Download presentation
Presentation is loading. Please wait.

1
Pathobiology of Breast Cancer Associate Professor Department of Pathology and Laboratory Medicine Ruth A. Lininger, MD MPH

2
1. Anatomy and Histology of the Normal Breast

3
Terminal duct/lobular units Nipple

4
Histology of the Normal Breast

5
Terminal duct Lobular unit Intralobular stroma Interlobular stroma Ductal Carcinomas Arise Here Lobular Carcinomas Arise Here Terminal Duct Lobular Unit

6
Epithelium Myoepithelium

7
Immunostain for Smooth Muscle Actin

8
Epithelium Myoepithelium

9
2. Normal Physiologic States of the Breast Pregnancy and Lactation Post-Menopausal State

10
Pregnancy and Lactation Changes Breast changes in response to hormonal stimulation secondary to B-HCG and progesterone (pregnancy) and prolactin (lactation) Rapid growth of the terminal ducts and lobules Secretory epithelial changes –Vacuolated cytoplasm, enlarged “activated” nuclei with prominent nuceoli (biosynthetic center for the cell) –Occurs in a patchy fashion throughout the breast with progressive recruitment of lobules with successive pregnancies Depletion of fibrofatty stroma Increased stromal vascularity Increased areolar pigmentation Involution post cessation of lactation
 and prolactin (lactation) Rapid growth of the terminal ducts and lobules Secretory epithelial changes –Vacuolated cytoplasm, enlarged activated nuclei with prominent nuceoli (biosynthetic center for the cell) –Occurs in a patchy fashion throughout the breast with progressive recruitment of lobules with successive pregnancies Depletion of fibrofatty stroma Increased stromal vascularity Increased areolar pigmentation Involution post cessation of lactation")
11
Foamy cytoplasm Secretory material

12
Prominent nucleoli Lactational Change

13
Post-menopausal Changes Breast undergoes atrophic changes in response to LOSS of hormonal support (decrease in estrogen and progesterone) Loss of glandular epithelium Fatty replacement of breast tissue Atrophy occurs in a patchy fashion with interspersed unaffected lobules
 Loss of glandular epithelium Fatty replacement of breast tissue Atrophy occurs in a patchy fashion with interspersed unaffected lobules")
14
Intralobular stromal collagenization Post-Menopausal Breast

16
3. Genetics and Epidemiology of Breast Cancer

17
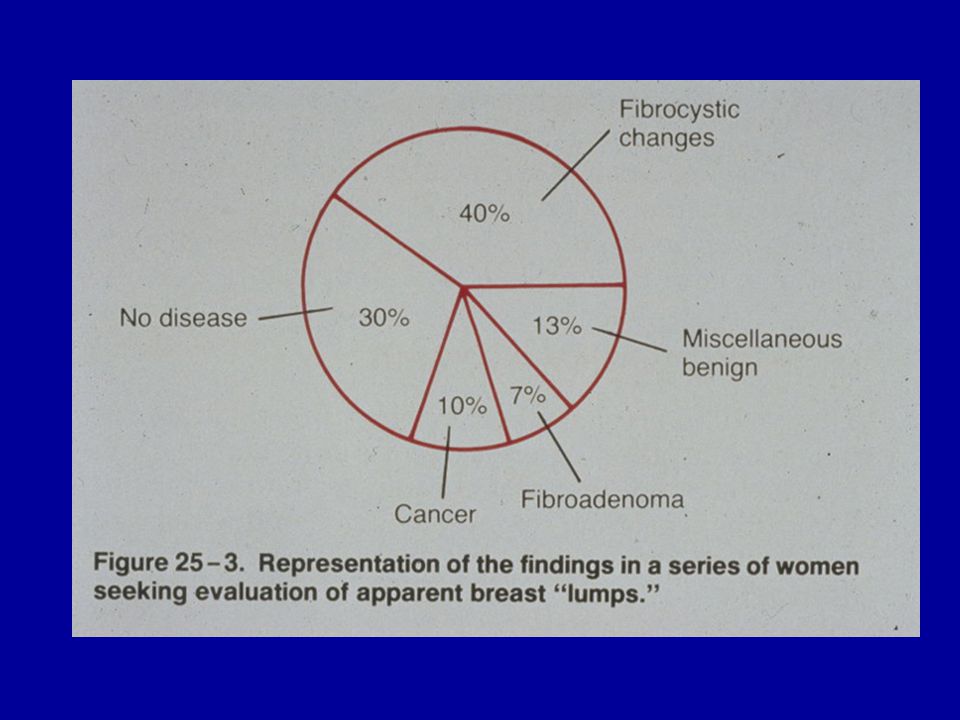
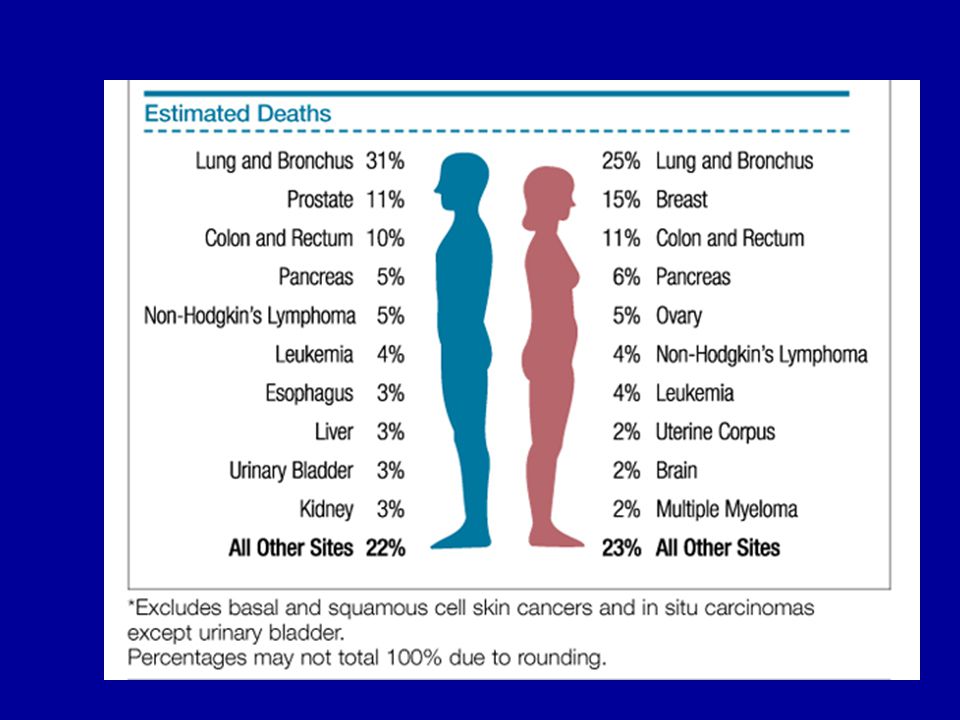
Breast Carcinoma Statistics THE most common cancer in women in the United States (excluding skin cancer) The second most common cause of cancer mortality in women (lung cancer is first) One in eight women will get breast cancer, and one third of women with breast cancer will die of the disease.
 The second most common cause of cancer mortality in women (lung cancer is first) One in eight women will get breast cancer, and one third of women with breast cancer will die of the disease.")
20
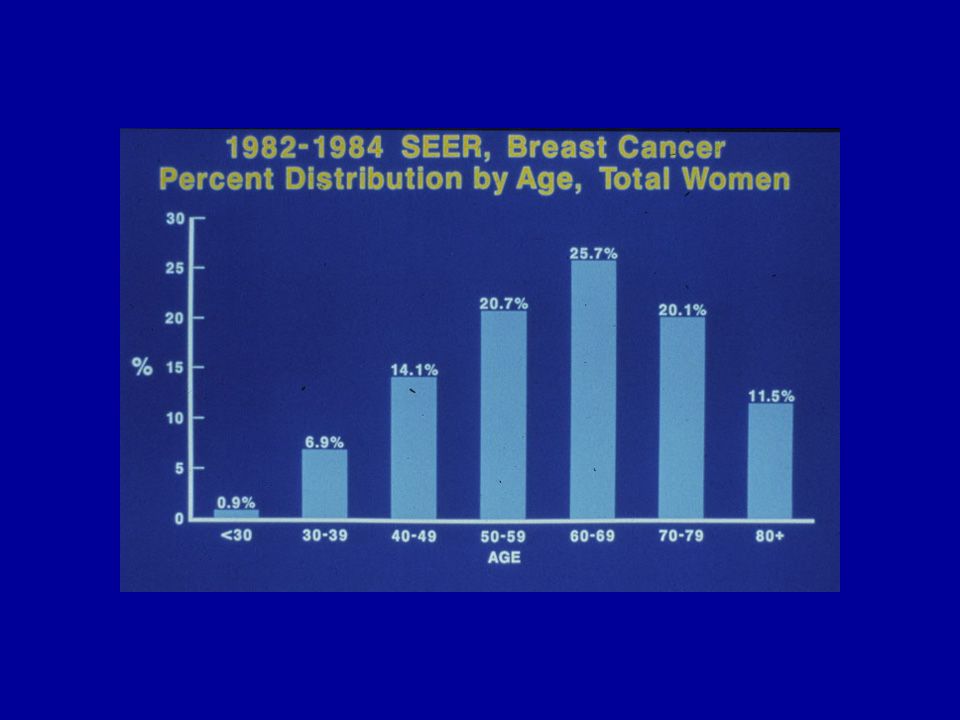
Age-adjusted Cancer Incidence Rates Among Females: 1973 to 1998

22
Risk Factors for Development of Breast Cancer Genetic Environmental Hormonal Radiation History of previous breast pathology

23
Genetic Factors Approximately 10% breast cancers are familial (90% sporadic) Positive Family History, especially in 1st degree relatives (mother, daughter, sister) confers increased risk for breast cancer Risk is greatest with: Relative with BILATERAL disease Relative affected at a YOUNG AGE
 Positive Family History, especially in 1st degree relatives (mother, daughter, sister) confers increased risk for breast cancer Risk is greatest with: Relative with BILATERAL disease Relative affected at a YOUNG AGE")
24
BRCA1 Gene (17q21) Responsible for up to 1/2 of “inherited” breast cancers (5% of cancers) Increased risk of ovarian and colon cancers (“Breast-Ovarian” cancer gene) 85% lifetime risk of breast cancer Breast cancer develops in >50% of these women by age 50 (“Early onset” breast cancer gene) Carried by 1 in 200-400 people
 Responsible for up to 1/2 of inherited breast cancers (5% of cancers) Increased risk of ovarian and colon cancers ( Breast-Ovarian cancer gene) 85% lifetime risk of breast cancer Breast cancer develops in >50% of these women by age 50 ( Early onset breast cancer gene) Carried by 1 in people")
25
BRCA2 Gene (13q) Responsible for up to 70% of inherited breast cancer NOT due to BRCA1 (3.5% of cancers) Characterized by increased risk of breast cancer in women and MALE breast cancer (“Male Breast Cancer” gene) 30-40% lifetime risk of breast cancer
 Responsible for up to 70% of inherited breast cancer NOT due to BRCA1 (3.5% of cancers) Characterized by increased risk of breast cancer in women and MALE breast cancer ( Male Breast Cancer gene) 30-40% lifetime risk of breast cancer")
26
Li-Fraumeni Syndrome (p53) Due to Inherited p53 Tumor Suppressor Gene Mutation (cell cycle checkpoint) Family cancer syndrome characterized by increased risk of breast cancer, osteosarcoma, soft tissue sarcomas, brain tumors, leukemia, other Accounts for approximately 1% of breast cancers detected before age 40
 Due to Inherited p53 Tumor Suppressor Gene Mutation (cell cycle checkpoint) Family cancer syndrome characterized by increased risk of breast cancer, osteosarcoma, soft tissue sarcomas, brain tumors, leukemia, other Accounts for approximately 1% of breast cancers detected before age 40")
27
OTHER Recognized Susceptibility Loci ESR 6q24-27 (Estrogen receptor) ARX11.2-q12(Androgen receptor) PTEN10q22-23 (Cowden’s syndrome)
 ARX11.2-q12(Androgen receptor) PTEN10q22-23 (Cowden’s syndrome)")
28
PUTATIVE Susceptibility Loci ATM11q22 (Ataxia Telangiectasia) HRAS111p15.5 GSTM1(Glutathione-S-transferase) CYP1A1 (Cytochrome P-450) NAT (N-acetyl-transferase) CYP17 (C2:C16-alpha-estrone)
 HRAS111p15.5 GSTM1(Glutathione-S-transferase) CYP1A1 (Cytochrome P-450) NAT (N-acetyl-transferase) CYP17 (C2:C16-alpha-estrone)")
29
Hormonal Factors “Incessant ovulation”: Early menarche, late menopause, nulliparity, late age at first term pregnancy all INCREASE the risk of breast cancer. Oophorectomy before age 35 DECREASES the risk of breast cancer. Oral contraceptive use and hormone replacement therapy may be associated with a SMALL increased risk Etiology: ? hormonal stimulation of proliferation and differentiation of cycling breast epithelium.

30
Environmental Factors 4-5 fold greater incidence of breast cancer in industrialized countries than in less developed countries. Increased risk may be related to: –Higher fat diet –Earlier menarche –Less physical activity –Decreased parity –Later age at parity

31
Radiation Exposure Increased risk of breast cancer after: –Radiation therapy for Hodgkin’s Disease in young women, postpartum mastitis in mothers –Survivors of atomic bomb blasts Increased risk when exposure is at a young age, little increase in risk after age 40 –Indicates that the risk is GREATEST to the developing and hormonally cycling breast

32
4. Histopathologic Risk Factors For Breast Cancer

33
Histopathology Presence of a history of breast pathology increases risk of breast cancer

34
Relative Risk for Invasive Carcinoma Based on Histologic Evaluation of Breast Tissue Without Invasive Carcinoma NON-Proliferative Fibrocystic Changes (1X, No increased risk) –Small simple cysts, apocrine metaplasia, mild epithelial hyperplasia Proliferative Fibrocystic Changes (1.5-2X, Slight increased risk) –Moderate to florid hyperplasia –Sclerosing adenosis –Intraductal papilloma –Fibroadenoma Proliferative Fibrocystic Changes WITH ATYPIA (3-5X, Moderate increased risk) –Atypical ductal hyperplasia –Atypical lobular hyperplasia Carcinoma IN SITU (8-10X, HIGH RISK) –Ductal carcinoma in situ (DCIS) –Lobular carcinoma in situ (LCIS)
 –Small simple cysts, apocrine metaplasia, mild epithelial hyperplasia Proliferative Fibrocystic Changes (1.5-2X, Slight increased risk) –Moderate to florid hyperplasia –Sclerosing adenosis –Intraductal papilloma –Fibroadenoma Proliferative Fibrocystic Changes WITH ATYPIA (3-5X, Moderate increased risk) –Atypical ductal hyperplasia –Atypical lobular hyperplasia Carcinoma IN SITU (8-10X, HIGH RISK) –Ductal carcinoma in situ (DCIS) –Lobular carcinoma in situ (LCIS)")
35
Proliferative Fibrocystic Change WITHOUT Atypia Intraductal Hyperplasia, Moderate to Florid Sclerosing Adenosis Intraductal Papilloma (A benign breast “tumor”) Fibroadenoma (A benign breast “tumor”)
 Fibroadenoma (A benign breast tumor )")
36
Intraductal Hyperplasia Definition: An increase above the normal 2-cell layer thickness –Mild hyperplasia: 3-4 cell layers thick –Moderate hyperplasia: with epithelial tufting and bridging –Severe (florid) hyperplasia: filling and distending ducts
 hyperplasia: filling and distending ducts")
37
Moderate hyperplasia

38
Florid hyperplasia

39
Intraductal Papilloma Discrete benign neoplasm arising from the ductal epithelium of mammary duct May be solitary or multiple Most frequent in the 6th decade Presents as nipple discharge (>75%) which may be bloody, and/or subareolar mass Infarction of the lesion may occur Gross appearance: Papillary growth of ductal epithelium within a duct lumen
 which may be bloody, and/or subareolar mass Infarction of the lesion may occur Gross appearance: Papillary growth of ductal epithelium within a duct lumen")
40
Most papillomas arise in larger mammary ducts

41
Intraductal papilloma

42
Duct lining Stalk

43
Fibrovascular core Myoepithelium

44
Homogeneous lesion with well circumscribed border Fibroadenoma Fibroadenoma (Benign Biphasic Tumor)
")
45
Fibroadenomas will “shell out” at surgery Fibroadenoma

46
Cleft Fibroadenoma

47
Branching compressed ducts Homogeneous stroma Fibroadenoma

48
Proliferative Fibrocystic Change WITH Atypia Atypical Intraductal Hyperplasia Atypical Lobular Hyperplasia

49
Atypical hyperplasia with family history or in a premenopausal woman has a risk of invasive carcinoma similar to DCIS Relative Risk of Invasive Breast Carcinoma

50
5. Breast Pathology Specimens

51
Surgical Procedures to Sample Breast Lesions

52
Fine Needle Aspirate Biopsy of the Breast Analogy- predicting the picture of a completed puzzle by examining the unassembled pieces May be the initial evaluation of a palpable mass Advantages over open biopsy: – Fast – Cost effective – May eliminate an unnecessary procedure Disadvantages: – False negatives and false positives

53
Fine Needle Aspirate Biopsy of the Breast Benign Breast Cytology- – Cohesive groups of uniform ductal epithelial cells without atypia Malignant Breast Cytology- – Poorly cohesive cells with atypia (pleomorphism, enlarged nuclei, large nucleoli, mitotic activity) – May see necrosis The “Triple Test”: – Clinical picture – Mammographic findings – Cytologic findings
 – May see necrosis The Triple Test : – Clinical picture – Mammographic findings – Cytologic findings")
54
Fine Needle Aspiration (FNA)
")
55
FNA Cytology Smear Specimen

56
Fine Needle Aspiration: Benign Ductal Epithelium Versus Breast Cancer

57
Needle Core Biopsy

58
Lumpectomy

59
Mastectomy: Modified Radical

60
6. Breast Cancer Pathology In Situ Carcinomas Invasive Carcinomas Special Subtypes

61
Ductal Carcinoma In Situ (DCIS) Arises in the terminal duct lobular unit (TDLU) and DOES NOT demonstrate invasion through the myoepithelial layer and basement membrane DCIS is a surgically treatable entity The likelihood of developing an invasive carcinoma, or recurrent DCIS varies with a)Histologic subtype of the in situ carcinoma b)Size/ extent of DCIS c)Distance to the margins of excision.
 Arises in the terminal duct lobular unit (TDLU) and DOES NOT demonstrate invasion through the myoepithelial layer and basement membrane DCIS is a surgically treatable entity The likelihood of developing an invasive carcinoma, or recurrent DCIS varies with a)Histologic subtype of the in situ carcinoma b)Size/ extent of DCIS c)Distance to the margins of excision.")
62
Ductal Carcinoma in Situ Clinical: –DCIS usually does not present as a palpable mass, if it does it is usually high grade and a large lesion Mammogram: –The most common method of detection is by identifying mammographic calcifications –The calcifications may be linear and branching...following the lumens of the involved ducts

63
DCIS is confined to within the ductal system

64
Mammography: DCIS

65
Linear and branching calcifications

66
Grossly visible comedo necrosis

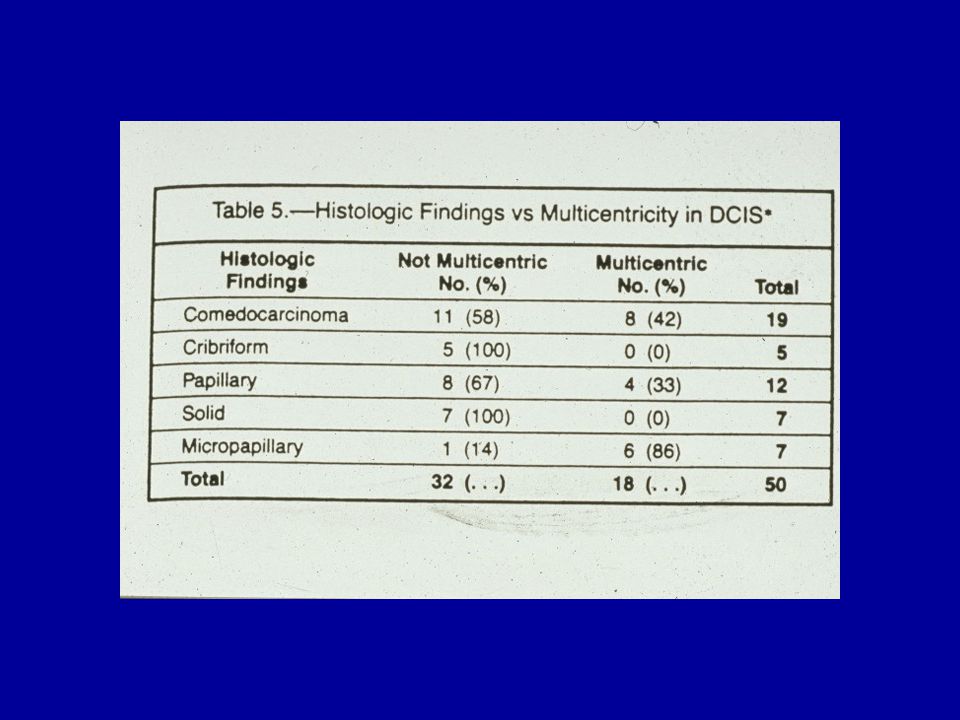
67
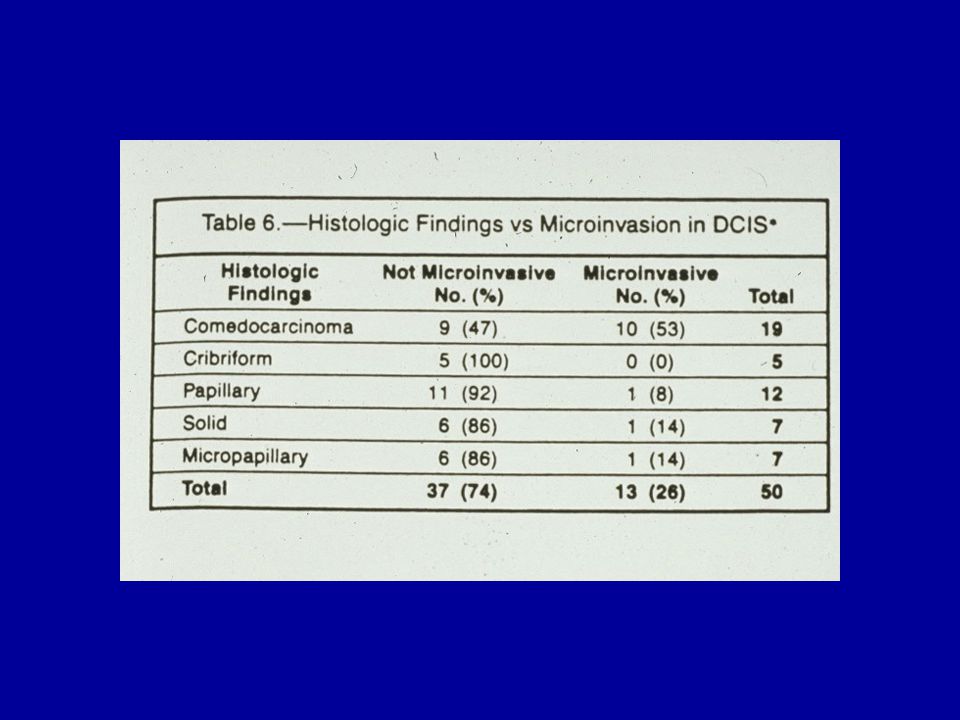
Architectural Patterns of DCIS Comedo –Grade 3 nuclei and necrosis –Often has associated microcalcifications Solid –Carcinoma fills and distends the ducts Micropapillary –Papillary structures that extend into the lumen of the duct Cribriform –Forms a rigid “cartwheel” pattern

68
Comedo necrosis Calcification Tumor cells confined to duct, i.e. DCIS

69
Solid DCIS, uniform monotonous cell population

70
Cribriforming DCIS Secondary lumina

71
Micropapillary DCIS Papillae

72
Nuclear grade 1

73
Nuclear grade 3

74
Surgical excision utilizes anatomic distribution in the lobe of involvement

77
Ductal Carcinoma in Situ, Axillary Metastases? In theory the risk of metastasis is 0% In reality, the risk is <3% –Invasive carcinoma outside the biopsy specimen or not in the plane of sections examined –Invasive carcinoma in a mastectomy specimen not sampled (mastectomy specimens are too large to entirely sample) –Invasive carcinoma not distinguishable at the light microscopic level (present at EM level) –Focus of invasive carcinoma overlooked
 –Invasive carcinoma not distinguishable at the light microscopic level (present at EM level) –Focus of invasive carcinoma overlooked.")
78
Lobular Carcinoma in Situ (LCIS) LCIS considered a “marker of risk for invasive cancer in EITHER breast”, rather than an obligate precursor Proliferation of neoplastic population of cells within the TDLU which usually fill and distend lobules, and may extend into adjacent ducts. Low nuclear grade monotonous cells

79
Lobular carcinoma in situ

81
Invasive Carcinoma of the Breast Infiltrating ductal carcinoma is the most common form of breast cancer. –It is characterized by invasion of the breast stroma by a malignant epithelial cell population derived from the terminal ducts. Clinical: –Often forms a firm palpable mass –May cause skin dimpling (from traction on Cooper’s ligaments) or nipple retraction Mammogram: –Often shows a stellate distortion, may have associated calcifications
 or nipple retraction Mammogram: –Often shows a stellate distortion, may have associated calcifications.")
82
Stellate lesion Calcifications

83
Infiltrating Ductal Carcinoma Gross: –Firm, pale gray/white, gritty, often stellate Micro: –Differentiation depends on: 1) degree of tubule formation 2) nuclear grade 3) mitotic rate –Desmoplastic stromal response: pronounced fibrosis –May have associated calcifications
 degree of tubule formation 2) nuclear grade 3) mitotic rate –Desmoplastic stromal response: pronounced fibrosis –May have associated calcifications")
84
Stellate lesion invading adjacent breast tissue

85
Well differentiated infiltrating ductal carcinoma

86
Poorly differentiated infiltrating ductal carcinoma High grade nuclei High mitotic rate

87
Infiltrating ductal carcinoma, invading and replacing breast stroma

88
Invasion of adipose tissue of breast

89
Infiltrating Lobular Carcinoma 2nd most common form of invasive breast cancer. Gross: –May or may not form a mass Micro: –Single cells and linear profiles of malignant cells with low nuclear grade, may form a targetoid pattern, may show intracytoplasmic vacuoles, characteristically show minimal mitotic activity –LACKS a desmoplastic stromal response –Show LOSS of E-cadherin membrane staining (a cytoplasmic membrane adhesion molecule)
.")
90
Infiltrating Lobular Carcinoma Often clinically and mammographically occult, and therefore microscopically more extensive than expected Propensity to be multifocal and bilateral Propensity to metastasize to unusual sites: –Gyn tract, GI tract Same prognosis as infiltrating ductal carcinoma, when matched for stage Usually ER/PR positive, C-erbB-2 negative Pleomorphic lobular variant: high nuclear grade, more aggressive course

91
Linear arrangement of malignant cells

92
Positive cytokeratin stain confirming the epithelial nature of lobular carcinoma

93
Infiltrating ductal carcinoma, in contrast, with architectural distortion

94
Uncommon types of Invasive Carcinoma of the Breast Mucinous (Colloid) Carcinoma –Older women –Malignant cells floating in pools of mucin –Better prognosis than invasive ductal or lobular Tubular Carcinoma –Younger women –Well differentiated, characterized by haphazardly arranged tubules –Excellent prognosis
 Carcinoma –Older women –Malignant cells floating in pools of mucin –Better prognosis than invasive ductal or lobular Tubular Carcinoma –Younger women –Well differentiated, characterized by haphazardly arranged tubules –Excellent prognosis")
95
Mucin “Floating” malignant cells Mucinous (Colloid) Carcinoma
 Carcinoma")
96
Tubular Carcinoma Well formed tubules

97
Inflammatory Carcinoma Defined as invasive carcinoma involving superficial dermal lymphatic spaces Poor prognosis (T3 disease) Erythema and induration of the skin, so called “inflammatory changes” –Peau d’orange-dimpling of involved skin due to retraction caused by lymphatic involvement and obstruction
 Erythema and induration of the skin, so called inflammatory changes –Peau d’orange-dimpling of involved skin due to retraction caused by lymphatic involvement and obstruction")
98
Inflammatory carcinoma

99
Inflammatory carcinoma: dermal lymphatic spaces containing tumor cells

100
Paget’s Disease Invasion of the SKIN of the nipple or areola by malignant cells, singly or in small nests Associated with an underlying cancer: either IN SITU OR INVASIVE carcinoma Clinically-erythema, scaling, ulceration

101
Paget’s disease: nipple ulceration

102
Paget’s Disease of the Nipple Intra-epidermal adenocarcinoma cells

103
Phyllodes Tumor (Cystosarcoma Phyllodes) Biphasic breast tumor consisting of a benign glandular component and malignant stromal component with leaf-like processes (“adenosarcoma”) ?Malignant counterpart to fibroadenoma –Coexistant fibroadenomas in 40%, may arise in fibroadenoma (history of stable mass that undergoes enlargement) Clinical Presentation –Discrete, solitary, firm to hard mass –Larger size > 4 cm and/or history of rapid growth favors phyllodes tumor over fibroadenoma –Median age 45 years (~15 years older than fibroadenoma)
 Biphasic breast tumor consisting of a benign glandular component and malignant stromal component with leaf-like processes ( adenosarcoma ) Malignant counterpart to fibroadenoma –Coexistant fibroadenomas in 40%, may arise in fibroadenoma (history of stable mass that undergoes enlargement) Clinical Presentation –Discrete, solitary, firm to hard mass –Larger size > 4 cm and/or history of rapid growth favors phyllodes tumor over fibroadenoma –Median age 45 years (~15 years older than fibroadenoma)")
104
Phyllodes Tumor-Pathology Micro: –Stromal and epithelial tissue in “leaf-like” arrangement –*Stroma (compared to fibroadenoma) Increased cellularity and expansion (“stromal overgrowth”) Increased mitotic rate Cellular pleomorphism
 Increased cellularity and expansion ( stromal overgrowth ) Increased mitotic rate Cellular pleomorphism")
105
Note the size!

106
“Leaf-like” architecture

107
Stromal expansion

108
Increased mitotic activity

109
Stromal component of Phyllodes invading adipose tissue

110
7. Male Breast Pathology Gynecomastia (Benign) Male Breast Cancer (Malignant)
 Male Breast Cancer (Malignant)")
111
Gynecomastia Potentially reversible enlargement of the male breast Clinical- Unilateral or bilateral subareolar mass with or without pain Microscopic-Ductal and stromal proliferation Etiology- Systemic disease-hyperthyroidism, cirrhosis, chronic renal failure –Drugs-cimetidine, digitalis, tricyclic antidepressants, marijuana –Neoplasms-pulmonary, testicular germ cell tumors –Hypogonadism: testicular atrophy, exogenous estrogen, Klinefelter’s syndrome

112
Gynecomastia

113
Periductal edema Epithelial hyperplasia

114
Carcinoma of the Male Breast < 1% of breast cancer Infiltrating ductal carcinoma is by far the most common type Tends to present at a more advanced stage –Less fat and breast tissue, therefore involvement of chest wall occurs earlier Similar prognosis when matched, stage for stage, with female breast cancer Associated with inherited BRCA2 mutation

115
8. Prognostic Markers and Staging

116
Prognostic Markers Routinely Clinically in Use Histopathologic grade, subtype Stage: Tumor size, lymph Node, Metastases (TNM) Steroid hormone receptors (ER and PR) Oncogene expression (HER-2/neu/c-erbB-2)
 Steroid hormone receptors (ER and PR) Oncogene expression (HER-2/neu/c-erbB-2)")
117
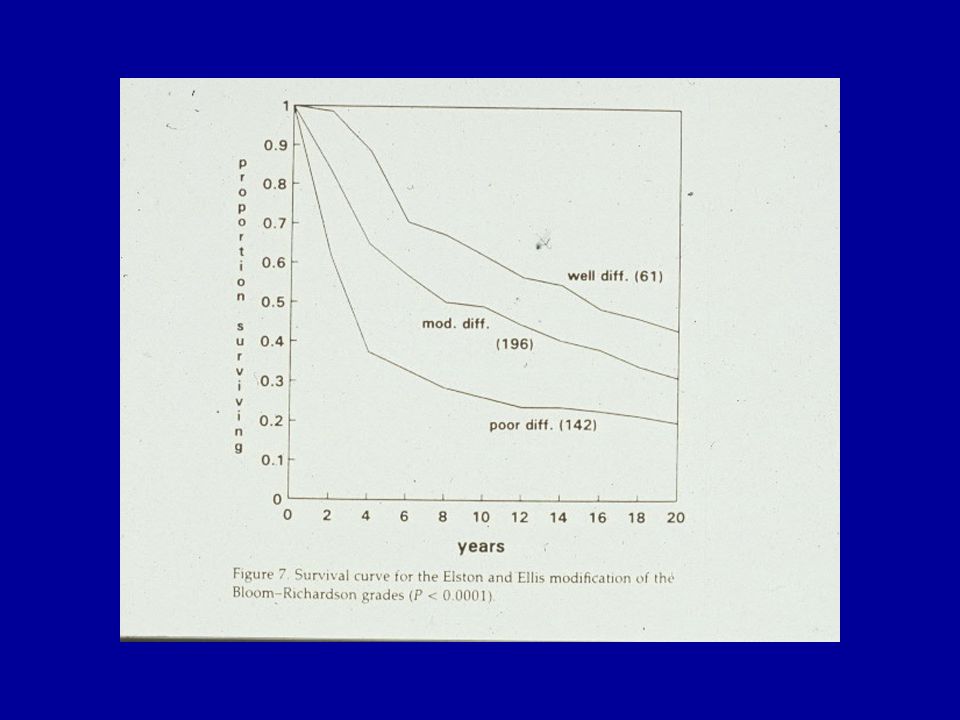
Histopathologic Grade

119
T= primary tumor size N= presence or absence of nodal metastases M= presence or absence of distant metastases TNM Clinical Pathologic Staging

120
The presence of axillary lymph node metastasis is the most important prognostic indicator

122
Regional Nodal Stations for Breast Cancer Staging

123
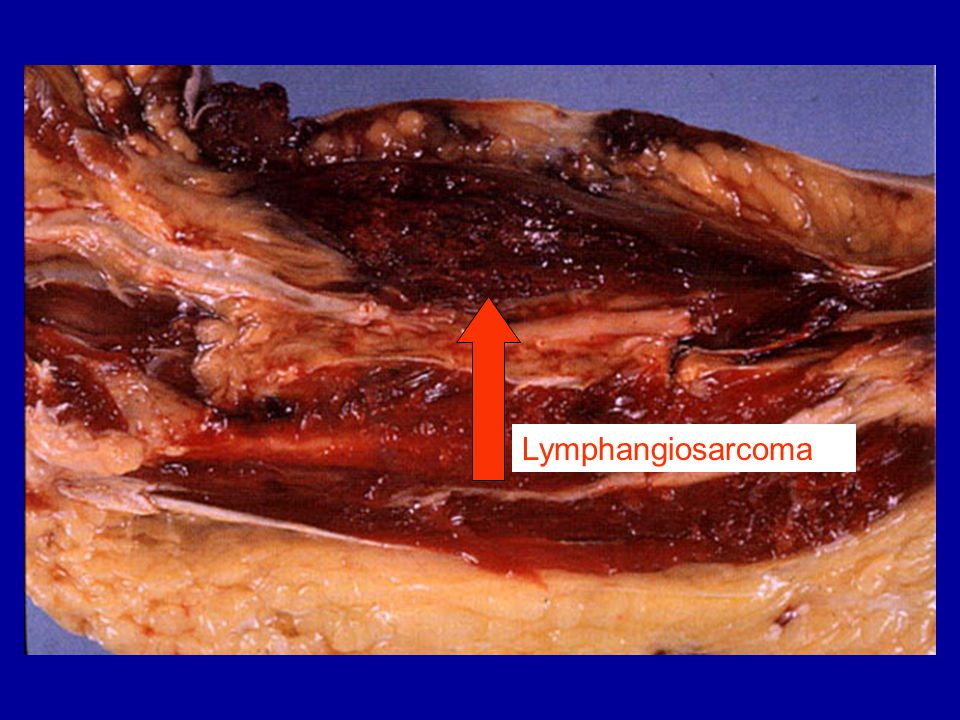
Morbidity (and Mortality!) from Axillary Lymph Node Dissection Arm edema Increased risk of infection Nerve injury Winged scapula Rare but devastating complication: development of lymphangiosarcoma in the setting of long-term lymphedema –High grade sarcoma with rapid spread and dismal prognosis
 from Axillary Lymph Node Dissection Arm edema Increased risk of infection Nerve injury Winged scapula Rare but devastating complication: development of lymphangiosarcoma in the setting of long-term lymphedema –High grade sarcoma with rapid spread and dismal prognosis")
124
Lymphangiosarcoma

126
Sentinel Lymph Nodes Sentinel Lymph Node- the first draining lymph node from a specified site Identified at UNC using two methods simultaneously –Radioactive technetium labeled sulfur colloid –Isosulfan blue dye Currently: –Sentinel LN(s) submitted to histology and examined at multiple levels (at least 3) by H&E and, if necessary, also with immunohistochemistry –The remainder of the axilla is also dissected
 submitted to histology and examined at multiple levels (at least 3) by H&E and, if necessary, also with immunohistochemistry –The remainder of the axilla is also dissected")
127
Significance of Sentinel Lymph Nodes Sentinel lymph node examination is a valid method of determining axillary status Efforts have shown improved detection of micrometastases through concentrated examination of the most likely positive node(s) Complete removal of the axillary lymph nodes is no longer standard treatment for all patients with invasive disease!
 Complete removal of the axillary lymph nodes is no longer standard treatment for all patients with invasive disease!")
128
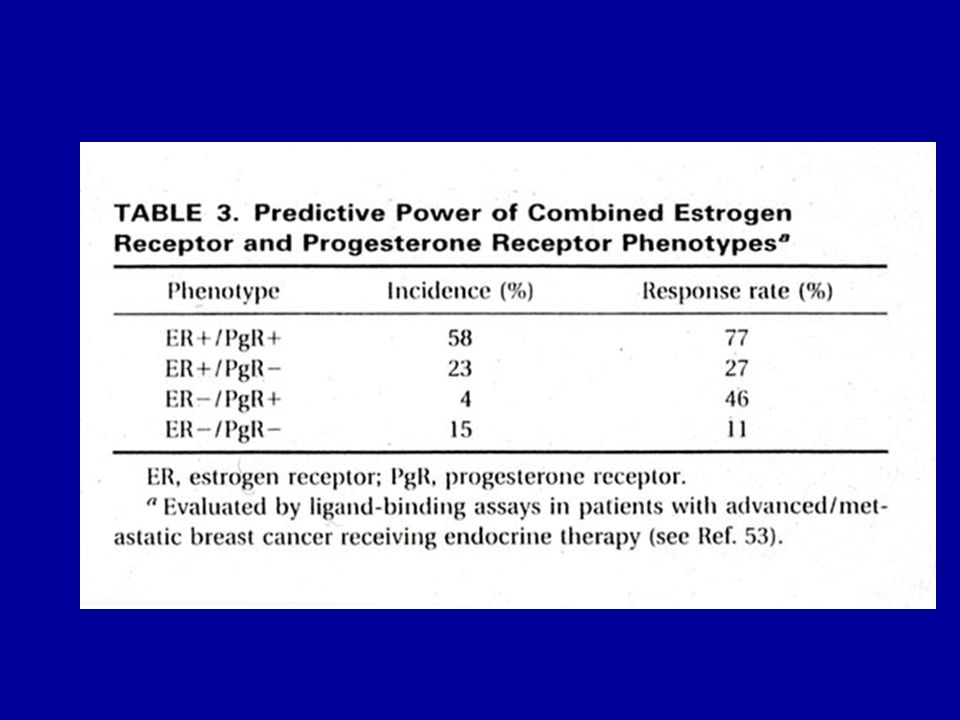
Estrogen and Progesterone Receptors (ER, PR) >50% of carcinomas are ER positive, slightly less are PR positive Hormone receptor positivity is associated with longer disease-free survival, better overall survival, and longer survival after recurrence Hormone receptor positivity predicts better response to hormonal (anti-estrogen) therapy: –ER+PR+ > ER-PR+ > ER+PR- > ER-PR-
 >50% of carcinomas are ER positive, slightly less are PR positive Hormone receptor positivity is associated with longer disease-free survival, better overall survival, and longer survival after recurrence Hormone receptor positivity predicts better response to hormonal (anti-estrogen) therapy: –ER+PR+ > ER-PR+ > ER+PR- > ER-PR-")
130
c-erbB-2 (HER-2/neu) Oncogene which shares extensive sequence homology with epidermal growth factor receptor (EGFR) Overexpression by invasive carcinoma associated with: –Decreased time to recurrence –Decreased overall survival
 Oncogene which shares extensive sequence homology with epidermal growth factor receptor (EGFR) Overexpression by invasive carcinoma associated with: –Decreased time to recurrence –Decreased overall survival")
131
Strong overexpression of HER-2/neu (c-erbB- 2) at cell surfaces
 at cell surfaces")
132
c-erbB-2 ( HER2/neu) Herceptin® –Recombinant humanized anti-HER2 –Inhibits growth of breast cancer cells that overexpress c-erbB-2 –Enhances tumoricidal effects of doxorubicin and taxol –Approved by the FDA September 1998 –Used in patients with metastatic disease and c-erbB-2 overexpression
 Herceptin® –Recombinant humanized anti-HER2 –Inhibits growth of breast cancer cells that overexpress c-erbB-2 –Enhances tumoricidal effects of doxorubicin and taxol –Approved by the FDA September 1998 –Used in patients with metastatic disease and c-erbB-2 overexpression")
134
HER-2 Gene Amplification by FISH

137
Other Prognostic Markers DNA content (DNA ploidy) Tumor suppressor genes (p53, others) Angiogenesis (Microvessel density) Proteases Gene profiling by microarrays***
 Tumor suppressor genes (p53, others) Angiogenesis (Microvessel density) Proteases Gene profiling by microarrays***")
138
9. Models of Breast Carcinogenesis

139
Models of Breast Carcinogenesis Multistage Model of Carcinogenesis Skip-stage Model of Carcinogenesis Divergence vs. Convergence Hypothesis

140
Multistage Model of Carcinogenesis Normal Atypical Hyperplasia Carcinoma In Situ Invasive Carcinoma Metastasis

141
“Skip Stage” Model of Carcinogenesis Normal Atypical Hyperplasia Carcinoma In Situ Invasive Carcinoma Metastasis

142
“Skip Stage” Model of Carcinogenesis Normal Atypical Hyperplasia Carcinoma In Situ Invasive Carcinoma Metastasis

143
Convergence Hypothesis

144
Divergence Hypothesis

145
10. Tissue Sampling Techniques

146
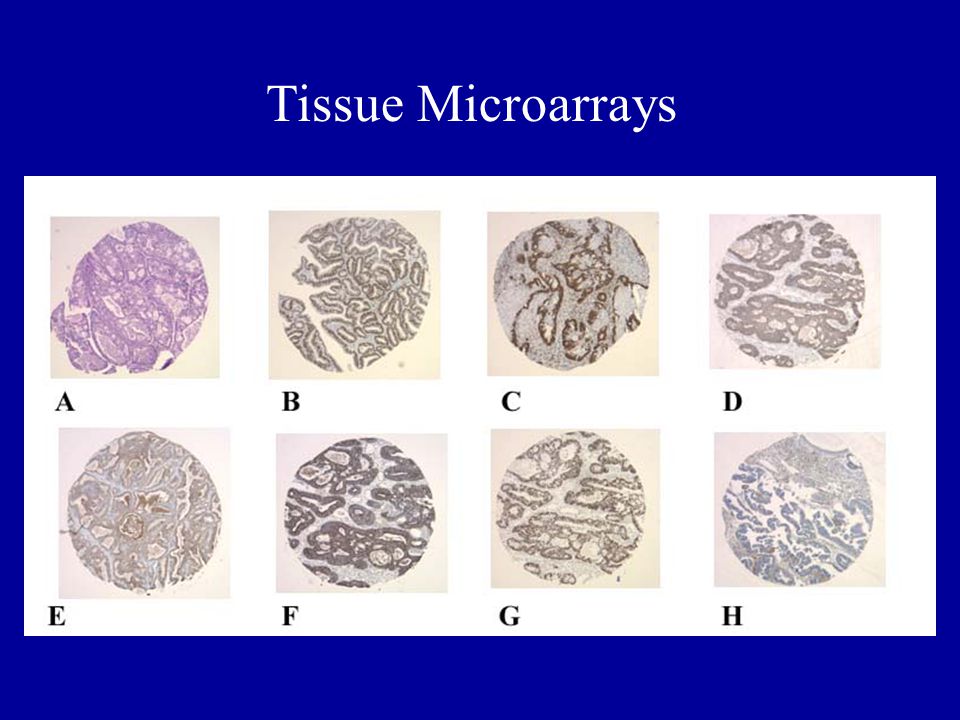
Tissue Microarrays

148
Microdissection of a single duct of DCIS Microdissection of single cells Microdissection Methodologies

Similar presentations








>")















