauterine life
 Second period of reactivity (2-6 hours after) Stability period (6-24 hours) Actual times vary by baby, but there should always be a pattern of activity/sleep/activity. The presence of periods of reactivity indicate a positive adjustment to extrauterine life.")
40
Stimulus for breathing
Sensory Chemistry Thermal Mechanical Stimulus for breathing

41
Cardiovascular Adaptations

42
Renal Intrauterine – kidney function not essential to life
Fetal urine helps to make up amniotic fluid At birth Vascular resistance of the renal vessels decreases Increased blood flow through kidneys

43
Maintenance of Body Temperature
4/19/2017 Maintenance of Body Temperature Thermogenesis (brown fat metabolism) Can find on the body in: Intrascapular region Thorax Peri-renal area Newborn’s ability to conserve heat is lacking due to not able to shiver. Thermogenesis (heat production) basal metabolic rate, muscular activity, and chemical thermogenesis (nonshivering thermogenesis - infant uses stores of brown adipose tissue/brown fat (first appears at wks/increases until 2 to 5 wks after birth). Shivering rarely seen in newborn(if infant shivers, metabolic rate has already doubled) Convection - is the loss of heat from the warm body surface to the cooler air currents (air conditioned rooms, oxygen by masks, removal from incubator Radiation - losses occur when heat transfers from the heated body surface to cooler surgaces and objects not in direct contact with the body (walls of a room or of an incubator) Evaporation - is the loss of heat incurred when water is converted to a vapor. Newborn particularly prone to this immediately after birth when wet with amniotic fluid, and during baths. Drying is critical Conduction - is the loss of heat to a cooler surface by direct skin contact (chilled hands, cool scales, cold exam tables, and cold stethoscopes)
 Can find on the body in: Intrascapular region. Thorax. Peri-renal area. Newborn’s ability to conserve heat is lacking due to not able to shiver. Thermogenesis (heat production) basal metabolic rate, muscular activity, and. chemical thermogenesis (nonshivering thermogenesis - infant uses stores of brown adipose tissue/brown fat (first appears at wks/increases until 2 to 5 wks after birth). Shivering rarely seen in newborn(if infant shivers, metabolic rate has already doubled) Convection - is the loss of heat from the warm body surface to the cooler air currents (air conditioned rooms, oxygen by masks, removal from incubator. Radiation - losses occur when heat transfers from the heated body surface to cooler surgaces and objects not in direct contact with the body (walls of a room or of an incubator) Evaporation - is the loss of heat incurred when water is converted to a vapor. Newborn particularly prone to this immediately after birth when wet with amniotic fluid, and during baths. Drying is critical. Conduction - is the loss of heat to a cooler surface by direct skin contact (chilled hands, cool scales, cold exam tables, and cold stethoscopes)")
44
Body surface to air (drafts) Radiation
4/19/2017 Convection Body surface to air (drafts) Radiation Body surface to cooler object not in contact (cold walls or window) Evaporation Conversion of a liquid to a vapor (dry infant) Conduction Body surface to cooler object in contact with baby ( warm surface)
 Radiation. Body surface to cooler object not in contact (cold walls or window) Evaporation. Conversion of a liquid to a vapor (dry infant) Conduction. Body surface to cooler object in contact with baby ( warm surface)")
45
Cold Stress Increased Metabolic Rate Increased need for O2
Increased respiratory rate Anaerobic metabolism Metabolic Acidosis, fatigue & CV collapse

46
Observe for signs of physical abnormalities

47
Newborn Vital Signs Heart rate: Apical pulse (120-160, irregular)
RR (30 to 60, no retractions, no grunting) Temperature ( ) Blood pressure 70’s/40’s Color: centrally pink with acrocyanosis
 Temperature ( ) Blood pressure 70’s/40’s. Color: centrally pink with acrocyanosis.")
48
Signs of Distress Increased respiratory rate (tachypnea)
Difficult respirations (dyspnea) Retractions Excessive mucous Cyanosis Facial grimacing Abdomen scaphoid or distended
 Retractions. Excessive mucous. Cyanosis. Facial grimacing. Abdomen scaphoid or distended.")
49
Silverman-Anderson Observations of synchrony in the chest & abdomen
Retractions of the lower ribs Retractions of the sternum Nasal flaring Presence & intensity of grunt on expiration 0 = no respiratory disease 10 = sever respiratory disease >7 = impending respiratory failure

50
Morley The need to relate signs & symptoms to grades of illness rather than to specific diagnoses d.t.: S/S nonspecific Diagnosis not always predictive of degree of illness Parents & practitioners can inform parents of the severity of illness even in the absence of a diagnosis

51
Evaluating Transition
Tachypnea C/S or preciptous delivery Metabolic acidosis Absence of tachypnea in the presence of cyanosis & poor air movement then it indicates inadequate respiratory drive May suggest depression from maternal drugs, stress

52
Remember… Delay determining sex of infant until accurate assessment of ambiguity is complete Inspect the infant for major anomalies Check the umbilical cord for the presence of 3 vessels (2 arteries, 1 vein)
")
53
Remember... Establish patency of upper airway
A term fetus swallows 450ml of amniotic fluid/day. Gastric emptying at 20 ml/hr. Aspirated gastric contents >15 ml is increased > 25ml is abnormal and suggests obstruction at the pylorus or duodenum

54
Remember... May be green-brown in color(old swallowed meconium), or blood Blood may be fetal or maternal APT test can distinguish Don’t forget to look at the back Check that the palate is intact Look for the anus! Is there an opening?

55
Before leaving DR Inspect for birth injuries Congenital anomalies
Evaluation of pulmonary & cardiovascular stability Extremities Genitalia

56
Facilitate Infant’s Relationship with Parents

57
Newborn Care to Prevent Complications
Vitamin K, Eye prophylaxis, & glucose evaluation Medves, Jennifer. (2002). Three infant care interventions: Reconsidering the evidence. JOGNN,31(5), pp
. Three infant care interventions: Reconsidering the evidence. JOGNN,31(5), pp")
58
Assessing Growth Weight, Length, Head & Chest 4/19/2017
HC cm or 13 to 14 inches Length 46 to 54 cm or inches Weight 2.5 to 3.4 kg or about 7 1/2 pounds chest 2cm or 1inch less than head Newborns are 75 t 90% fluid and may lose up to % of birthweight, should regain by days of age Weight, Length, Head & Chest

59
Assessing Growth A normal growth pattern is an indicator of fetal and neonatal well-being. Growth follows a predictable path Influenced by genetic and environmental patterns May be proportionate or disproportionate

60
Assessing Growth Standard measurements are head circumference, height and weight Compare the individual to himself over time by looking at the rate of growth or the expected pattern of an infant of similar characteristics Validity & Reliability of measurements

61
Measurements Weight Length Head Circumference Chest Circumference
Abdominal Circumference

62
Gestational Age Assessment

63
Gestational Age Assessment: Estimating post-conceptual age of the neonate
An accurate assessment of age is important for 2 reasons Age and growth patterns appropriate to that age aid in identifying neonatal risks Help in developing management plans

64
Gestational Age Assessment
There are 3 general methods to determine gestational age Calculation of dates based on LMP Evaluation of obstetrical patterns Physical exam of the neonate

65
Gestational Age Assessment
Physical Assessment Assessment of anterior vascular lens capsule using opthalmoscope Best done on the 2nd day of life Assessment of neuromuscular and physical criteria by inspection and palpation

66
Assessment of the Anterior vascular lens capsule

67
Grade 4, 27 – 28 wks

68
Grade 3, 29 – 30 wks

69
Grade 2, 31 – 32 wks

70
Grade 1, 33 – 34 wks

71
Modified Ballard

72
Plotting Weight, Length, HC

73
Pre-term: born before end of 37th week gestation

74
Term

75
AGA

76
SGA: < 10th %

77
LGA: >90th%

78
Post term: Born after the 42nd week of pregnancy

79
Low birth weight: g

80
Very Low Birth weight: 1000-1500g

81
Extremely very low birthweight: 500-1000g

82
Skin

83
Lanugo

84
Plantar creases

85
Ear cartilage

86
Genitalia

87
Neuromuscular Criteria
Posture Observe in the supine position Score is assigned based on the degree of flexion of arms, knees and hips Increased flexion and hip adduction with increased gestational age

88
Neuromuscular Criteria
Square Window Infants hand is flexed on the forearm between the thumb and index finger of the examiner Apply enough pressure to get FULL flexion without rotating the wrist Angle between the forearm and palm is measured

89
Neuromuscular Criteria
Arm Recoil Flex the neonates arms for 5 seconds while in the supine position Fully extend the arms by pulling on the hands and release The degree of arm flexion and strength of recoil are scored

90
Neuromuscular Criteria
Popliteal Angle Place infant in supine position with the pelvis on the mattress Using the thumb and index finger of one hand, examiner holds the knee adjacent to the chest and abdomen. Gently extend the leg with the index finger Look at the angle between the lower leg, thigh and posterior knee

91
Neuromuscular Criteria
Scarf sign Place infant in supine position with head in mid-line position. Grasp the infants hand and pull the arm across the chest and around the neck. Look at the relationship of elbow to mid-line of body when arm pulls across the chest

92
Neuromuscular Criteria
Heel to ear Place the infant supine with pelvis flat on table. Grasp one foot with thumb and index finger and draw foot as near to head as possible. Note the distance between the foot and head as well as degree of knee extension

93
Physical Criteria Skin
less transparent and tougher with increasing gestational age 36-37 weeks loses transparency and underlying vessels are no longer visable Increasing gestational age the veins become less viable and increasing subcutaneous tissue

94
Physical Criteria Lunago
Fine downy hair covering fetus from weeks Disappears around face and anterior trunk ~28 weeks Term infants may have a few patches over shoulders

95
Physical Criteria Sole creases
28-30 weeks appear and cover the anterior portion of of the plantar surface of the foot Extend toward the heel as increases gestational age After 12 hours sole creases are not valid indicator of gestational age due to drying of the skin

96
Physical Criteria Breast tissue and aerola
Aerola is raised by 34 weeks A 1-2 mm nodule of breast tissue is palpable by 36 weeks By 40 weeks the nodule is 10mm

97
Physical Criteria Ears
Incurving of the upper pinna begins by 34 weeks gestation and extend entire lobe by 40 weeks Before 34 weeks, pinna has very little cartilage (Stays folded on itself) At 36 weeks, there is some cartilage and will spring back
 At 36 weeks, there is some cartilage and will spring back.")
98
Physical Criteria Female Genitalia
Early gestation, clitoris prominent and widely separated labia By 40 weeks, fat deposits have increased in size in labia majora so labia minora are completely covered

99
Physical Criteria Male genitalia
Testes begin to descend from abdomen around 28 weeks At 37 weeks, testes can be palpated high in scrotum At 40 weeks, testes are completely descended and covered with rugae As gestation progresses, scrotum becomes more pendulous

100
CANSCORE Nine signs for assessing nutritional status in term infants
4/19/2017 CANSCORE Nine signs for assessing nutritional status in term infants Hair Cheeks Chin & neck Arms Back Buttocks Legs Chest Skin on Abdominal wall

101
4/19/2017 CANSCORE, Fletcher, p34 Nine signs for assessing nutritional status in term infants Hair Cheeks Chin & neck Arms Back Buttocks Legs Chest Skin on Abdominal wall

102
4/19/2017 Cheeks from full buccal pads & rouind face to narrow, flat face Neck & chin from double or triple chin fat folds, neck not evident to thin chin, no fat folds, neck with loose, wrinkled skin easily evident.

103
Assessing Growth Normal growth pattern Follows a predictable path
Influenced by genetic & environmental patterns Compare individual to himself over time.

104
Quiet Sleep

105
Active Sleep

106
Drowsy

107
Quiet Alert

108
Active Alert

109
Crying

110
State Related Behaviors
Visual responses Auditory responses Motor behavior Smile Habituation Consolability Cuddliness Readability

Similar presentations
















) p. 201- 206 By : Mohammad Abuadas RN, MSN.>")



