Download presentation
Presentation is loading. Please wait.

1
ATHEROSCLEROSIS By Joshua Bower Easter Revision 2014 J.Bower@warwick.ac.uk

2
Distinguish arteriosclerosis, atherosclerosis and arteriolosclerosis ARTERIOSCLEROSIS – generic term meaning ‘hardening of the arteries’ which encompasses the other 2 ATHEROSCLEROSIS – intimal lesions of arteries caused by atheromas ARTERIOLOSCLEROSIS – arteriolar hardening seen in HTN and DM

3
Intima: Endothelium BM Subendothelial connective tissue Internal elastic lamina Media: SMCs Connective Tissue Externa/Adventitia Connective tissue External elastic lamina Vasa vasorum

4
What are vasa vasorum? Network of small blood vessels supplying walls of large blood vessels Provide blood supply and nourishment to tunica adventitia and outer part of tunica media

5
What is an atheroma? Chronic intimal lesion occurring in arteries Causes lumen narrowing and weakening of vessel wall

6
Atheromas are characterised by accumulation of what FOUR things? [4] Vascular SMCs (vascular smooth muscle cells) ECM Inflammatory cells Lipids
 ECM Inflammatory cells Lipids.")
7
List FOUR modifiable and non-modifiable risk factors for atherosclerosis Hyperlipidaemia HTN Smoking DM Older Male FHx Genetics (e.g. ?) ModifiableNon-modifiable
 ModifiableNon-modifiable.")
8
Give an example of a genetic abnormality which may contribute to atheroma development Apolipoproteins APLs package fats e.g. LDL Some APLs act as ligand for receptors for uptake into cells Abnormal APL or receptors means: Reduced uptake Reduced excretion Thus increased serum LDL

9
What are the THREE key features of chronic inflammation? [3] Ongoing inflammation Ongoing tissue destruction Ongoing tissue repair

10
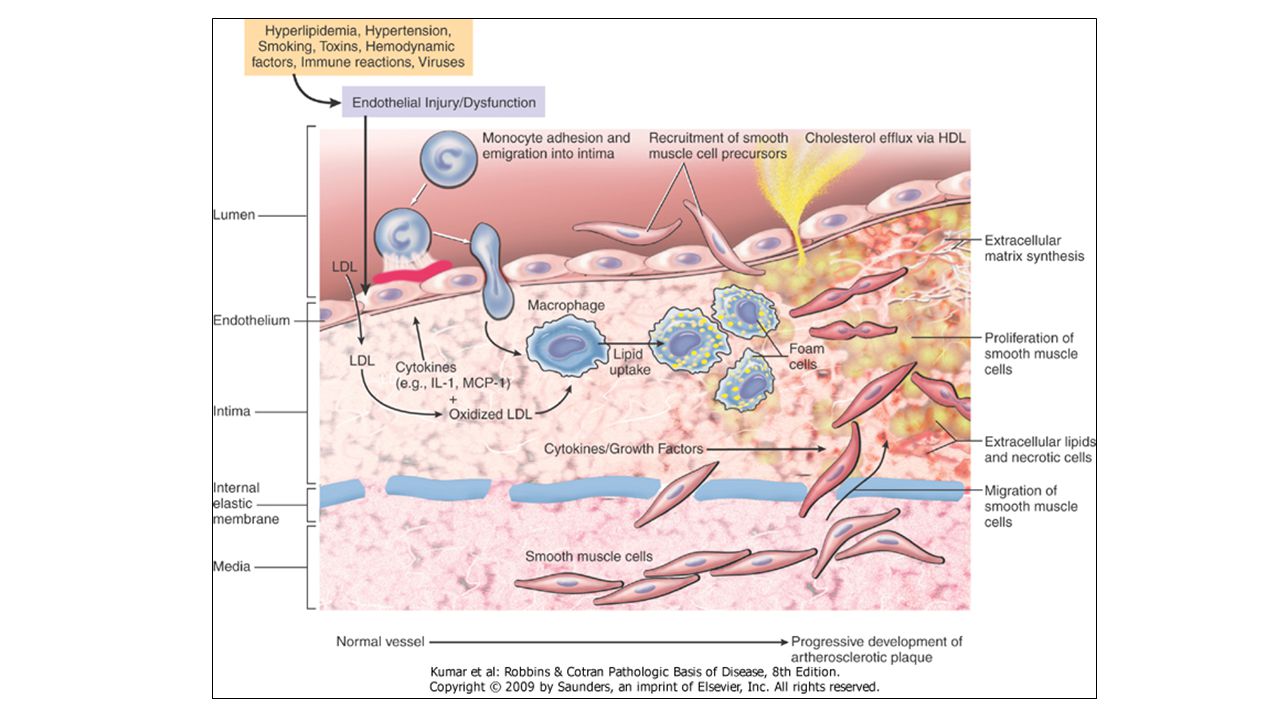
List the steps leading to atheroma development [6] 1.Chronic endothelial injury (e.g. HTN, smoking) 2.Endothelial dysfunction (becomes more permeable, cholesterol-rich LDLs enter and becomes oxidised 3.Monocytes enter, becomes macrophages and attempt to digest the cholesterol – become foam cells (visible as a fatty streak) 4.Foam cells release growth factors, stimulating SMC infiltration from the media, which then proliferate 5.Collagen and ECM becomes deposited, forming fibrofatty plaque 6.SMCs calcify as they degenerate in aged plaques, making them more vulnerable to rupture
![List the steps leading to atheroma development [6] 1.Chronic endothelial injury (e.g.](http://images.slideplayer.com/6/5661159/slides/slide_10.jpg "HTN, smoking) 2.Endothelial dysfunction (becomes more permeable, cholesterol-rich LDLs enter and becomes oxidised 3.Monocytes enter, becomes macrophages and attempt to digest the cholesterol – become foam cells (visible as a fatty streak) 4.Foam cells release growth factors, stimulating SMC infiltration from the media, which then proliferate 5.Collagen and ECM becomes deposited, forming fibrofatty plaque 6.SMCs calcify as they degenerate in aged plaques, making them more vulnerable to rupture.")
13
Suggest THREE outcomes of atheroma [3] Atheroma Chronic Narrowing of lumen Chronic reduction in blood flow Chronic ischaemia Weakening of vessel wall Aneurysm Plaque rupture Bleeding into atheroma Thrombus Occlusion Embolus
![Suggest THREE outcomes of atheroma [3] Atheroma Chronic Narrowing of lumen Chronic reduction in blood flow Chronic ischaemia Weakening of vessel wall Aneurysm Plaque rupture Bleeding into atheroma Thrombus Occlusion Embolus](http://images.slideplayer.com/6/5661159/slides/slide_13.jpg "Suggest THREE outcomes of atheroma [3] Atheroma Chronic Narrowing of lumen Chronic reduction in blood flow Chronic ischaemia Weakening of vessel wall Aneurysm Plaque rupture Bleeding into atheroma Thrombus Occlusion Embolus")
14
List THREE features of vessels which may make them more vulnerable to atheroma development [3] High pressure Bifurcation (e.g. abdominal aorta) Narrow lumen with high flow (e.g. cerebral vasculature)
![List THREE features of vessels which may make them more vulnerable to atheroma development [3] High pressure Bifurcation (e.g.](http://images.slideplayer.com/6/5661159/slides/slide_14.jpg "abdominal aorta) Narrow lumen with high flow (e.g. cerebral vasculature).")
15
An obese 67yo diabetic male presents to his GP with pain in his lower leg which becomes worse after he has been walking for a while. Diagnosis? Peripheral vascular disease Intermittent claudication Pain at rest Ischaemic limb These are atherosclerotic blockages outside of the coronary tree – usually lower limb

16
The effects of the atheroma on distal tissue is dependent on what THREE things? [3-5] Size of lumen Stability of plaque Degree of degeneration of underlying wall Natural Hx of plaque Type of blood supply

17
How can atheroma be treated? [3] Reduce risk Stenting by PCTA Bypass grafting via CABG
![How can atheroma be treated [3] Reduce risk Stenting by PCTA Bypass grafting via CABG](http://images.slideplayer.com/6/5661159/slides/slide_17.jpg "How can atheroma be treated [3] Reduce risk Stenting by PCTA Bypass grafting via CABG")
18
QUESTIONS? By Joshua Bower Easter Revision 2014 J.Bower@warwick.ac.uk

Similar presentations








, fibrous material and.>")











