Download presentation
Presentation is loading. Please wait.

1
Ethiopia Unlocking the confines of Illness pMTCT Project Fekadu Chala Dabi, Christine Groff Nadia Nijim, Rebecca Noe, Cynthia Pearson

2
Ethiopia

3
A Regional Glance: Population

4
A Regional Glance: GDP per Capita

5
Health System Structure Budget $150 million US ~ 1.7% of GDP 3 medical schools train 200 doctors a year, but highest rate of brain drain in Africa Physician to population ratio: 1 : 38,619 Health care facility to population is 1:172,000 –Health stations 1 : 27,456 persons –Hospitals 1 : 658,305 persons

6
Basic Health Determinants Indicator Status Life expectancy 43.8 years Child Mortality < 5 years 170 Infant Death <1years 1 in 10 Child Stunting and Malnutrition 64% Preventive Health Coverage <50% Access to Antenatal Services 34% Adult literacy29% females 41% males Access to Safe Water 35%

7
Ethiopia and HIV/AIDS 2,100,000 Ethiopian living with HIV/AIDS –52% women; 38% men; 10% children 6.4% HIV/AIDS prevalence –Urban 13.7% rural 3.7% 87 % of all HIV/AIDS infections result from hetero-sexual transmission. 990,000 estimated orphans Sources:UNAIDS,U.S.Census Bureau 7/2002

8
Ethiopia

9
The City: Nazret Capital city of the largest region - Oromia –Population: 130,000 Worst health conditions in Ethiopia 75% of the endemic disease are communicable –Respiratory, Diarrhoeal –Malaria/TB –STI/HIV/AIDS

10
Health Structure of Nazret Legend Church School Mosque Pharmacy FGAE Hospital/MOH Factory Clinic Highway Railroad Unpaved roads

11
Major pMTCT Interventions Improved Maternal Child Health (MCH) Services Voluntary Counseling & Testing (VCT) Safe infant-feeding choices Safe Motherhood practices Antiretroviral drugs (ARV): Nevirapine http://www.coregroup.org/working_groups/hiv_resour ce_materials.pdf
 Services Voluntary Counseling & Testing (VCT) Safe infant-feeding choices Safe Motherhood practices Antiretroviral drugs (ARV): Nevirapine ce_materials.pdf")
12
Project Objectives 1. Offer voluntary counseling and STI testing (VCT) to all (100%) women who are receiving antenatal care (ANC). 2. Increase the acceptance of VCT from 50% to 80% of ANC participant. 3. Increase acceptance/delivery of nevirapine from 20% to 80% of HIV infected mothers who received ANC and who have accepted VCT.
 to all (100%) women who are receiving antenatal care (ANC). 2. Increase the acceptance of VCT from 50% to 80% of ANC participant. 3. Increase acceptance/delivery of nevirapine from 20% to 80% of HIV infected mothers who received ANC and who have accepted VCT..")
13
Provision of VCT and pMTCT – MOH hospital, 3 private clinics, 1 RH clinic Training and program implementation –Family Guidance Association Community groups for follow-up support: –3 religious groups (2 Christian, 1 Muslim) –4 NGOs –1 PLWA group –1 women/mother’s support group, and –1 youth group Community Partners
 –4 NGOs –1 PLWA group –1 women/mother’s support group, and –1 youth group Community Partners")
14
Input: Time - 3-year program Training: VCT counselors – 2 weeks Clinics: ARV – 3 days 1-day refresher training every 6-months Training for replacement VCT counselors and clinic staff Bi-weekly visits by VCT and pMTCT trainers and supervisors (later monthly) Every 3 months overall project meeting
 Every 3 months overall project meeting")
15
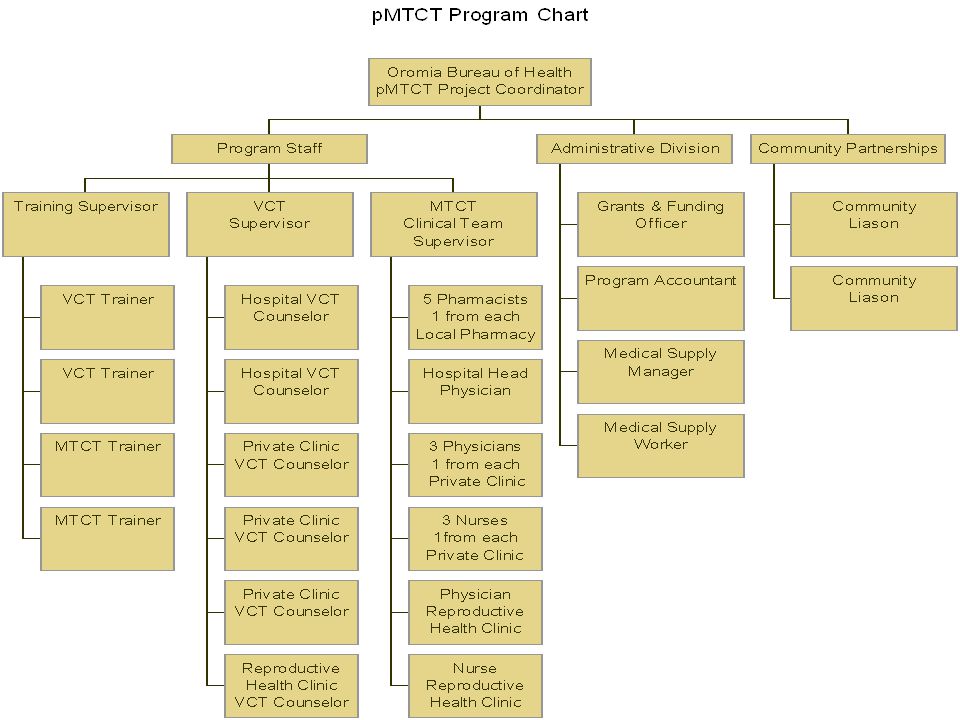
Input: Staff Trainer of trainers - 1 Trainers: 2 VCT; 2 clinic pMTCT Project coordinator: 1 Supervisors: 1 VCT; 1 pMTCT VCT staff: 6 (2-hospital, 1-RH clinic, 3-private clinic) pMTCT clinic staff (~14) doctors, nurses, midwifes
 pMTCT clinic staff (~14) doctors, nurses, midwifes")
17
Input: Other Resources Funding Training materials (rooms, lunch, supplies, kits) VCT and pMTCT guideline manuals for all participants Space to ensure VCT can be provided and will be confidential Supply of HIV rapid test kits, Nevirapine –6 months inventory maintained on hand at local hospital warehouse
 VCT and pMTCT guideline manuals for all participants Space to ensure VCT can be provided and will be confidential Supply of HIV rapid test kits, Nevirapine –6 months inventory maintained on hand at local hospital warehouse")
18
Present Model of VCT Service Delivery Pre-test counseling Testing (as desired by the client and after informed consent is provided Post-test counseling (more than one visit if needed) Individual risk assessment & risk reduction planning
 Individual risk assessment & risk reduction planning")
19
Model for Nevirapine Delivery Sustainable HIV kits/drug supply Strengthen delivery infrastructure Nevirapine HIV+ pregnant women –To women at the onset of labor: 200mg –To baby within 72 hrs. of delivery: 2mg/kg body weight

21
Process (1) Develop plan: initial training manuals Train VCT counselors and pMTCT clinic staff Monitor quality of training and quality of teaching Teach trainees to use the manual as a resource Initial follow-up: bi-weekly trainee meeting to discuss barriers/problems
 Develop plan: initial training manuals Train VCT counselors and pMTCT clinic staff Monitor quality of training and quality of teaching Teach trainees to use the manual as a resource Initial follow-up: bi-weekly trainee meeting to discuss barriers/problems")
22
Process (2) After 6 month in field – secondary training Ongoing support and feedback Monthly site visits by supervisors Monthly reports from project supervisors to coordinator Consumer satisfaction feedback
 After 6 month in field – secondary training Ongoing support and feedback Monthly site visits by supervisors Monthly reports from project supervisors to coordinator Consumer satisfaction feedback")
23
Outputs and Outcomes: Trained 6 VCT counselors; 14 clinic staff in pMTCT Track quality –Pre-post-test % Increase in knowledge Areas to improve curriculum –Focus groups at 6-month training Availability of HIV test/Nevirapine –% Of time in 3 years with no shortage of HIV test kits or Nevirapine

24
Outputs and Outcomes: (2) Use of pre-test counseling: –% of women who received counseling [initial use] Use of HIV testing/post-counseling: –% of women who received HIV testing during pregnancy [Measures initial use &continuity] Use of Nevirapine: –% of women who HIV+ and request treatment and receive course [measures continuity of service]
![Outputs and Outcomes: (2) Use of pre-test counseling: –% of women who received counseling [initial use] Use of HIV testing/post-counseling: –% of women who received HIV testing during pregnancy [Measures initial use &continuity] Use of Nevirapine: –% of women who HIV+ and request treatment and receive course [measures continuity of service]](http://images.slideplayer.com/17/5334498/slides/slide_24.jpg "Outputs and Outcomes: (2) Use of pre-test counseling: –% of women who received counseling [initial use] Use of HIV testing/post-counseling: –% of women who received HIV testing during pregnancy [Measures initial use &continuity] Use of Nevirapine: –% of women who HIV+ and request treatment and receive course [measures continuity of service]")
25
VCT/ARV Impact 100% ANC participants offered VCT 80% acceptance of VCT services 100% of HIV + women identified through VCT will have access to Nevirapine 80% of these (HIV + mothers & newborn) will complete Nevirapine regimen.
 will complete Nevirapine regimen.")
26
Amesegnalehu (Thank you for your attention)
")
Similar presentations



>")





: What Will it Take to Eliminate MTCT? Jessica Rodrigues Presentation for UNICEF Written.>")










