Download presentation
Presentation is loading. Please wait.

1
Dr. Paula Blanco & Dr. Peter Magner
Glomerular Diseases Dr. Paula Blanco & Dr. Peter Magner April 27th, 2015

2
Objectives 1491 List and describe the clinical syndromes with which patients with glomerular disease may present and name actual diseases for each syndrome. 1492 Explain the effect of glomerular changes on normal glomerular function, i.e. how the changes in the glomerulus affect the following: proteinuria, hypoalbuminemia, edema, hematuria, hypertension, hyperlipidemia and glomerular filtration rate. 1494 Describe an immunopathogenic mechanism involved in one of the various forms of glomerulonephritis and how it affects glomerular morphology. 1913 Propose a diagnostic approach for a patient with hematuria, and differentiate glomerular from non glomerular hematuria. 2879 Define nephrotic syndrome.

3
Manifestations of Glomerular Disease
Proteinuria Hematuria Hypertension Decreased GFR Rapid/acute Slow/chronic

4
Proteinuria 3+ protein on dipstick: What protein(s)? How much?
Where from? What diseases?

5
What proteins? Small plasma proteins (freely filtered)
enzymes light chains etc. Albumin (should not be filtered) Immunoglobulins (IgG) (should not be filtered)
 Immunoglobulins (IgG) (should not be filtered)")
6
Normal Renal Handling of Protein
Albumin: < 15 mg / 24 hr other small proteins: < 100 mg / 24 hr So 24 hour urine protein < 150 mg * more small proteins are filtered, but most is reabsorbed

7
Quantifying Proteinuria
Traditional to use 24 hour urine protein Inconvenient, expensive, innaccurate Should factor for body size (but many do not in adults) Random urine: Protein:creatinine ratio “PCR” or Albumin:creatinine ratio “ACR”
 Random urine: Protein:creatinine ratio PCR or. Albumin:creatinine ratio ACR")
8
Proteinuria Tubular proteinuria Glomerular proteinuria
up to 1 gm/ 24 hr mixed small proteins PCR 30 – 100 mg/mmol but ACR low Glomerular proteinuria Albumin is the majority normal glomeruli can leak albumin transiently with fever, exercise, severe CHF 8

9
Urine dipstick for protein 24-hour urine collection for albumin*
Stages of Diabetic renal involvement according to the urinary albumin Stage of nephropathy Urine dipstick for protein Urine ACR (mg/mmol) 24-hour urine collection for albumin* Normal Negative <~ 30 mg/day Mild (“Microalbuminuria”) ~ 30–300 mg/day Overt nephropathy (“macroalbuminuria” ) +, ++, +++ ++, +++, +++ +++, ++++ >~ 300 mg/day >~ 1000 mg/day >~ 3000 mg/day < 3 3 - 30 30 – 60 >60 > 200
 24-hour urine collection for albumin* Normal. Negative. <~ 30 mg/day. Mild. ( Microalbuminuria ) ~ 30–300 mg/day. Overt nephropathy. ( macroalbuminuria ) +, ++, , +++, , ++++ >~ 300 mg/day. >~ 1000 mg/day. >~ 3000 mg/day. < – 60. >60. > 200.")
10
Nephrotic Syndrome proteinuria (mostly albumin) hypoalbuminemia edema
ACR > 200 or PCR > 300 (traditional threshold is > 3 gm /24 hr) hypoalbuminemia edema hyperlipidemia (mostly LDL) lipiduria THIS MEANS GLOMERULAR DISEASE
 hypoalbuminemia. edema. hyperlipidemia (mostly LDL) lipiduria. THIS MEANS GLOMERULAR DISEASE.")
11
Manifestations of Glomerular Disease
Proteinuria (albuminuria) If severe may have other features of nephrotic syndrome Hematuria Hypertension Decreased GFR Rapid/acute Slow/chronic
 If severe may have other features of nephrotic syndrome. Hematuria. Hypertension. Decreased GFR. Rapid/acute. Slow/chronic.")
12
Glomeruli Anatomy Mechanisms of injury Pathological changes

18
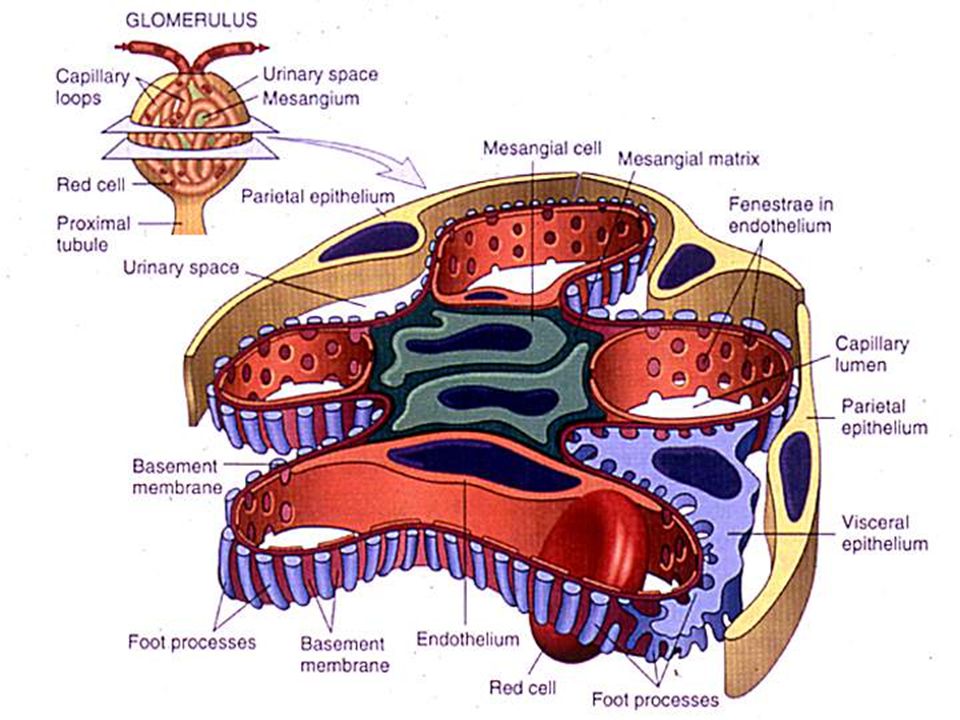
Normal Glomerulus

19
Capillary lumen

20
Immune Mechanisms in Glomerular diseases
Circulating immune complex deposition most common mechanism (~ 70% of all glomerulonephritis) many different diseases have a similar pathogenesis in terms of immune complexes activating complement antigens may be endogenous or exogenous
 many different diseases have a similar pathogenesis in terms of immune complexes activating complement. antigens may be endogenous or exogenous.")
21
GBM Circulating immune complex deposition

22
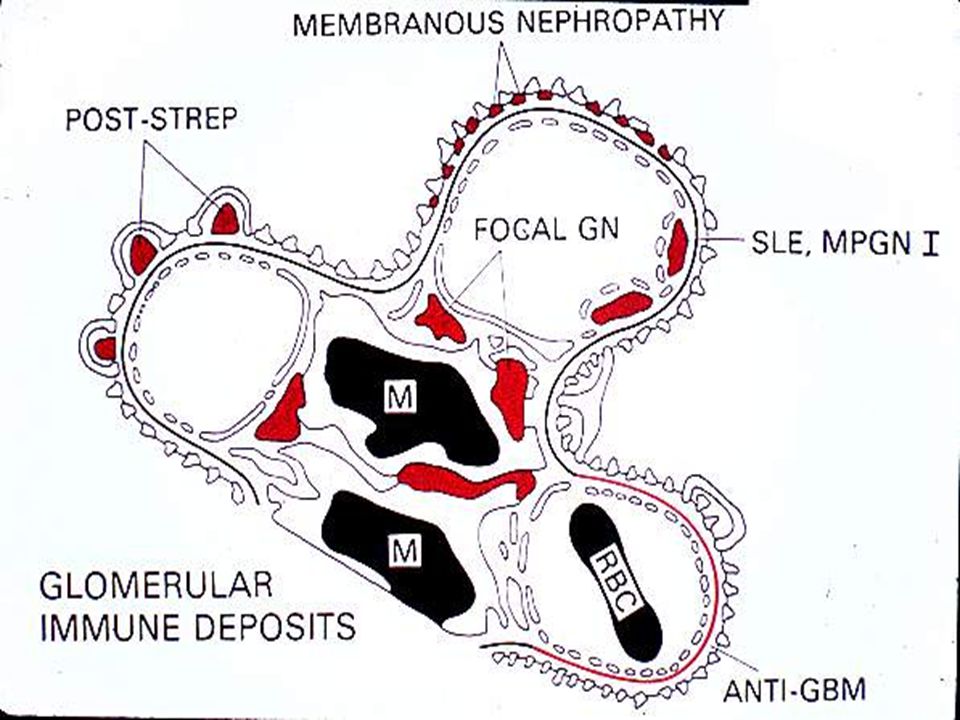
Immune Complex Deposition
Sites of deposition may be: subendothelial mesangial subepithelial Immune complexes may be detected by immunofluorescence or by electron microscopy

24
Subepithelial deposits

25
IgG

26
Expansion of mesangial areas

27
IgA 27

28
IgA 28

29
Anti-GBM Autoantibodies
antigen is part of collagen IV in the GBM antigen also in alveolar basement membranes, hence lung + kidney syndrome autoantibody (IgG class) fixes to GBM forming an in situ immune complex, activates complement antibody can be detected in kidney and in serum
 fixes to GBM forming an in situ immune complex, activates complement. antibody can be detected in kidney and in serum.")
30
IgG

31
Clinical- Pathological relationships
3 cases as examples

32
Case 1 22 year old woman complaining of swelling of the legs and a 9 kg weight gain no shortness of breath B.P. 120/70, weight 69 kg serum albumin 20 gm /L serum creatinine 80 umol/L

33
Case 1 Urinalysis findings: random urine ACR 450 mg/mmol (PCR 600)
4+ protein 0-2 RBC’s/HPF random urine ACR 450 mg/mmol (PCR 600)
")
34
Why do a renal biopsy? Prognosis:
many different diseases present in similar ways some are relatively “benign”, others progressive to chronic renal failure some diseases (e.g.. SLE) have different degrees of severity Treatment some are treatable and some are not some diseases require immediate treatment with potentially toxic drugs
 have different degrees of severity. Treatment. some are treatable and some are not. some diseases require immediate treatment with potentially toxic drugs.")
35
How is a renal biopsy done?
done with biopsy gun under U/S guidance tissue divided up for examining by: light microscopy immunofluorescence electron microscopy complications rare, most important is bleeding requiring transfusion, or embolization

36
Light microscopy

37
Immunofluorescence

38
Electron Microscopy

40
Normal glomerulus

41
Thickened basement membranes

42
“Spikes” along GBM

43
IgG - Granular GBM pattern

44
Subepithelial dense deposits
Lumen

45
Case 1 “Pure” Nephrotic Syndrome
Clinical Differential diagnosis (before we did the biopsy) includes: minimal change glomerulopathy focal glomerulosclerosis (FSGS) Membranous glomerulopathy IgA nephropathy (usually hematuria too) Diabetes (should be able to diagnose this without a biopsy!) Amyloidosis (rare)
 includes: minimal change glomerulopathy. focal glomerulosclerosis (FSGS) Membranous glomerulopathy. IgA nephropathy (usually hematuria too) Diabetes (should be able to diagnose this without a biopsy!) Amyloidosis (rare)")
46
Case 1 “Pure” Nephrotic Syndrome
Pathology Diagnosis: Membranous Glomerulopathy Usually ”primary” Sometimes “secondary” (we’ll come to this later)
")
47
Nephrotic Proteinuria - Points to remember
High ACR implies glomerular pathology glomerular changes in all causes of nephrotic syndrome include visceral epithelial cell “foot process fusion” features such as immune complex deposition point to specific disorders Permeability changes in GBM that permit heavy proteinuria may or may not be associated with breaks large enough for hematuria

48
What about lesser degrees of proteinuria. eg. PCR < 150 ( < 1
What about lesser degrees of proteinuria? eg. PCR < 150 ( < 1.5 gm/24 hr ) Tubular proteinuria? (< 50 % albumin) Normal glomeruli (transient albuminuria) Non-nephrotic glomerular diseases Suspect if other clues that point to glomerular disease Hematuria (especially with RBC casts) hypertension decreased GFR Systemic illness that may be associated with secondary glomerular involvement
 Tubular proteinuria (< 50 % albumin) Normal glomeruli (transient albuminuria) Non-nephrotic glomerular diseases. Suspect if other clues that point to glomerular disease. Hematuria (especially with RBC casts) hypertension. decreased GFR. Systemic illness that may be associated with secondary glomerular involvement.")
49
Case 2 27 year old east asian man complaining of recent onset of dark colored urine had flu-like illness with sore throat 3 days ago no frequency or dysuria (pain on urination) feels well
 feels well.")
50
Case 2 Physical Examination
BP 130/80 no skin rashes no edema rest of exam normal

51
Case 2 Laboratory findings
Urinalysis: 1+ proteinuria 20-30 RBC’s / HPF urine ACR 50 mg/mmol (~750 mg/24hr) serum creatinine = 116 umol/L Hb = 126 gm/L
 serum creatinine = 116 umol/L. Hb = 126 gm/L.")
52
Case 2 Special Laboratory Studies
ANA - negative Complement levels normal Streptococcal serology negative

53
Increased mesangial matrix - Mesangial proliferation

54
Increased mesangial matrix - Mesangial proliferation

55
IgA 55

56
Lumen Mesangial dense deposits RBC

57
Mesangial dense deposits

58
Case 2 Clinical presentation: “Nephritic” syndrome: some or all of
Hematuria, mild proteinuria, reduced GFR high BP Pathology Diagnosis: IgA Nephropathy Mesangial proliferation on LM IgA deposits on IF dense deposits EM

59
How can we classify glomerular diseases?
Clinical presentation (but lots of overlap) Nephrotic Nephritic rapidly progressive (~ bad nephritic) Etiology Primary vs. Secondary Pathology
 Nephrotic. Nephritic. rapidly progressive (~ bad nephritic) Etiology. Primary vs. Secondary. Pathology.")
60
Pathologic Classification of GN
Usually Nephrotic Minimal change Focal segmental glomerulosclerosis (FSGS) Membranous Usually Nephritic Mesangial proliferative (IgA) Diffuse proliferative +/- crescents Others diabetes, amyloid Etc…
 Membranous. Usually Nephritic. Mesangial proliferative (IgA) Diffuse proliferative +/- crescents. Others. diabetes, amyloid. Etc…")
61
Secondary Causes of GN Infections Drugs- NSAIDs
Viruses: HBV, HCV, HIV, malaria, bacterial endocarditis post-streptococcal Drugs- NSAIDs Neoplasia (a “paraneoplastic syndrome”) SLE & vasculitis Diabetes Amyloidosis (may be associated with myeloma)
 SLE & vasculitis. Diabetes. Amyloidosis (may be associated with myeloma)")
62
Case 3 72 year old woman admitted to hospital with recent history of increasing fatigue, weakness and swelling of legs no joint pains, skin rashes or shortness of breath serum creatinine one year ago was 160 umol/L

63
Case 3 Physical Examination
BP 160/88, pulse 78/min & regular, afebrile peripheral edema to knees rest of exam normal

64
Case Studies - 3 Laboratory Findings Hemoglobin 91 gm/L
Serum Creatinine 364 umol/L Urinalysis - 3+ protein 30-40 RBC’s/HPF and RBC casts Urine ACR 100

65
RBC cast

67
Normal glomerulus

68
Crescent formation 68

69
Crescent 69

70
Crescent 70

71
IgG

72
Crescentic Glomerulonephritis
Pathologic manifestation of many different diseases Three groups by immunofluorescence Linear antibody deposits along the GBM: Anti-GBM (+/- lungs involved) Immune complexes (esp. SLE, infections) No (or very few) immune deposits: “Pauci-immune” Vasculitis
 Immune complexes (esp. SLE, infections) No (or very few) immune deposits: Pauci-immune Vasculitis.")
73
Rapidly Progressive GN
the clinical correlate of crescentic GN proteinuria (usually PCR < 150 ) active urine sediment RBC’s, casts (granular casts, RBC casts) decreased GFR (days to weeks) usually feel “sick”
 active urine sediment. RBC’s, casts (granular casts, RBC casts) decreased GFR (days to weeks) usually feel sick")
74
Case 3 Clinical presentation: RPGN (rapidly Progressive GN)
- Nephritic syndrome with rapidly worsening GFR Pathology Diagnosis: Anti GBM syndrome with inflammation & crescents on LM Linear IgG along GBM on IF often not much on EM

75
Clinical- Pathological relationships
3 cases as examples of Nephrotic presentation Nephritic presentation RPGN

76
Summary

77
Manifestations of Glomerular Disease
Proteinuria Mostly albuminuria +/- edema, hypoalbuminemia, hyperlipidemia (“nephrotic syndrome”) Hematuria (usually microscopic +/- casts) Hypertension Decreased GFR acute: consider “RPGN” (with crescents on biopsy) chronic 77
 Hematuria (usually microscopic +/- casts) Hypertension. Decreased GFR. acute: consider RPGN (with crescents on biopsy) chronic. 77.")
78
Syndromes (presentations) of Glomerular Disease
Nephrotic Syndrome Lots of proteinuria (ACR>200) +/- edema, hypoalbuminemia, hyperlipidemia Nephritic Syndrome hematuria (usually microscopic +/- casts) Proteinuria: ACR usually ; High BP (usually) Declining GFR (usually) RPGN Severe Nephritic syndrome with rapid decline in GFR 78
 +/- edema, hypoalbuminemia, hyperlipidemia. Nephritic Syndrome. hematuria (usually microscopic +/- casts) Proteinuria: ACR usually ; High BP (usually) Declining GFR (usually) RPGN. Severe Nephritic syndrome with rapid decline in GFR. 78.")
79
Hematuria Urologic (plumbing) Nephrologic (interesting diseases)
Think anatomically from glomerulus down to urethra Then think about aetiology, investigations/referral Urologic (plumbing) Microscopic or Gross Clots very suggestive Often pain or other plumbing symptoms Occasionally “initial” or “terminal” Nephrologic (interesting diseases) Usually microscopic Casts are very specific (but not sensitive) Proteinuria is very suggestive Consider if systemic illness (eg. Lupus)
 Microscopic or Gross. Clots very suggestive. Often pain or other plumbing symptoms. Occasionally initial or terminal Nephrologic (interesting diseases) Usually microscopic. Casts are very specific (but not sensitive) Proteinuria is very suggestive. Consider if systemic illness (eg. Lupus)")
Similar presentations















 Membranous glomerulonephritis Focal segmental glomerulosclerosis.>")

 RENAL DISEASE: OVERVIEW AND ACUTE RENAL FAILURE Pathophysiology of Disease: Chapter 16 (388-394) Jack.>")






