Download presentation
Presentation is loading. Please wait.

1
CHEST TRAUMA Dr.mohammadzadeh Thorasic surgeon

2
Incidence Trauma kills 150,000 Americans every year. It is the most common cause of death in the population <40 years of age. One-fourth of deaths are specifically related to chest trauma,many of them occurring in the prehospital setting.

3
Specific Physical Findings in Chest Trauma

4
Subcutaneous emphysema

5
Traumatic Asphyxia

6
Theory of mechanism

7
Thoracic cage injuries

8
Sternal Fracture

10
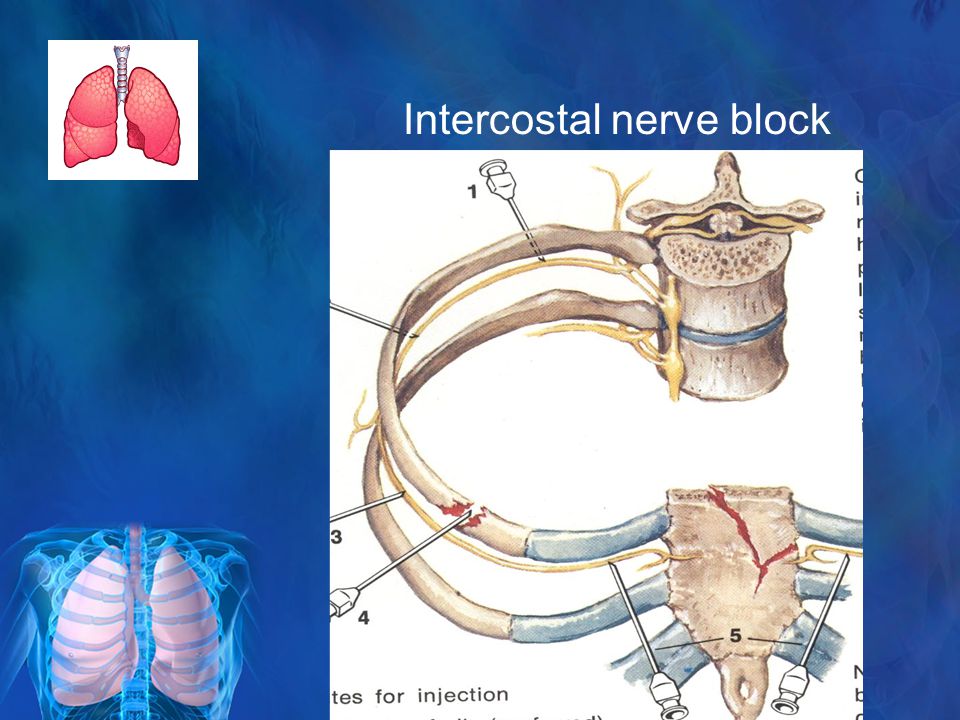
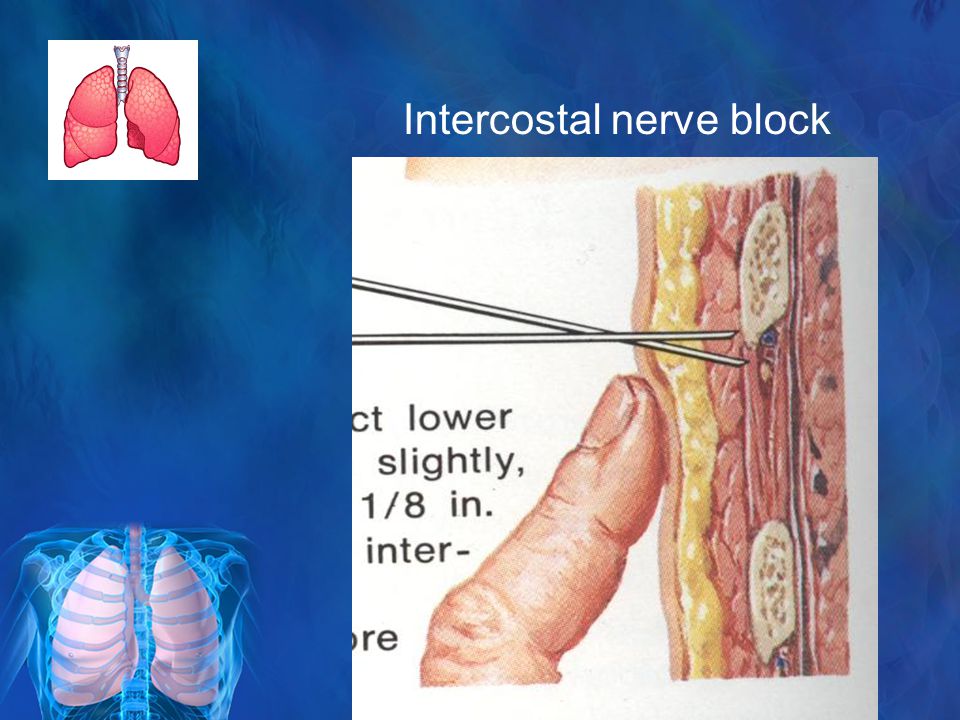
Intercostal nerve block

13
Flail chest

14
Complete sternochondral separation

15
Flail chest

16
Penetrating chest injuries 1.Pneumothorax simple p. tension p. open p. 2.Hemothorax 3.Pulmonary hematoma 4.Major pulmonary paranchymal inj. 5. Air embolism 6.Traumatic lung herniation 7.Diaphragmatic injury

17
Simple Pneumothorax may not come to the attention of the clinician during the initial assessment of critically injured victims. A chest radiograph should always be obtained as early as possible during the secondary survey., chest tube drainage is recommended, even for small collections of air, especially in patients who require positive-pressure ventilation.

18
When a large air leak is present or reexpansion of the lung is incomplete, a tracheobronchial injury should be suspected and prompt flexible bronchoscopy performed

19
Pneumothorax

20
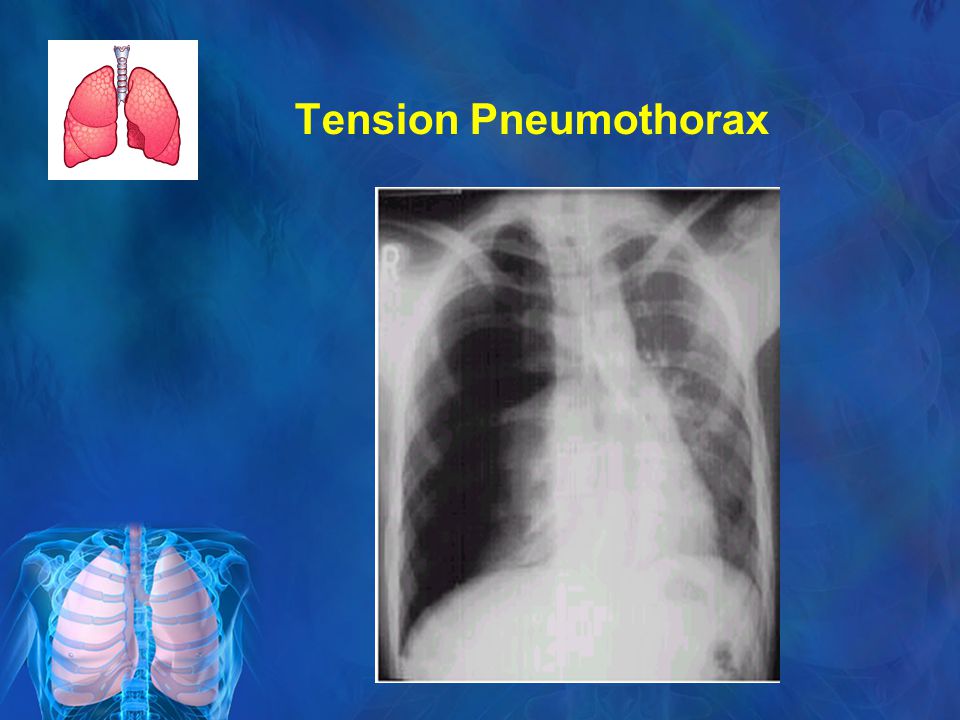
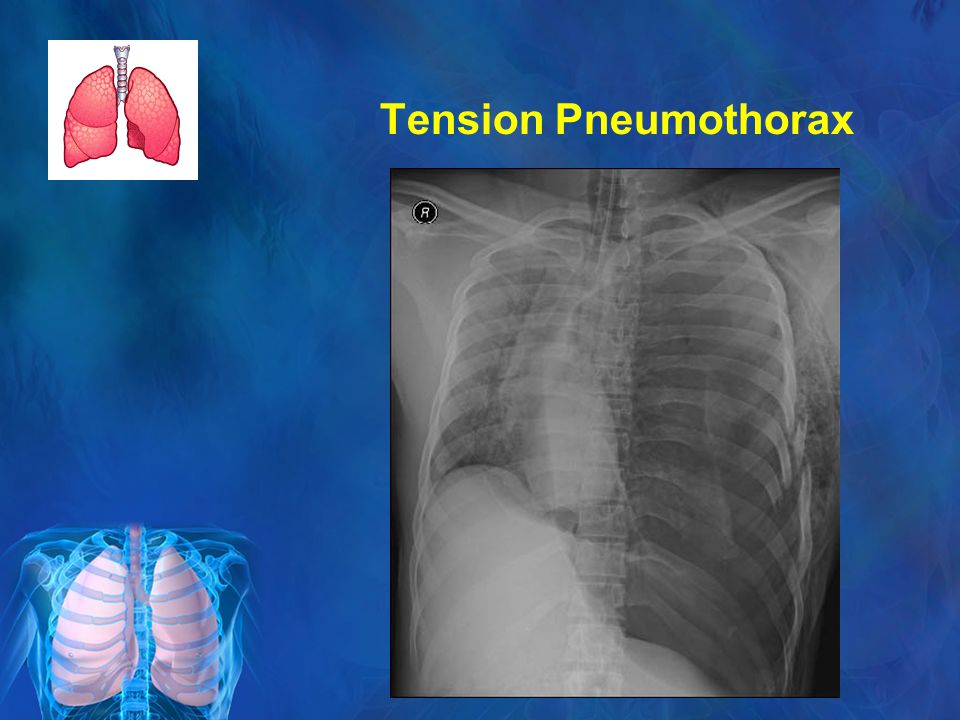
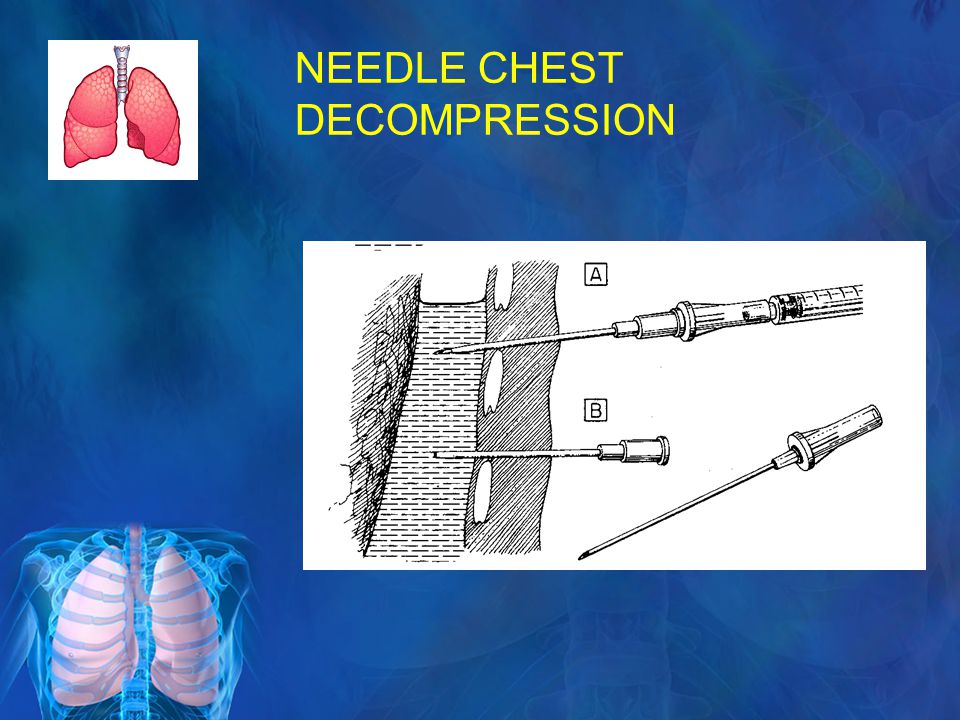
Tension Pneumothorax Physical examination is more dramatic and may demonstrate severe respiratory distress, distended neck veins, deviated trachea, absent breath sounds, or tympany to percussion on the affected side

21
Signs and Symptoms of Tension Pneumothorax Anxiety, agitation, and apprehension Diminished or absent breath sounds Cyanosis Rapid shallow breathing Distended neck veins

22
Tension Pneumothorax

25
NEEDLE CHEST DECOMPRESSION

28
Open Pneumothorax (( sucking chest wounds Result of full-thickness loss of a portion of the chest wall, usually from a gunshot wound A life-threatening emergency. Air can flow freely in and out of the pleural space

29
Open Pneumothorax

31
Open(Sucking) Pneumothorax
 Pneumothorax")
32
Open Pneumothorax

33
Flutter-Valve Seal

34
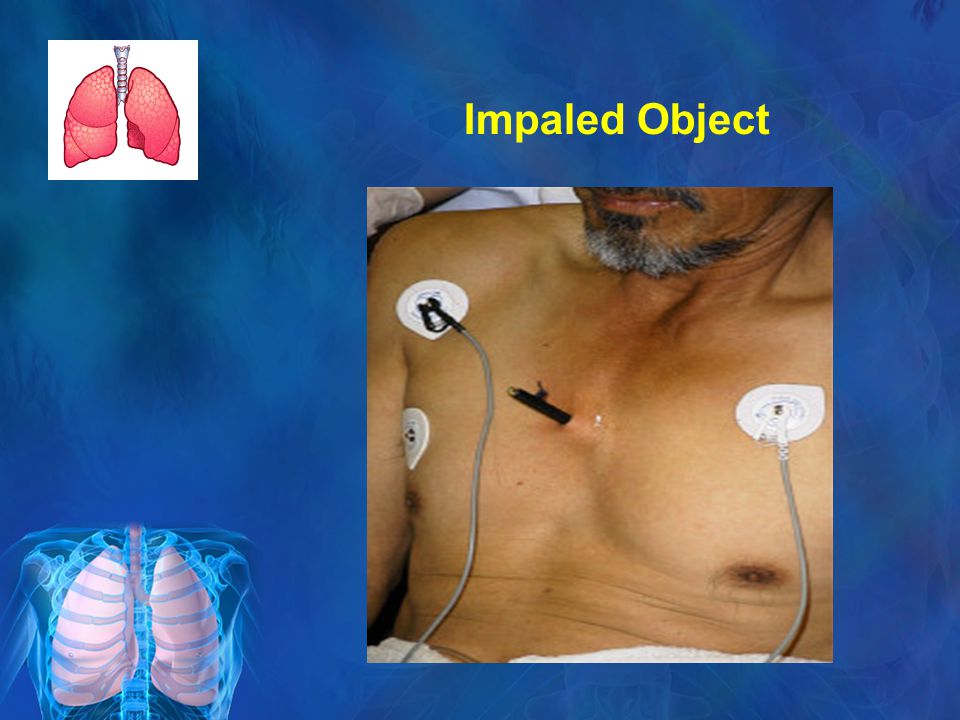
Impaled Object

37
Asherman chest seal

38
Treatment Asherman chest seal – convert sucking chest wounds to simple pneumo/hemothorax

39
Hemothorax Often associated with penetrating chest injury or chest wall blunt trauma with bony injury. Ultrasound can be rapidly performed by the surgeon carrying out the initial evaluation of the injured patient. A slight reverse Trendelenburg position of the patient is helpful in identifying smaller hemothoraces More commonly, a hemothorax is recognized on chest radiography

40
Sources of Hemothorax

41
Degree of Hemothorax

42
Hemothorax

44
Management Complete evacuation of the blood collection. Intrathoracic bleeding recognized in the emergency department requires a closed- tube thoracostomy. Most commonly, a 24- or 28-Fr thoracostomy tube is sufficient to accomplish this goal.

45
ATLS criteria Chest drainage >1,500 mL initial or >250 mL/hr for the next 4 hours

46
Residual Hemothorax Must be evacuated as soon as the patient is stable to reduce the risk for empyema or prevent the formation of a fibrous peel (resulting in lung entrapment). It is not an emergency situation if bleeding has stopped. Thoracoscopic drainage is best performed within 1 to 3 days after injury

47
Rupure of trachea or bronchi

48
Small tear of membranous portion of r. main bronchus

49
Almost complete rupture of thoracic trachea

50
Complete rupture of cervical trachea

51
Diaphragmatic injury

52
Thoracoabdominal stab wounds : anterior : 4 th intercostal space laterally : 6 th intercostal space posteriorly : 8 th intercostal space DPL : an RBC count > 10000 laparatomy an RBC count > 1000 thoracoscopy THORACOSCOPY

53
Diaphragmatic injury

54
Pulmonary contusion

55
Symptoms & Signs

56
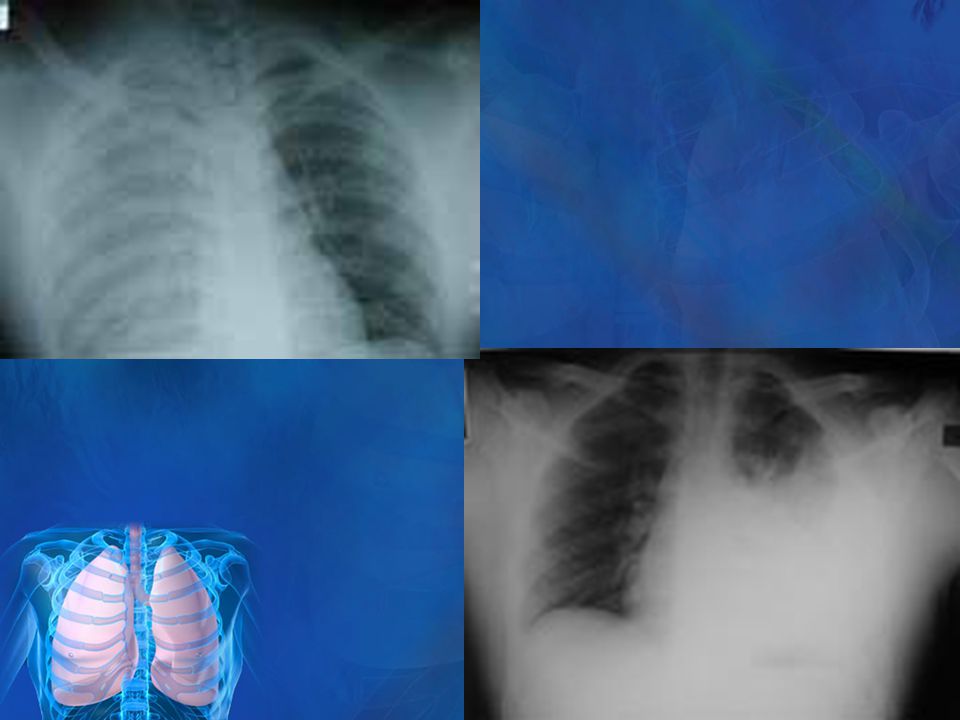
Ill-defined patchy densities scattered throughout the lung

57
Pulmonary contusion

58
Pathology

59
Pulmonary Hematoma Difficult to differentiate from pulmonary contusion because of the surrounding intraparenchymal hemorrhage. 24 to 48 hours after the injury, a hematoma typically develops into a discrete mass with distinct margins. CT scans can be helpful in distinguishing between contusion and hematoma.

60
In most cases, the hematoma itself does not interfere with gas exchange and is reabsorbed in time. Rarely such a hematoma become secondarily infected and present as an abscess requiring drainage

61
Major Pulmonary Parenchymal Injury Most pulmonary parenchymal injuries are treated with chest tube drainage. Indication for thoracotomy : Radiographic assessment Bronchoscopy Patient's hemodynamic status, Adequacy of lung expansion, Size of air leak, Chest tube output

62
Surgery The most effective method is the nonanatomic stapled resection. More proximal lesions require extensive resection, including lobectomy or pneumonectomy. Anatomic resections are rarely indicated Tractotomy was first described by Wall in 1994

63
Tractotomy

64
Pulmonary tractotomy

65
Air Embolism Air embolism was first reported in 1974 by Thomas and Stevens in patients with penetrating lung injury. It is typically seen in patients with penetrating injuries to the hilum of the lung, where the veins are not surrounded by lung or other structures. Even small amounts of air can be catastrophic, resulting in hemodynamic instability with ventricular fibrillation and seizure activity.

66
Air embolism is difficult to recognize. It may present as sudden cardiovascular collapse and sudden death in the conscious patient and must be suspected in patients who present with pulseless electrical activity. When endotracheal pressure is >60 mm Hg, gas will easily pass from the pulmonary venous system into the systemic circulation and embolize in the coronary arteries.

67
The hallmark of an air emblus is hemoptisis and bloody,frothy air leak from a lung injury

68
Management Immediate thoracotomy Clamping of hilum Head down position De-airing of left ventricular apex with a large –gauge needle

69
Traumatic Lung Herniation Historically, noncongenital lung herniations resulted from penetrating traumatic injuries, including postsurgical incisional herniations. Today, the most common cause of lung herniation is motor vehicle collisions, particularly in restrained passengers. Other reported herniation sites include the site of internal mammary artery harvest, port sites after minimally invasive coronary bypass procedures, thoracoscopy port sites, through tube thoracostomy drainage sites. Symptoms may be minimal despite a localized bulge that paradoxically changes shape with the respiratory cycle.

70
Lung Herniation

72
Treatment Treatment involves hernia reduction and defect closure with a prosthetic patch (such as polytetrafluoroethylene). The results are frequently excellent.

73
QUESTIONS?

Similar presentations










, FCCP>")













