Download presentation
Presentation is loading. Please wait.

1
PATHOLOGY OF VASCULAR OCCLUSION, ATHEROSCLEROSIS, HYPERTENSION AND LYMPHEDEMA

2
Define arteriosclerosis three patterns of arteriosclerosis. pathomechanism of atherosclerosis and the formation of the atheroma or plaque.

3
sequence of histologic changes in progression, growth mechanisms, decade of onset and clinical correlation of atherosclerosis

4
consequences of atherosclerosis when it affects the following vessels –cerebral vessels –coronary vessels –renal vessels –peripheral arteries

5
risk factors for atherosclerosis –modifiable –non-modifiable preventive measures for atherosclerosis.

6
clinical complications of atherosclerosis. how atherosclerosis can result in –thrombosis –embolism –aneurysms –ischemia –infarction

7
Atherosclerosis is a type of arteriosclerosis. Epidemiology most frequent cause of death in US and Europe incidence increases with age with major risk factors a. hypertension b. hyperlipidemia c. smoking

8
arteriosclerosis = "hardening of the arteries" describes three diseases: a. atherosclerosis b. medial calcific sclerosis (accumulation of calcium in tunica media of artery

9
c. arteriolar sclerosis- loss of elasticity in media of artery, thickening of walls and narrowing of lumen of small arteries often associated with hypertension

10
NORMAL ARTERIAL WALL

11
Atheromatous plaque - responsible for “carotid stenosis.”

12
A – Normal arterial wall Atheromatous plaque forms through the thickening of tunica media, which then reduces the arterial lumen (channel in which blood flows) and causes a stenosis (narrowing).
 and causes a stenosis (narrowing).")
13
in areas of damage in endothelium, LDL accumulates monocytes from blood enter subendothelial space, differentiate into macrophages and digest LDL, resulting in their conversion to FOAM CELLS, leading to formation of a FATTY STREAK.

14
Platelets also enter into lesion, secrete platelet derived growth factor which starts smooth muscle cells to multiply and move into damaged area. smooth muscle cells secrete a connective tissue matrix rich in collagen

15
death of foam cells leads to formation of a core of acellular lipid, = RAISED PLAQUE later, the plaque may fissure, causing a thrombus to form COMPLICATED LESION, this is an unstable plaque

16
Role of Macrophages and LDL 1 fatty streaks develop early in life 2. in order for macrophages to bind LDL, LDL must be oxidized, hence value of anti-oxidants such as Vit C, Vit E and B carotene in preventing ischemic heart disease

17
3. oxidized LDL's impair nitric oxide mediated vasodilatation and may cause release of tissue factors from macrophages that predispose to prevent breakdown of clots.

18
atherosclerosis is the presence of focal thickenings (plaques).
.")
19
atheromatous plaque becomes voluminous may rupture blood clot will form plaque becomes necrosed (liquefaction)
")
20
the necrosis or the hematoma may extend up to the tunica intima with rupture, tissue and the debris associated with necrosis will spill into the blood, migrate toward the brain (cerebral embolism) neurological incident...
 neurological incident...")
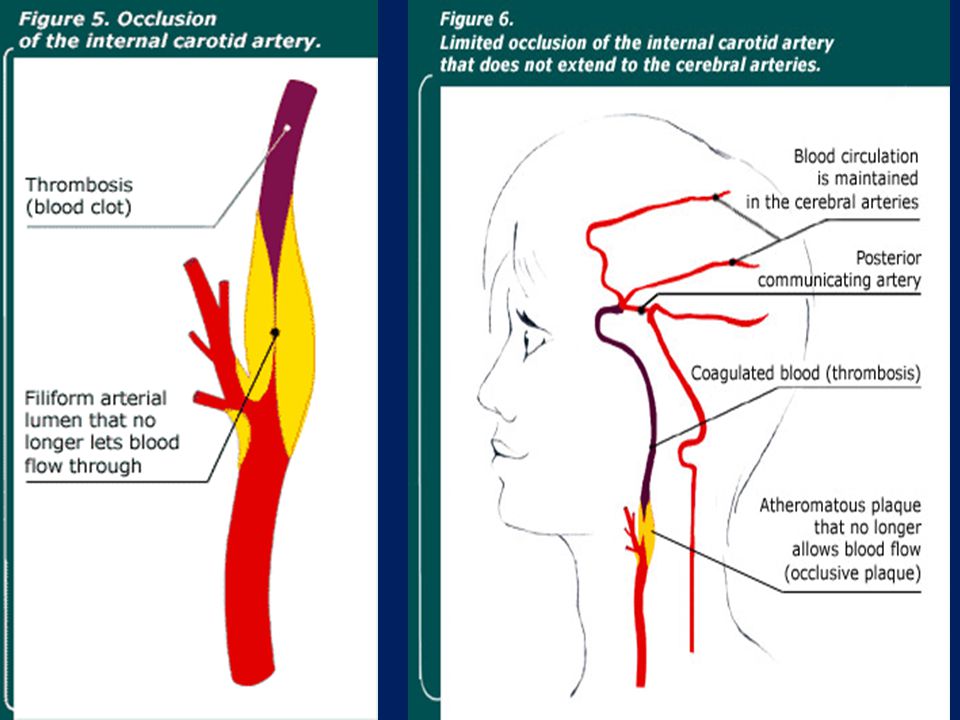
24
Occlusion of the carotid artery atheromatous plaque becomes voluminous blood can no longer flow and coagulates carotid artery is occluded (clogged). Blood no longer flows. The thrombosis (blood clot) extends within the entire internal carotid artery and up to the cerebral arteries.
 extends within the entire internal carotid artery and up to the cerebral arteries..")
25
Plaques may have complications including 1)calcification, common in advanced disease, with more complications 2) rupture or ulceration -result in cholesterol emboli, or provide a site for thrombosis
calcification, common in advanced disease, with more complications 2) rupture or ulceration -result in cholesterol emboli, or provide a site for thrombosis")
26
3)thrombosis superimposed on the plaque, most often presents on a disrupted plaque 4)hemorrhage into the plaque, from rupture of fibrous cap or capillaries into the plaque 5) medial atrophy in advanced AS can lead to the formation of aneurysms
thrombosis superimposed on the plaque, most often presents on a disrupted plaque 4)hemorrhage into the plaque, from rupture of fibrous cap or capillaries into the plaque 5) medial atrophy in advanced AS can lead to the formation of aneurysms")
30
Thrombosis of the carotid artery and the cerebral arteries stenosis (narrowing) develops into occlusion of the carotid artery (completely clogged). Insufficient blood flow stenosis (narrowing) of carotid artery- not enough blood Both develops into cerebral infarction
 of carotid artery- not enough blood Both develops into cerebral infarction.")
31
coronary artery disease (CAD) the accumulation of atheromatous plaques within the walls of the arteries that supply the myocardium
 the accumulation of atheromatous plaques within the walls of the arteries that supply the myocardium")
32
Angina – heart muscle is unable to be adequately oxygenated to meet its metabolic demand anaerobic metabolism - production of lactic acid as a waste product - stimulates nerve endings causing pain

33
The whole process of ischemia, necrosis (cell death) and inflammation of surrounding tissue is a myocardial infarction (MI). Dead heart cells cannot be replaced.

34
prior to menopause, few women suffer from coronary artery disease. protective actions of estrogen.

35
Estrogen reduces LDL accumulation, inhibits platelet aggregation, inhibits foam cell formation, decreases collagen and elastin production and, generally, acts as an anti- oxidant.

36
In what ways are estrogen beneficial? Fully developed atherosclerotic plaque consists of?

37
After menopause, the protective role of estrogen is diminished and women start suffering heart disease.

38
Risk Factors for Atherosclerosis Nonmodifiable Risk Factors Age Family history of premature atherosclerosis* Male sex

39
Modifiable Risk Factors Certain dyslipidemias (high LDL level, low HDL level) Cigarette smoking Diabetes mellitus Hypertension
 Cigarette smoking Diabetes mellitus Hypertension")
40
Alcohol intake Chlamydia pneumoniae infection High CRP level High level of small, dense LDL High lipoprotein level

41
Hyperhomocysteinemia Hyperinsulinemia Hypertriglyceridemia 5-Lipoxygenase polymorphisms Low intake of fruits and vegetables

42
Obesity or metabolic syndrome Prothrombotic states Psychosocial factors (eg, type A personality, depression, anxiety, work characteristics, socioeconomic status) Renal insufficiency Sedentary lifestyle
 Renal insufficiency Sedentary lifestyle")
43
Symptoms and Signs Atherosclerosis is initially asymptomatic Symptoms- when lesions impede blood flow.

44
when stable plaques grow and reduce the arterial lumen by > 70%. angina transient ischemic attacks intermittent claudication

45
Unstable plaques rupture Thrombosis Embolism Sudden death Aneurysms

46
Evaluation for atherosclerosis: History and physical examination Fasting lipid profile Plasma glucose and glycosylated hemoglobin (HbA 1c ) levels
 levels")
47
Treatment Lifestyle changes (diet, smoking, physical activity) Drug treatment of diagnosed risk factors Antiplatelet drugs Possibly statins, ACE inhibitors, β- blockers
 Drug treatment of diagnosed risk factors Antiplatelet drugs Possibly statins, ACE inhibitors, β- blockers")
48
Diet: Less saturated fat No trans fats More fruits and vegetables More fiber Moderate (if any) alcohol
 alcohol")
49
Physical activity: Regular physical activity (30 to 45 min 3 to 5 times/wk) Antiplatelet drugs: Aspirin Clopidogrel
 Antiplatelet drugs: Aspirin Clopidogrel")
50
Aneurysm an abnormal bulge in the wall of a blood vessel common in the aorta (aortic aneurysm)
")
51
Dangers of aneurysm: Atherosclerotic plaque formation at the site A clot (thrombus) may form, dislodge Increase in aneurysm size, pressure sx, pain Aneurysm rupture- life threatening
 may form, dislodge Increase in aneurysm size, pressure sx, pain Aneurysm rupture- life threatening")
52
Proceed to LYMPHEDEMA ppt

Similar presentations









, fibrous material and.>")






 accumulate in subendothelial space. Subsequent structural modifications of LDL.>")







 Atheroma as the presence of fatty material within the walls of arteries. The link between atheroma and the increased.>")