Download presentation
Presentation is loading. Please wait.

1
Basis of Medical Cancer Therapy Rebecca Roylance Senior Lecturer in Medical Oncology

2
Background Chemotherapy Radiotherapy Endocrine Therapy Biological Therapy

3
‘Ideal’ Cancer Treatment Highly efficacious Highly tumour specific Minimal toxicity

4
Chemotherapy Efficacious 90% cure occurs in only 10% of cancers Completely non-specific Marked toxicity

5
Historical Background 1940s alkylating agents were identified as by- product of secret gas production marrow & lymphoid hypoplasia Used leukaemia/lymphomas - pub 1946 Folic acid lead to proliferation of leukaemic cells antifolates e.g. methotrexate

6
Mechanism Principle of treatment - tumour growth fraction –Malignant cells do not divide more quickly than normal cells –Bigger population of cells dividing

7
10 12 10 10 8 10 6 10 4 10 2 Time Number of cells surviving M T Fractional Cell Kill Hypothesis CCCCC

8
Classes of Drug Alkylating agents Platinum compounds Anthracyclines Antimicrotubule agents Antimetabolites Topoisomerase II inhibitors

9
G0G0 M G2G2 G1G1 S METHOTREXATE HYDOXYUREA CYTOSINE ARABINOSIDE ANTHRACYCLINES VINCA ALKALOIDS TAXANES PHASE NON-SPECIFIC Alkylating agents Cisplatin Nitrosoureas Antibiotics

10
Alkylating agents e.g. Cyclophosphamide Covalently link to structures in nuclei acids inter- or intra-DNA strand cross-linking impairs DNA replication More lethal if occurs during S-phase

11
Platinum Drugs e.g. Cisplatin, carboplatin, oxaliplatin Platinum drugs bind to DNA intra-strand cross-linking predominantly Conformational change in DNA - making repair of the damage difficult

12
Anthracyclines e.g. Doxorubicin, epirubicin, mitoxantrone Bind tightly to DNA and deform its structure Intercalate DNA causing single-stranded and double stranded breaks Produce intracellular free radicals - contribute to toxicity

13
Metaphase Anaphase Vinca alkaloids prevent microtubule assembly Taxanes prevent microtubule disassembly Mitotic block

14
Dihydrofolate reductase Dihydrofolate (FH 2 ) Tetrahydrofolate (FH 4 ) Thymidine monophosphate Deoxyuridine monophosphate METHOTREXATE Blocks here Folinic acid Bypasses block
 Tetrahydrofolate (FH 4 ) Thymidine monophosphate Deoxyuridine monophosphate METHOTREXATE Blocks here Folinic acid Bypasses block")
15
Combination Chemotherapy Only use if effective alone Non-overlapping toxicity Each drug used at optimal dose and schedule Synergistic action Different effects cell cycle

16
Uses of chemotherapy Cure –Induction –Adjuvant –Primary (neoadjuvant) Palliation
 Palliation")
17
Neoadjuvant chemotherapy Taken from Biology of Cancer

18
Clinical Trials Phase I - determine optimal dosage Phase II - assess tumour response Phase III - large randomised studies assess improvement in survival

19
Endocrine therapy Efficacious –Breast –Prostate Fairly specific Minimal toxicity

20
Historical Background 1896 case report of oophorectomy in breast cancer by Beatson Postulated a link between ovaries and proliferation of breast cells 33 yr old women lump L breast 12cm at presentation - breast removed but cancer advanced oophorectomy pt survived for further 4 years

21
Taken from BJC 2004 90(1) S2-6
 S2-6")
22
Tamoxifen 1969 development of tamoxifen as a contraceptive SERM - selective oestrogen receptor modulator 1973 licenced for use in breast cancer 1980s clinical trials demonstrated a benefit in overall survival

23
Further Oestrogen modulation Aromatase inhibitors –Steroidal e.g. exemestane –Non-steroidal e.g. arimidex Anti-oestrogen e.g. fulvestant

25
Mechanism of action of fulvestrant Taken from BJC 2004 90(1) S2-6
 S2-6")
26
Biological Therapy Efficacious –But less than expected, mechanisms not fully understood Specific Minimal toxicity cf trastuzumab (herceptin)
")
27
Biological Therapy Monoclonal antibodies Small molecule inhibitors

29
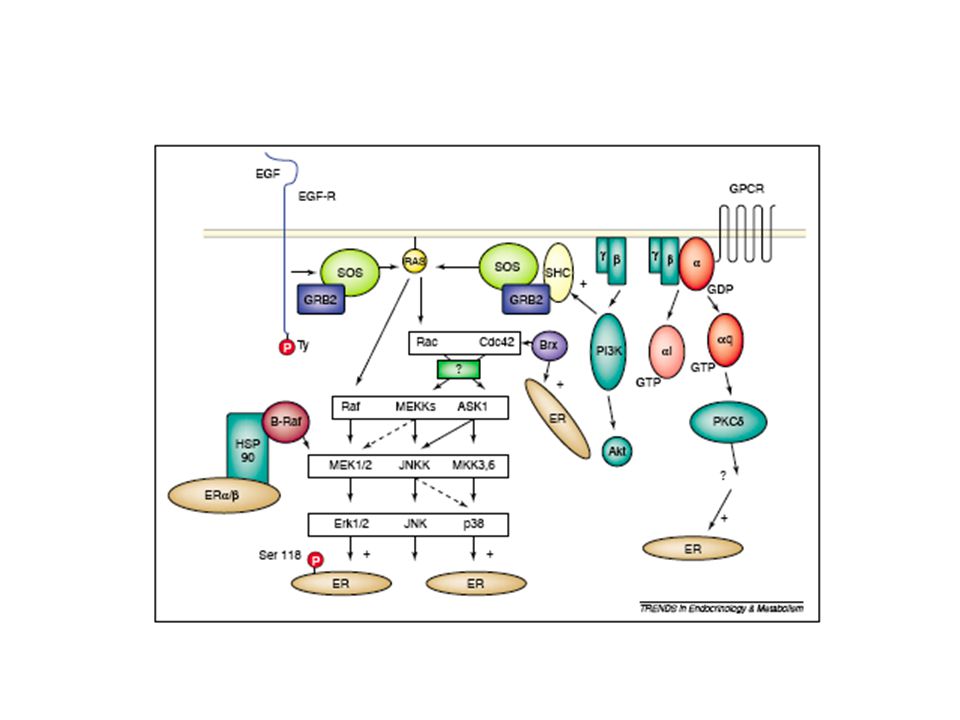
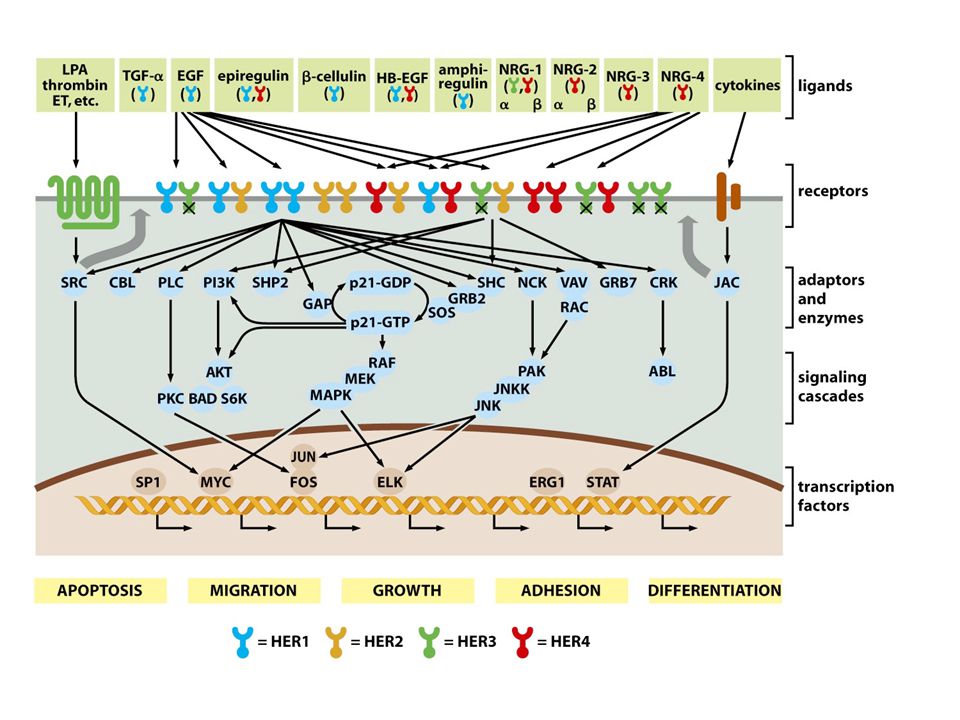
HER2/ERBB2 1987 - amplified and overexpressed in 25- 30% breast cancers Associated with poor prognosis No natural ligand Activation results in heterodimerisation Many downstream substrates

30
FISH amplification of HER2

31
HER2 IHC

32
Trastuzumab (Herceptin®) Humanised monoclonal antibody to HER2 receptor Infusion related reaction - chills, fever, rash - rarely repeated Cardiac toxicity - especially if given in association with anthracyclines ?why - cross reactivity with cardiac muscle
 Humanised monoclonal antibody to HER2 receptor Infusion related reaction - chills, fever, rash - rarely repeated Cardiac toxicity - especially if given in association with anthracyclines why - cross reactivity with cardiac muscle")
33
Clinical trials - metastatic 2001 Phase III clinical trial showed in combination with chemotherapy in metastatic setting: Improved response rate 50% vs 32% (p<0.001) Decreased one year mortality 22 vs 33% (p=0.008)
 Decreased one year mortality 22 vs 33% (p=0.008)")
34
Clinical trials - adjuvant 2006 - 4 trials >10000 women Interim analysis resulted in stopping trials early Decreased risk of relapse - 50% Survival advantage of 2.5% NEJM 2005 353 1659-72 & 1673-84

35
Other targeted monoclonal antibody therapies TargetDrugUse VEFRBevacizumabcolorectal EGFRCetuximab colorectal CD20 RetuximabB cell NHL CD52AlemtuzumabCLL HER2 Pertuzumab clinical trials

36
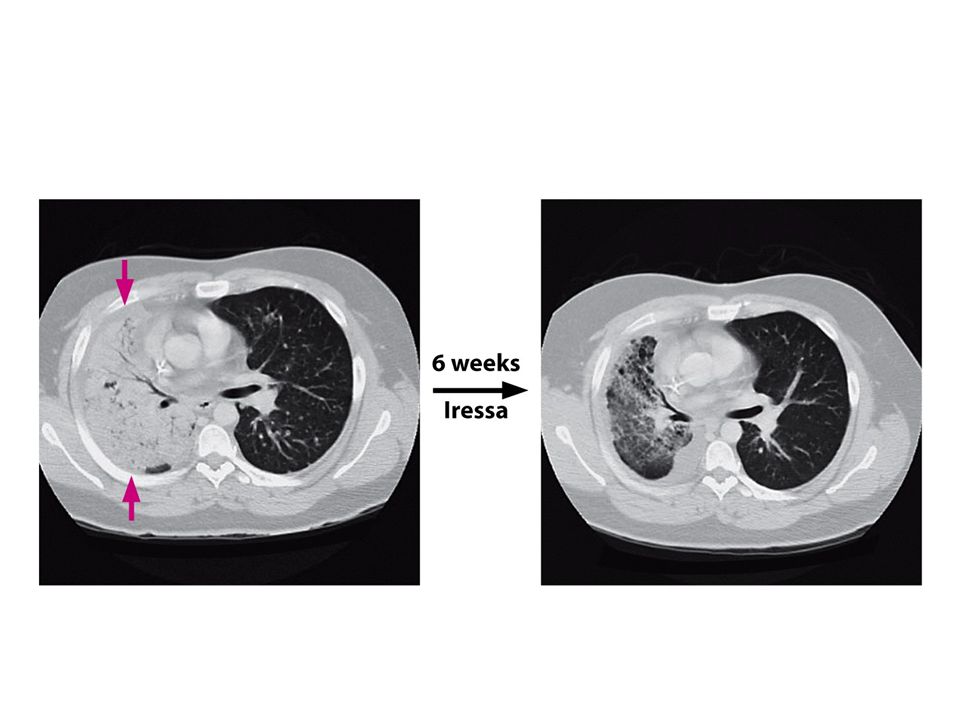
Small molecule therapy ReceptorDrugUse KITImatinib (Gleevec)GIST EGFRErlotinib (Tarceva)NSCLC Gefitinib (Iressa) NSCLC HER1,2LapatinibBreast RTKSunitinib (Sutent)RCC
GIST EGFRErlotinib (Tarceva)NSCLC Gefitinib (Iressa) NSCLC HER1,2LapatinibBreast RTKSunitinib (Sutent)RCC")
38
Imatinib (Gleevec)
")
39
GIST Pre Post

41
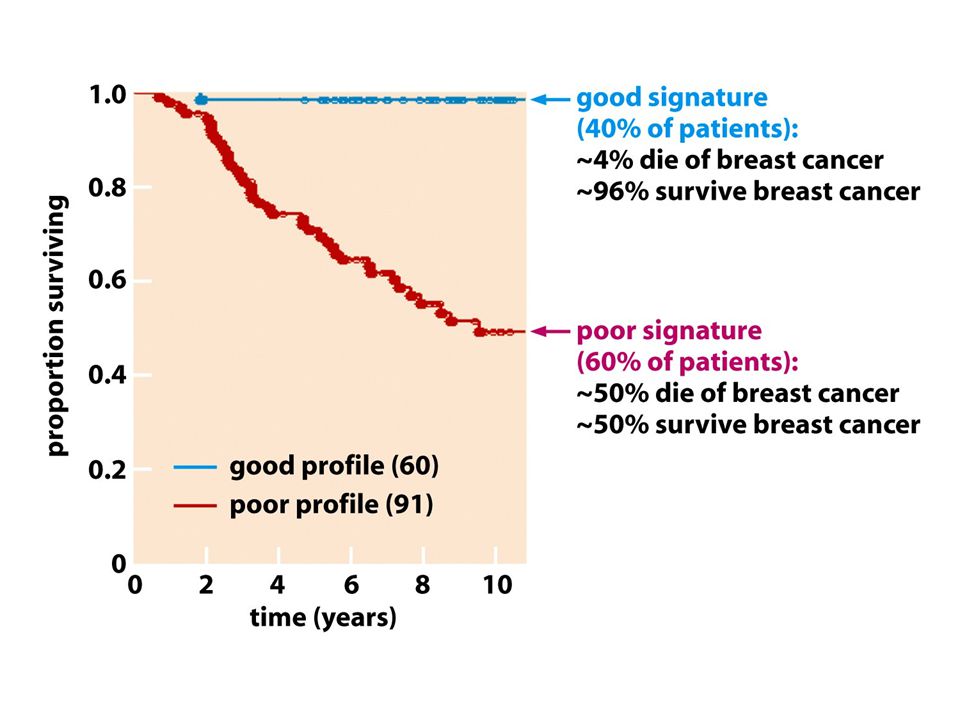
Can understanding the basic biology of cancer improve the treatment…..?

42
Copyright ©2001 by the National Academy of Sciences Sorlie, Therese et al. (2001) Proc. Natl. Acad. Sci. USA 98, 10869-10874
 Proc. Natl. Acad. Sci. USA 98,")
45
The future Understanding the genetic pathways of cancer development Treatment will be tailored to individual patients Aim of making it much more effective and less toxic

Similar presentations





 Carcinoembryonic.>")

 –Localised to breast +/- lymph nodes –Recommended standard treatment involves NEPTUNE Taxane.>")


 in combination with chemotherapy: pivotal metastatic breast cancer survival data 1.>")









