Download presentation
Presentation is loading. Please wait.

1
ARDS University of Washington Department of Respiratory Care Services Skills Day May, 2006

2
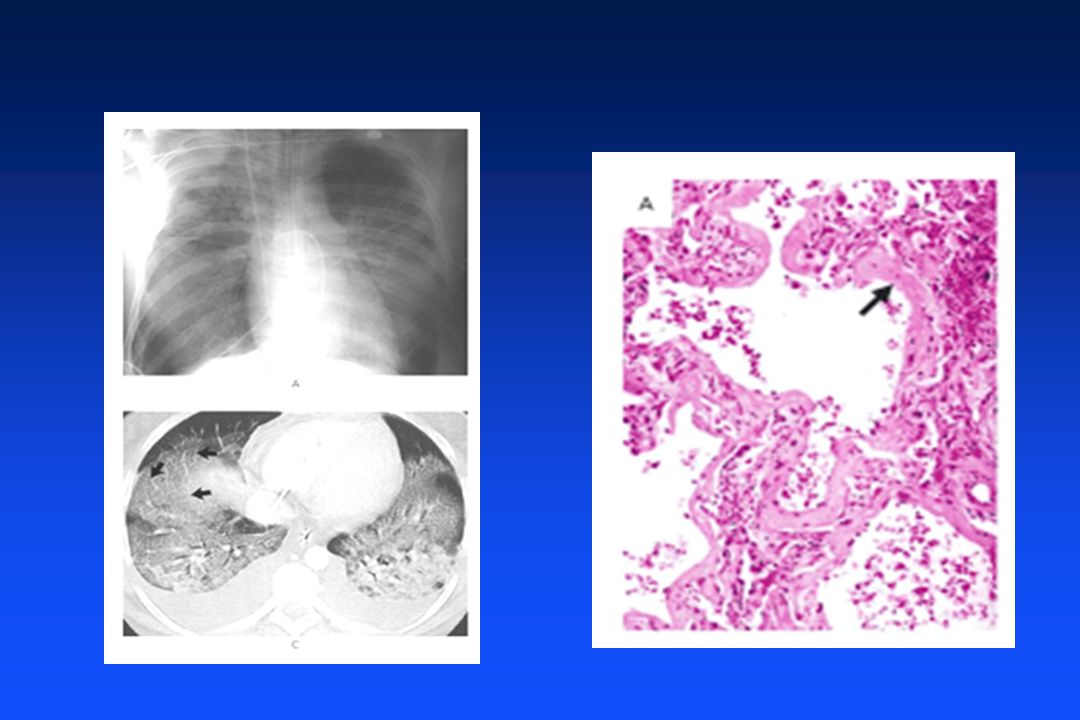
CASE PRESENTATION A 62 year old woman with a history of coronary artery disease comes to the ER with shortness of breath over the past 8 hours. A CXR reveals a bilateral alveolar filling process and her arterial blood gas shows marked hypoxemia despite a 70 % high flow mask. A PA catheter is placed to assess the cause of the bilateral infiltrates.

3
CASE PRESENTATION SVR - 500 dynes/sec/cm2 PA - 21/ 13 mm Hg PAOP - 11 mm Hg CO - 9 LPM You should: 1) Consider a inotrope such as dobutamine as she is in CHF. 2) Administer dopamine IV, evaluate carefully for a source of infection and cover with broad spectrum antibiotics 3) Consider volume infusion with normal saline to treat her volume depletion.
 Administer dopamine IV, evaluate carefully for a source of infection and cover with broad spectrum antibiotics 3) Consider volume infusion with normal saline to treat her volume depletion..")
4
CASET PRESENTATION She develops progressive hypoxemia despite 100 % non-rebreather mask and is intubated. The most appropriate ventilator management would include the following settings: A)V T = 600ml, PEEP = 15cmH 2 O B)V T = 600 ml, PEEP = 5 cmH 2 O C)V T = 400 ml, PEEP = 10 cmH 2 O D)V T = 400 ml, PEEP = 17.5 cmH 2 O
V T = 600ml, PEEP = 15cmH 2 O B)V T = 600 ml, PEEP = 5 cmH 2 O C)V T = 400 ml, PEEP = 10 cmH 2 O D)V T = 400 ml, PEEP = 17.5 cmH 2 O.")
5
ARDS Definition American-European Consensus Conference-1994 –Acute onset of respiratory symptoms (with associated predisposing factor) –Bilateral infiltrates on CXR –PCWP ≤18 or the absence of clinical evidence of LA hypertension –PaO2/FiO2 ratio: ·≤ 200 = ARDS ·≤ 300 = ALI (acute lung injury)
 –Bilateral infiltrates on CXR –PCWP ≤18 or the absence of clinical evidence of LA hypertension –PaO2/FiO2 ratio: ·≤ 200 = ARDS ·≤ 300 = ALI (acute lung injury)")
7
ARDS Predisposing Factors –Direct Lung Injury ·Pneumonia ·Aspiration ·Lung contusion ·Near-drowning ·Inhalation injury ·Fat emboli –Indirect lung injury ·Sepsis ·Severe trauma ·Acute pancreatitis ·Blood transfusions ·Cardiopulmonary bypass

8
PATHOGENESIS Target organ injury from host’s inflammatory response and uncontrolled liberation of inflammatory mediators Localized manifestation of SIRS Neutrophils and macrophages play major roles Complement activation Cytokines: TNF- , IL-1 , IL-6 Platelet activation factor Eicosanoids: prostacyclin, leukotrienes, thromboxane Free radicals Nitric oxide

9
PATHOPHYSIOLOGY Abnormalities of gas exchange Oxygen delivery and consumption Cardiopulmonary interactions Multiple organ involvement

10
ABNORMALITIES OF GAS EXCHANGE Hypoxemia: HALLMARK of ARDS –Increased capillary permeability –Interstitial and alveolar exudate –Surfactant damage –Decreased FRC –Diffusion defect and right to left shunt

11
ARDS STAGES Acute or Exudative Phase Proliferative or Subacute Phase Chronic Phase –Scarring –Recovery

12
ARDS STAGES Acute, exudative phase –rapid onset of respiratory failure after trigger –diffuse alveolar damage with inflammatory cell infiltration –hyaline membrane formation –capillary injury –protein-rich edema fluid in alveoli –disruption of alveolar epithelium

13
NORMAL ALVEOLUS Type I cell Endothelial Cell RBC’s Capillary Alveolar macrophage Type II cell

14
ACUTE PHASE OF ARDS Type I cell Endothelial Cell RBC’s Capillary Alveolar macrophage Type II cell Neutrophils

15
Proliferative Phase Subacute, Proliferative phase: –persistent hypoxemia –development of hypercarbia –fibrosing alveolitis –further decrease in pulmonary compliance –pulmonary hypertension

16
Chronic Phase Chronic phase –obliteration of alveolar and bronchiolar spaces and pulmonary capillaries Recovery phase –gradual resolution of hypoxemia –improved lung compliance –resolution of radiographic abnormalities

17
ARDS Treatments Decades of Ineffective Treatments –Steroids –NSAIDs –Pentoxyphlline –Nitric oxide –surfactant –……….

18
Low Tidal Volume Strategies in ARDS High lung inflation volumes over distend more compliant portions of the lung. In the past our high tidal volume strategies may have actually caused lung injury (“ventilator lung”). Using lower lung volumes may prevent over distension and reduce ventilator induced lung injury.
. Using lower lung volumes may prevent over distension and reduce ventilator induced lung injury..")
19
ARDS NETWORK Clinical Trials Network > 20 centers nationwide Multiple Trials Initial Study “ARMA” Randomized to 6 ml/kg (IBW) vs. 12 ml/kg and plateau pressure <30 cm Study was halted early due to significant survival improvement in one group

20
New England Journal of Medicine 2000;342:1301-8

21
Mortality Prior to Hospital Discharge 6 ml/kg12 ml/kg P=0.0054

22
What about PEEP ?

23
549 ARDS Patients Randomized to high or low PEEP levels –5 versus 12 cm PEEP –? Differences in mortality, ventilator, ICU and hospital days

24
High vs. Low PEEP Protocol

25
High vs. Low PEEP

26
Where do I set PEEP ?

27
Recruitment Maneuvers Hyperinflation maneuvers to open collapse lung Some parts of lung are open, some are collapsed Detrimental effects: –“Baby lungs” can be overdistended –Collapsed portions can put traction on normal portions causing injury –Opening and closing of collapsed or atelectatic areas could cause “shear stress injury”

28
Baby Lung Effect Shear Force Effect

29
NEJM 1998;347

30
CT Scan and outcome study of patients with ARDS who had recruitable lung looked at Percentage of recruitable lung looked at as a predictor of outcomes

31
13% of lung was recruitable Higher percentage of recruitable lung correlted with: –Higher oxygenation requirments –Heavier lungs –Worse outcome BOTTOM LINE: THE JURY IS STILL OUT ON RECRUITMENT MANEUVERS

32
KCLIP DATA Survey of ALI and ARDS in King County NEJM 2005;353:1685

33
KCLIP Cohort NEJM 2005;353:1685

35
ARDS Big Problem Small tidal volumes Small pressures PEEP around 10 No recruitment maneuvers at this time.

Similar presentations









>")







 Dr. Meg-angela Christi Amores.>")


 Acute Respiratory Distress Syndrome (ARDS) Pathophysiology in ARDS Therapy.>")