Download presentation
Presentation is loading. Please wait.

1
David W. Chang, EdD, RRT University of South Alabama

2
1. Definition 2. History 3. Pathophysiology 4. Mechanical Stress 5. Clinical presentations 6. Management Strategies 7. Complications

3
1. Definition 2. History 3. Pathophysiology 4. Mechanical Stress 5. Clinical presentations 6. Management Strategies 7. Complications

4
Definition of ALI and ARDS (1994 AECC) Acute onset Hypoxemia (PaO 2 /F I O 2 = 200 or 300 mm Hg) Bilateral infiltrates PCWP <18 mm Hg
 Acute onset Hypoxemia (PaO 2 /F I O 2 = 200 or 300 mm Hg) Bilateral infiltrates PCWP <18 mm Hg")
5
1. Definitions of ALI and ARDS

6
Definition of ARDS (2011 Berlin) P/F index mild ARDS: 201 - 300 mmHg (≤ 39.9 kPa) moderate ARDS: 101 - 200 mmHg (≤ 26.6 kPa) severe ARDS: ≤ 100 mmHg (≤ 13.3 kPa) Radiographic severity Respiratory compliance ≤ 40 mL/cm H 2 O PEEP ≥ 10 cm H 2 O Corrected minute ventilation ≥ 10 L/min
 P/F index mild ARDS: mmHg (≤ 39.9 kPa) moderate ARDS: mmHg (≤ 26.6 kPa) severe ARDS: ≤ 100 mmHg (≤ 13.3 kPa) Radiographic severity Respiratory compliance ≤ 40 mL/cm H 2 O PEEP ≥ 10 cm H 2 O Corrected minute ventilation ≥ 10 L/min")
7
1. Definition 2. History 3. Pathophysiology 4. Mechanical Stress 5. Clinical presentations 6. Management Strategies 7. Complications

8
History 1950’s – Pulmonary edema (respirator lung, DaNang lung, shock lung, post-traumatic lung, wet lung) 1959 – Neonatal RDS (Avery and Mead) 1967 – ARDS (Ashbaugh et al)
 1959 – Neonatal RDS (Avery and Mead) 1967 – ARDS (Ashbaugh et al)")
9
History Late 1960s – intensive care units became common in the U.S. 1930s to 1950s – Drinker respirator (negative pressure ventilation, iron lung, chest cuirass) 1950s to present – manual ventilation, positive pressure breathing, mechanical ventilator, microprocessor controlled ventilator Mortality ranges from 90% (untreated) to 25% (treated aggressively)
 1950s to present – manual ventilation, positive pressure breathing, mechanical ventilator, microprocessor controlled ventilator Mortality ranges from 90% (untreated) to 25% (treated aggressively).")
14
1. Definition 2. History 3. Pathophysiology 4. Mechanical Stress 5. Clinical presentations 6. Management Strategies 7. Complications

15
Pathophysiology Direct injury (e.g., pneumonia, aspiration, inhalation of toxins, near drowning, pulmonary contusion, fat embolism) Indirect injury (e.g., sepsis, severe trauma, acute pancreatitis, cardiopulmonary bypass, transfusion of blood products, drug overdose)
 Indirect injury (e.g., sepsis, severe trauma, acute pancreatitis, cardiopulmonary bypass, transfusion of blood products, drug overdose)")
16
Pathophysiology Direct injury may lead to (A) activation of alveolar macrophages (B) development of inflammatory response within the lungs (C) alveolar epithelial damage (D) alveolar walls are thickened due to acute distention of capillaries and interstitial edema
 activation of alveolar macrophages (B) development of inflammatory response within the lungs (C) alveolar epithelial damage (D) alveolar walls are thickened due to acute distention of capillaries and interstitial edema")
17
Pathophysiology Direct injury may lead to (E) pathological abnormality in the intra-alveolar space (F) alveolar filling by edema, fibrin, collagen, neutrophilic aggregates or blood (G) V/Q mismatch and intrapulmonary shunting
 pathological abnormality in the intra-alveolar space (F) alveolar filling by edema, fibrin, collagen, neutrophilic aggregates or blood (G) V/Q mismatch and intrapulmonary shunting")
18
Pathophysiology Indirect injury may lead to (A) Inflammatory mediators released from the extrapulmonary foci into the systemic circulation (B) target of damage is the pulmonary vascular endothelial cell (C) Endothelial dysfunction causes fluid extravasation from the capillaries and impaired drainage of fluid from the lungs
 Inflammatory mediators released from the extrapulmonary foci into the systemic circulation (B) target of damage is the pulmonary vascular endothelial cell (C) Endothelial dysfunction causes fluid extravasation from the capillaries and impaired drainage of fluid from the lungs")
19
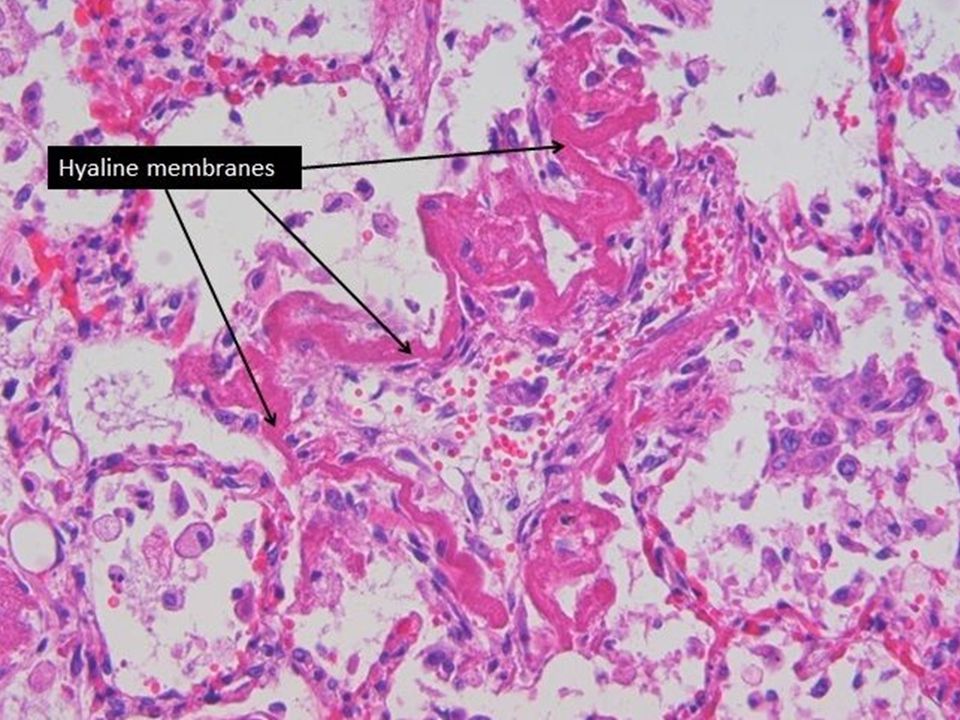
Pathophysiology Indirect injury may lead to (D) Dysfunction of type II pulmonary epithelial cells leads to reduction of surfactant (E) Increase of vascular permeability (transudate – a pale esinophilic finely granular, replaces the air) *Exudate is caused by inflammation Transudate is caused by disturbance of hydrostatic pressure and colloid osmotic pressure
 Dysfunction of type II pulmonary epithelial cells leads to reduction of surfactant (E) Increase of vascular permeability (transudate – a pale esinophilic finely granular, replaces the air) *Exudate is caused by inflammation Transudate is caused by disturbance of hydrostatic pressure and colloid osmotic pressure")
20
Pathophysiology Indirect injury may lead to (F) Recruitment of monocytes, polymorphonuclear leukocytes, platelets, and other abnormal cells (G) Primary pathological alteration is microvascular congestion and interstitial edema (H) V/Q mismatch and intrapulmonary shunting
 Recruitment of monocytes, polymorphonuclear leukocytes, platelets, and other abnormal cells (G) Primary pathological alteration is microvascular congestion and interstitial edema (H) V/Q mismatch and intrapulmonary shunting")
23
1. Definition 2. History 3. Pathophysiology 4. Mechanical Stress 5. Clinical presentations 6. Management Strategies 7. Complications

24
Mechanical Stress In ARDS, lung structure and function are not homogenous (i.e., healthy and sick lung units are mingled) Collapsed lung units require higher positive pressure Normal lung units become overdistended at high pressures (video) Barotrauma or volutrauma is more likely to occur in normal lung units
 Collapsed lung units require higher positive pressure Normal lung units become overdistended at high pressures (video) Barotrauma or volutrauma is more likely to occur in normal lung units")
26
1. Definition 2. History 3. Pathophysiology 4. Mechanical Stress 5. Clinical presentations 6. Management Strategies 7. Complications

27
Clinical presentations (ventilation & oxygenation) Tachypnea Rapid shallow breathing (↑f/V T ) ↑V D /V T ↓V A (V A = V T – V D ) ↑V/Q mismatch ↑Intrapulmonary Shunting ↓PaO 2 /F I O 2 (P/F) index ↑PaCO 2 due to fatigue of respiratory muscles Impending ventilatory failure Acute ventilatory failure
 Tachypnea Rapid shallow breathing (↑f/V T ) ↑V D /V T ↓V A (V A = V T – V D ) ↑V/Q mismatch ↑Intrapulmonary Shunting ↓PaO 2 /F I O 2 (P/F) index ↑PaCO 2 due to fatigue of respiratory muscles Impending ventilatory failure Acute ventilatory failure")
28
Clinical presentations (radiographic) Bilateral infiltrates No signs of large pleural effusion (normal costophrenic angles) No signs of atrial enlargement No signs of heart failure (e.g., PCWP >18 mm Hg) or volume overload (high systemic blood pressure, peripheral edema)
 Bilateral infiltrates No signs of large pleural effusion (normal costophrenic angles) No signs of atrial enlargement No signs of heart failure (e.g., PCWP >18 mm Hg) or volume overload (high systemic blood pressure, peripheral edema)")
29
1. Definition 2. History 3. Pathophysiology 4. Mechanical Stress 5. Clinical presentations 6. Management Strategies 7. Complications

30
Management Strategies (ineffective, controversial, transient positive effects or not validated in large studies) Drugs Inhaled synthetic surfactant, IV antibody to endotoxin, ketoconazole (anti-fungal), ibuprofen (NSAID), simvastatin (cholesterol reduction), and inhaled nitric oxide (pulmonary vasodilator) Nutritional support and supplement Devices ECMO, HFOV
 Drugs Inhaled synthetic surfactant, IV antibody to endotoxin, ketoconazole (anti-fungal), ibuprofen (NSAID), simvastatin (cholesterol reduction), and inhaled nitric oxide (pulmonary vasodilator) Nutritional support and supplement Devices ECMO, HFOV")
31
Management Strategies (reasonable and potentially useful) Fluid management Infection control (early intervention) Prevention of VAP Noninvasive ventilation (early intervention) Nutritional support (enteral feeding tube) Frequent position changes and range of motion
 Fluid management Infection control (early intervention) Prevention of VAP Noninvasive ventilation (early intervention) Nutritional support (enteral feeding tube) Frequent position changes and range of motion")
32
Management Strategies (current practice) Mechanical ventilation with PEEP Decramental recruitment maneuver for optimal PEEP Low VT and permissive hypercapnia Airway pressure release ventilaiton Inverse ratio ventilation Prone positioning
 Mechanical ventilation with PEEP Decramental recruitment maneuver for optimal PEEP Low VT and permissive hypercapnia Airway pressure release ventilaiton Inverse ratio ventilation Prone positioning")
33
Management Strategies Mechanical ventilation (volume-controlled or pressure-controlled) to reduce work of breathing Keep airway pressures below thresholds PIP < 50 cm H 2 O Plateau pressure < 35 cm H 2 O (ARDSNet recommends < 30 cm H2O) Mean airway pressure < 30 cm H 2 O PEEP < 10 cm H 2 O
 to reduce work of breathing Keep airway pressures below thresholds PIP < 50 cm H 2 O Plateau pressure < 35 cm H 2 O (ARDSNet recommends < 30 cm H2O) Mean airway pressure < 30 cm H 2 O PEEP < 10 cm H 2 O")
34
Management Strategies Oxygen and PEEP to provide oxygenation Note effects of PEEP and other factors on airway pressures (Figure) mPaw = (f x I time / 60) x (PIP – PEEP) + PEEP mPaw may be used to monitor hemodynamic effects plateau pressure may be used to monitor overdistention Recommended F I O 2 /PEEP combinations (Table) Recruitment maneuver to determine optimal PEEP (Video)
 mPaw = (f x I time / 60) x (PIP – PEEP) + PEEP mPaw may be used to monitor hemodynamic effects plateau pressure may be used to monitor overdistention Recommended F I O 2 /PEEP combinations (Table) Recruitment maneuver to determine optimal PEEP (Video)")
40
Management Strategies Low V T and Permissive Hypercapnia to minimize lung injury (Table) 6 mL/Kg as low as 4 mL/Kg to keep P PLAT < 30 cm H 2 O permit PaCO 2 to rise acidosis is managed by bicarbonate or tromethamine
 6 mL/Kg as low as 4 mL/Kg to keep P PLAT < 30 cm H 2 O permit PaCO 2 to rise acidosis is managed by bicarbonate or tromethamine")
42
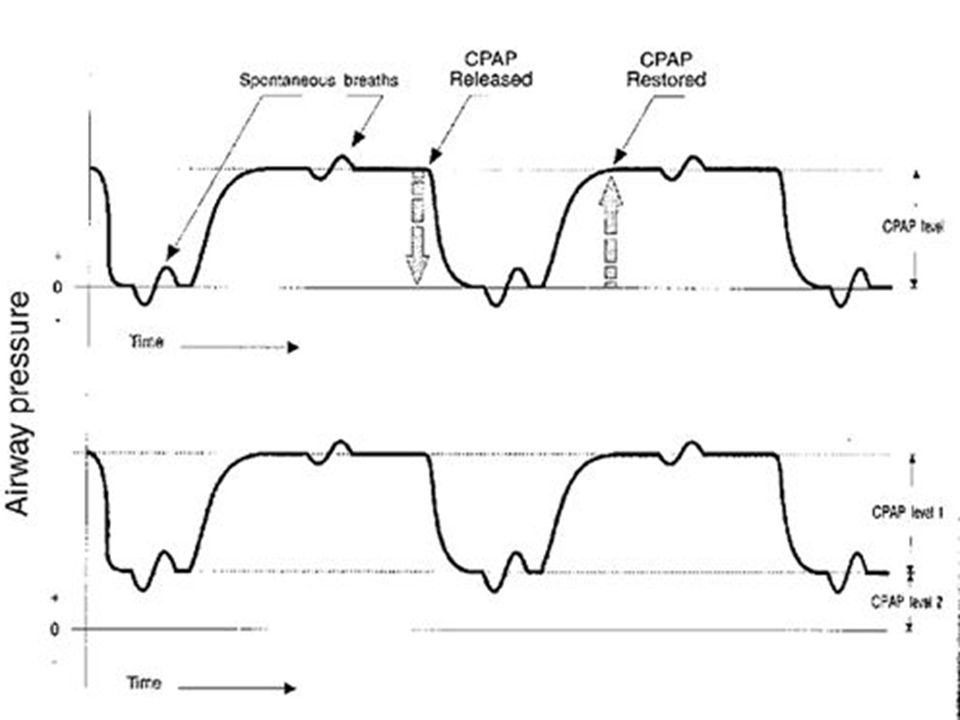
Management Strategies Airway Pressure Release Ventilation (APRV) (Figure) ↓decreased airway pressure requirement ↓ minute ventilation ↓ dead-space ventilation promote spontaneous breathing ↓ use of sedation & neuromuscular blockade optimized ABG results ↑ FRC ↑ cardiac output
 (Figure) ↓decreased airway pressure requirement ↓ minute ventilation ↓ dead-space ventilation promote spontaneous breathing ↓ use of sedation & neuromuscular blockade optimized ABG results ↑ FRC ↑ cardiac output")
44
Management Strategies Inverse ratio ventilation (IRV) Pressure-Controlled + IRV (pressure titrated to low V T 4 to 7 mL/kg) Long inspiratory time (inspiratory flow titrated to desired inverse ratio)
 Pressure-Controlled + IRV (pressure titrated to low V T 4 to 7 mL/kg) Long inspiratory time (inspiratory flow titrated to desired inverse ratio)")
45
Management Strategies Inverse ratio ventilation (IRV) Facilitate gas exchange (esp. O 2 ) Reduce F I O 2 and PEEP requirement Require sedation and neuromuscular blockade Monitor for improvement & hemodynamic effects
 Reduce F I O 2 and PEEP requirement Require sedation and neuromuscular blockade Monitor for improvement & hemodynamic effects.")
47
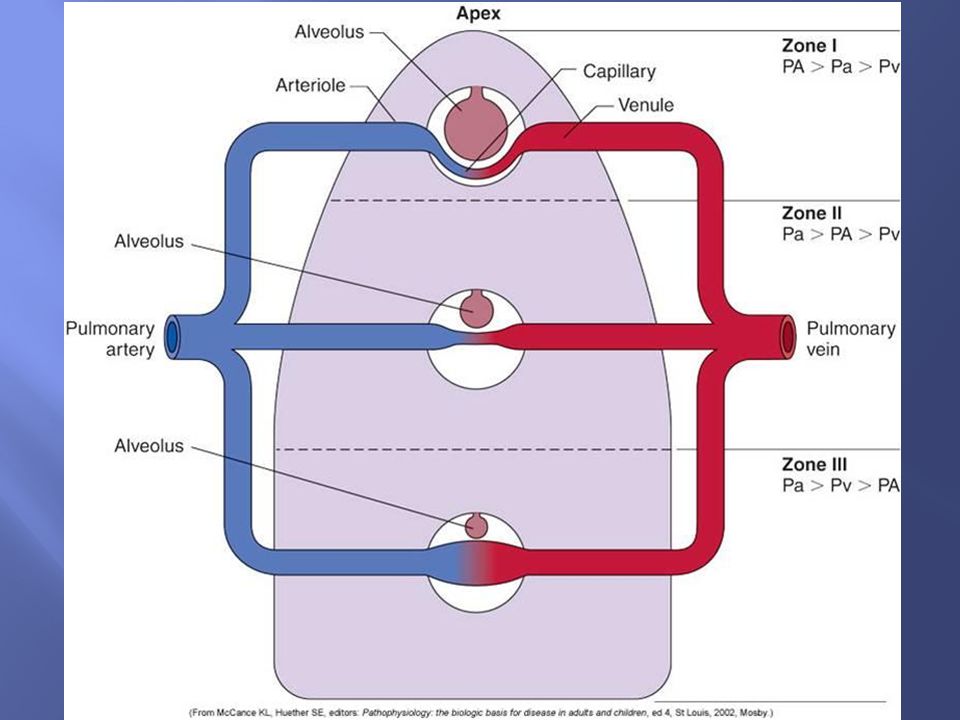
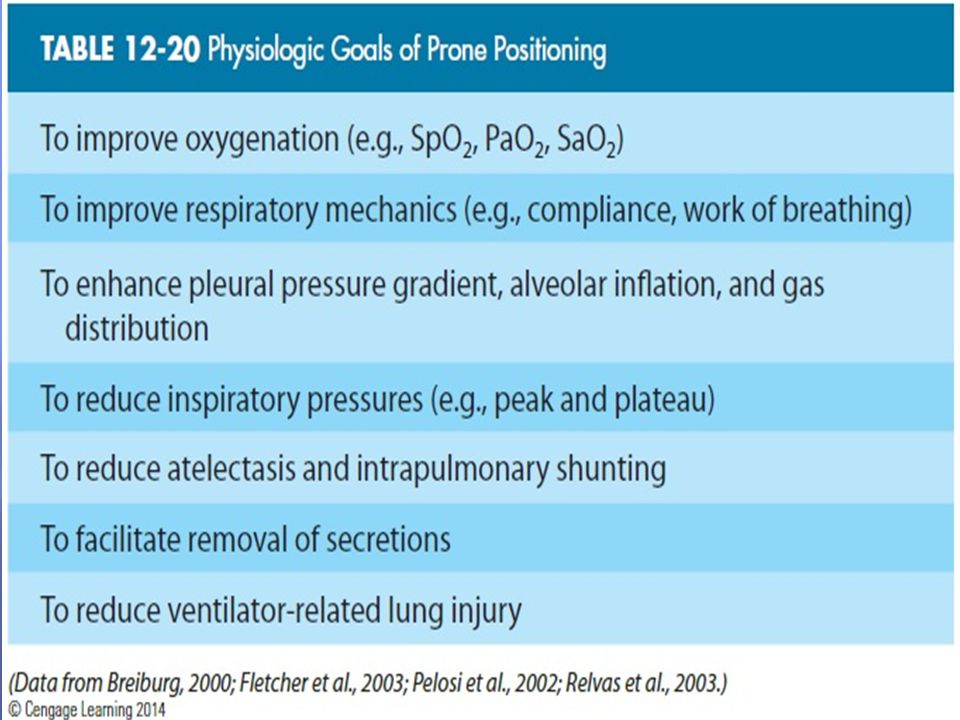
Management Strategies Prone positioning Lung zones Lung volume distribution * Improvement in oxygenation is temporary

54
1. Definition 2. History 3. Pathophysiology 4. Mechanical Stress 5. Clinical presentations 6. Management Strategies 7. Complications

55
Complications Ventilator-associated pneumonia Prevention and intervention Hypoxic-ischemic encephalopathy Brain (2% body weight, 15% energy consumption, cannot hold or store energy in the form of glycogen, cannot utilize fatty acids, depends on a constant supply of oxygen and glucose) CPP = MAP – ICP (normal 70 to 80 mm Hg)
 CPP = MAP – ICP (normal 70 to 80 mm Hg)")
59
Early intervention Team approach Tailor management strategies to patient’s need Prevent complications

Similar presentations