Download presentation
Presentation is loading. Please wait.

1
Magee-Womens Hospital of UPMC
HER2 Immunohistochemistry: Workflow Experience with Image Analysis Based Interpretation of CB11 and 4B5 Clones Jeffrey Fine MD, Rohit Bhargava MD, Urvashi Surthi PhD, and David Dabbs MD Magee-Womens Hospital of UPMC

2
Disclaimer One of the abstract authors (David Dabbs) is a consultant for Ventana None of the other authors have any conflicts of interest to report

3
Objectives Overview of Her2/NEU testing (IHC)
Recap of validation results Discuss implementation of image analysis

4
Her2/NEU Test for responsiveness to Trastuzumab (Herceptin)
Trastuzumab is cardiotoxic and is very expensive False positives are highly undesirable Trastuzumab can increase survival or reduce risk of recurrence False negatives are also undesirable

5
CAP HER2-A Survey (Spring 2007)
40 TMA cores (4 slides) Stained/interpreted at institutions (350ish) Consensus (>80%) in 22 of 40 cases Very variable
 Stained/interpreted at institutions (350ish) Consensus (>80%) in 22 of 40 cases. Very variable.")
6
IHC Variables Pre-analytic Analytic Post-analytic
Fixation issues, tissue processing Analytic Validation, Calibration, Antibody clone, Antigen retrieval, Automation, Controls, etc. Post-analytic Interpretation criteria QA procedures Image analysis (17.9% reported using it)
")
7
Validation of IA at UPMC
Formalin fixed (8-48 hours) paraffin embedded tissue Automated IHC platform (Ventana) CB11 and 4B5 antibodies (Ventana) VIAS (Ventana Image Analysis System) FISH (Vysis)
 paraffin embedded tissue. Automated IHC platform (Ventana) CB11 and 4B5 antibodies (Ventana) VIAS (Ventana Image Analysis System) FISH (Vysis)")
8
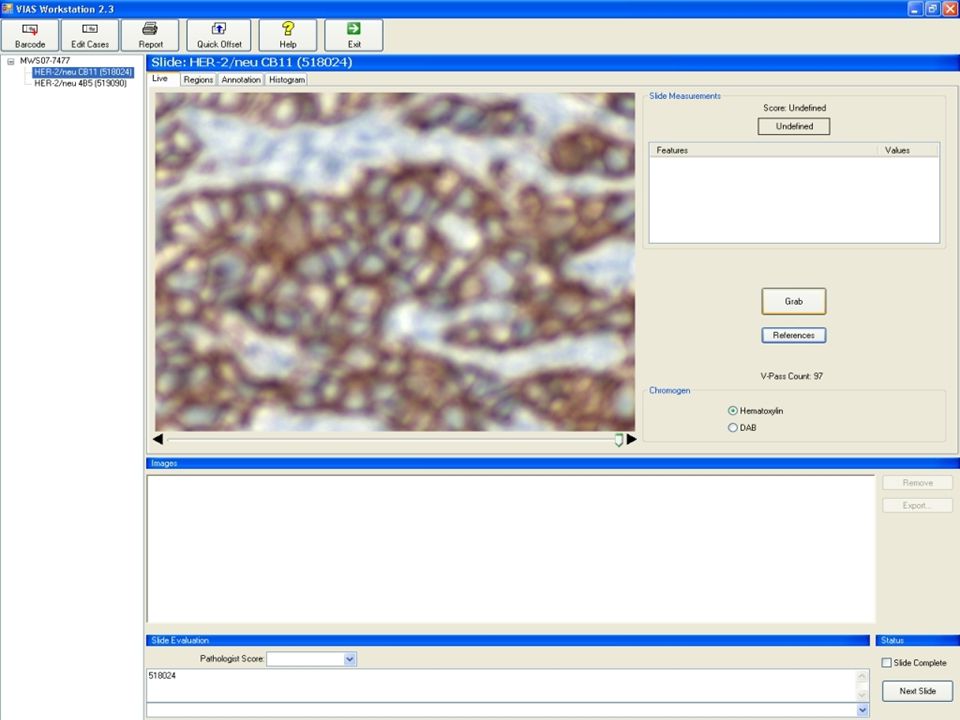
VIAS (image from vendor)
")
9
Validation Results I System differentiated between tumor and stroma (subjective impression) Pathologist had to find invasive tumor (and exclude in-situ tumor)
")
10
Classification (Tumor vs. Stroma)
")
11
Results CB11 100% Concordance with FISH (n=52) FISH rate (2+ rate):
0/1+ IHC with no amp by FISH 3+ with amp by FISH FISH rate (2+ rate): Expert 22.9% (n=118) VIAS 21.2% (expert was also 100% concordant)
: Expert 22.9% (n=118) VIAS 21.2% (expert was also 100% concordant)")
12
Results 4B5 94.6% Concordance with FISH (n=56) FISH rate (2+):
100% Concordance with new reference range FISH rate (2+): Expert 21.9% (n=114) VIAS 28.9% (n=117) *new reference range
: Expert 21.9% (n=114) VIAS 28.9% (n=117) *new reference range.")
13
Reference Range VIAS assigns a raw number score to each case which is then rounded to the nearest whole number. Out of the box—score 2.5 or higher was rounded to “3+” New range is conservative—only cases with score 3.5 are called “3+”

14
Demixed to show brown

15
Old Workflow Office Mailbox Order Her2/NEU Retrieve IHC Stain
Interpret Stain Dictate Results Sign out case Old Workflow

16
New Workflow IA Workstation Office Mailbox Order Her2/NEU Retrieve IHC
Stain Perform IA Dictate Results Sign out case New Workflow

17
Implementation Details
Billing Fee code 88361 Technical charge initiated by order in APLIS Documentation VIAS results printout retained with other case paperwork (requisition) IHC results (ER/PR and Her2/NEU) dictated into canned text that includes VIAS blurb
 IHC results (ER/PR and Her2/NEU) dictated into canned text that includes VIAS blurb.")
18
Documentation Support
Transcription New “quick text” with VIAS sentence Communication with Transcription Team Slide/paper management personnel Communication – do not discard results report Back-up of data Currently performed manually

19
“Consumables” IA charged per “click”
IHC Laboratory responsible for keeping an adequate supply of the click reagent Smart Card (100 tests) Image from nist.gov www site
 Image from nist.gov www site.")
20
Training Local Domain Expert (me) Fellows Selected Faculty
Other Faculty Residents

21
Status Report IA is in production for a week Bumps being ironed out
Transcription Training End experience varies

22
Good Should increase standardization
Recent switch to 4B5 clone – different appearance and possible differences in interpretation Documented response to pressure for accurate Her2/NEU testing Foot in the door for other IA applications Vendor has been responsive and appears to want to improve shortcomings

23
Bad IA of new antibody is less accurate than that of discontinued antibody Reference range work-around Workflow involves “travel” and is more labor intensive than traditional method Quality improvement but does not extend the pathologist Operator error is possible Data entry Lighting Focusing

25
Future IA (More Automation)
Whole Slide Images (some systems do permit IA) Slide could be scanned in the IHC lab, and results (with the electronic slide) delivered straight to the pathologist Automated detection of invasive tumor Transition of IA to non-pathologist staff Electronic interfaces to support test ordering and resulting (no more paper print outs or dictation)
 Slide could be scanned in the IHC lab, and results (with the electronic slide) delivered straight to the pathologist. Automated detection of invasive tumor. Transition of IA to non-pathologist staff. Electronic interfaces to support test ordering and resulting (no more paper print outs or dictation)")
26
Conclusions IA is validated and should improve performance of Her2/NEU IHC testing by reducing post-analytic variability Current IA set-up not ideal but an important first step: Successful implementation in a busy academic setting Revenue (digital pathology business case)
")
Similar presentations

















>")

 Lindy A. Brigham Div of Plant Pathology and Microbiology Department of Plant Sciences PLS 595D Regulatory.>")