Download presentation
Presentation is loading. Please wait.

1
LIFE TIME HAPPINESS Dr.Sarma@works
Asthma is a complex disease that requires a long-term and multifaceted solution. This includes educating, treating, and providing ongoing medical care and monitoring for people with the disease, changing behaviors that lead to asthma or make it worse, and eliminating or avoiding triggers. All the topics we discuss today total “A Public Health Response to Asthma.”

2
When you can't breathe, nothing else matters®
American Lung Association

3
Important Announcement
CD format of today’s presentation is ready 1. Asthma, COPD and Basics of Spirometry In addition it, also contains 2. ECG workshop presented earlier 3. Guidelines on Hypertension treatment This can be used in Computer & DVD player

4
COPD and Asthma Resources
ACCP ATS BTS COPD profess. GOLD NICE Chest Net CDC NAEPP COPD Rapid series by ELSEVIER

5
CHRONIC LUNG DISEASES Pulmonary Tuberculosis Restrictive lung diseases
Suppurative lung disease Obstructive lung diseases Bronchial Asthma Chronic bronchitis Emphysema and Their differentiations

6
AN OVERVIEW - GINA MANAGEMENT GUIDE LINES
ASTHMA AN OVERVIEW - GINA MANAGEMENT GUIDE LINES Dr. Sarma.R.V.S.N., M.D., M.Sc (Canada) Consultant Physician and chest specialist # 5, Jayanagar, Tiruvallur , (4116)
 Consultant Physician and chest specialist. # 5, Jayanagar, Tiruvallur , (4116)")
7
WHAT IS ASTHMA ? Primarily it is an allergic inflam-matory disorder of the airways Infiltration of mast cells, eosinophils and lymphocytes Secondary broncho-constriction Airway hyper-responsiveness Recurrent episodes of wheezing, coughing and shortness of breath Airflow limitation is variable and often reversible and wide spread

8
BURDEN OF ILLNESS 15- 20 million asthmatics in India.
A recent study conducted in Delhi established asthma prevalence to be 12% in school children. Significant cause of school/work absence. Health care expenditures very high. Morbidity and mortality are on the rise.

9
THE HUGE GAP Patients are not detected Do not seek medical attention
No access to health service Stigma associated with the label Broken marriages, alliances Missed diagnosis (bronchitis, LRTI)
")
10
Symptoms- (shortness of breath, cough, wheeze)
MECHANISM OF ASTHMA Risk Factors (for development of asthma) INFLAMMATION Airway Hyper responsiveness Airflow Limitation Symptoms- (shortness of breath, cough, wheeze) Risk Factors (for exacerbations)
 INFLAMMATION. Airway Hyper responsiveness. Airflow Limitation. Symptoms- (shortness of breath, cough, wheeze) Risk Factors (for exacerbations)")
11
ASTHMA : PATHOLOGY

12
RISK FACTORS FOR ASTHMA
Predisposing Factors Atopy (↑ IgE) Causal Factors Indoor Allergens Domestic mites Animal Allergens Cockroach Allergens Fungi moulds Outdoor Allergens Pollens Fungi, RSV Occupational Sensitizers Contributing Factors Respiratory infections Small size at birth Diet Air pollution Outdoor pollutants Indoor pollutants Smoking Passive Smoking Active Smoking
 Causal Factors. Indoor Allergens. Domestic mites. Animal Allergens. Cockroach Allergens. Fungi moulds. Outdoor Allergens. Pollens. Fungi, RSV. Occupational Sensitizers. Contributing Factors. Respiratory infections. Small size at birth. Diet. Air pollution. Outdoor pollutants. Indoor pollutants. Smoking. Passive Smoking. Active Smoking.")
13
HOUSE DUST MITE Use bedding encasements Wash bed linens weekly
Avoid down fillings Limit stuffed toys to those that can be washed Reduce humidity level Dust mites thrive in soft furnishings like pillows, mattresses, carpets, and drapes. These microscopic organisms give off particles that cause allergic reactions when inhaled. They need moisture to survive and therefore thrive in humid environments. Decreasing the number of dust mites to which people with asthma are exposed may help control their asthma. One key way of doing this in the bedroom is by using mattress and pillow case covers. These bedding encasements, which are available commercially, may be plastic or vinyl and are covered with cotton, nylon, or knit fabric. They provide a barrier between the dust mites and the person with asthma. A sheet and pillow case are usually placed over the encasement for increased comfort. Any linens placed over the encasements should be washed weekly in hot water. Down-filled pillows, quilts, or comforters should not be used. Down filling consists of tiny feathers that contain large numbers of dust mites. Also, stuffed animals and clutter should be removed from the bedroom. If a child with asthma wants to play or sleep with a stuffed toy, wash the toy frequently in hot water, or put it in the freezer for a few hours every 2 weeks. Freezing cold kills dust mites as effectively as hot water. The hot water needs to be about 130 degrees to kill mites, and this is generally hotter than most household hot water. If you re-set your hot water heater thermostat to 130 degrees, you have to take other precautions to prevent scalding. Another thing to consider in the bedroom is getting rid of fabric curtains and replacing them with shades or mini-blinds. Replace upholstered chairs with plastic or wood, and, if possible, get rid of carpeting in favor of vinyl or wood floors with area rugs that can be shaken out frequently. Because dust mites need high humidity, try to keep the humidity levels in your home to under 50%. In hot, humid climates, this requires the use of air conditioning and possibly dehumidifiers. In dryer, cooler climates, you may be able to achieve this by opening windows and ensuring good air flow.

14
COCKROACHES Remove as many water and food sources as possible to avoid cockroaches. Allergy to cockroaches is an important risk factor for worsening asthma. Decreasing exposure to cockroaches in the home can help reduce asthma attacks. To do this, remove as many water and food sources as possible because cockroaches need food and water to survive. That is why kitchens and bathrooms are areas where we commonly see cockroaches. Food, including pet food, or water anywhere in the home will attract roaches, so immediately wash soiled dishes, throw away discardable food containers, and remove standing water from all rooms. Keep trash in closed containers, and keep food covered and put away. Discard grocery bags, newspapers, cardboard boxes, and other clutter. People tend to eat where they watch television. As a result, cockroaches and cockroach remains are frequently found in living rooms, family rooms, and bedrooms. You may find cockroaches any place where food is eaten and crumbs are left behind. These areas will need to be vacuumed or swept at least every 2-3 days to get rid of food crumbs.

15
PETS People allergic to pets should not have them in the house.
At a minimum, do not allow pets in the bedroom. Animals are a common source of allergens. They shed fur and feathers; they leave saliva, urine, and feces. Cats and rodents are potent asthma sensitizers, whereas dogs cause less allergic sensitivity than other mammals. People with asthma may find that their pets trigger an attack. The simplest solution to this situation is, of course, to find another home for the pet. However, some pet owners may be too emotionally attached to their pets or unable to locate a safe new home for the animal. Fortunately, other steps can be taken to reduce the impact of pet allergens in the home. At the very least, any animal causing an allergic reaction should not be allowed in the bedroom of the affected person. Pets such as cats and dogs should be kept outside as much as possible. Frequent vacuuming will help to minimize the presence of the allergen. If the room has a hard surface floor, it should be damp mopped weekly. If you have carpeting, try to use a vacuum cleaner equipped with a high-efficiency particle arresting or HEPA filter. At a minimum, use specifically designed micro-filtration vacuum cleaner bags, which can be purchased at any department store. Use pet beds or blankets that are washable, and wash them weekly. If the veterinarian says it’s OK, bathe the animal every week or two.

16
Eliminating mold may help control asthma exacerbations.
MOLDS - FUNGUS When mold is inhaled, it can cause asthma attacks. Mold grows outdoors and indoors, especially in humid areas like bathroom showers and basements. Eliminating mold throughout the home can help control asthma attacks. To do this, one needs to keep humidity levels between 35 and 50%. A gauge called a hygrometer can be used to monitor humidity levels. When the humidity is above 60%, a dehumidifier or air conditioner should be used and the windows kept closed. If a humidifier must be used, it should be cleaned weekly with diluted bleach, and the water should be changed daily so that mold does not grow. In the kitchen, use an exhaust fan to remove water vapor when cooking. Each week, empty water pans which are found below self-defrosting refrigerators. Remove spoiling foods immediately. Empty trash frequently to keep the home clean. In the bathroom, use an exhaust fan or open a window to remove humidity after showering. Use a squeegee to remove excess water from the shower stall, tub, and tiles. Vent a clothes dryer by attaching a vent hose to it and running the hose outside. Dry clothes immediately after washing, either in a dryer or by hanging clothes outside. Do not lay carpet and pad on a concrete floor. Correct seepage or flooding problems, and remove any previously flooded carpets. Ideally, people with asthma should not have bedrooms on the basement level, especially if the basement tends to be humid. Also, they should not have potted plants in their bedroom because the soil is a breeding ground for mold. Eliminating mold may help control asthma exacerbations.

17
DIAGNOSIS OF ASTHMA History and patterns of symptoms
Physical examination Measurements of lung function Peak flow meter Spirometry

18
PATIENT HISTORY Has the patient had an attack or recurrent episodes of wheezing? Does the patient have a troublesome cough, worse particularly at night, or on awakening? Does the patient cough after physical activity (eg. Playing)? Does the patient have breathing problems during a particular season (or change of season)?
 Does the patient have breathing problems during a particular season (or change of season)")
19
MAIN SYMPTOM CLUES Do the patient’s colds ‘go to the chest’ or take more than 10 days to resolve? Does the patient use any medication ? (e.g. bronchodilator) when symptoms occur ? - Is there a (relief) response? If the patient answers “YES” to any of the above questions, suspect asthma. Remember, the commonest cause of persistent cough is asthma
 when symptoms occur - Is there a (relief) response If the patient answers YES to any of the above questions, suspect asthma. Remember, the commonest cause of persistent cough is asthma.")
20
PHYSICAL EXAM Wheeze - Usually heard without a stethoscope Dyspnoea -
Rhonchi heard with a stethoscope Use of accessory muscles Remember - Absence of symptoms at the time of examination does not exclude the diagnosis of asthma

21
PHYSICAL EXAM Hyper-expansion of the thorax
Increased nasal secretions or nasal polyps Atopic dermatitis, eczema, or other allergic skin conditions In the absence of specific symptoms, some physical findings still increase the possibility that a patient has asthma. These include: A wheezing sound in the lungs Hyperexpansion of the chest area (expansion of the area between the neck and abdomen), especially in children Hunched shoulders Chest deformity Nasal swelling Increased secretions or polyps, and Indications of an allergic skin condition. The physician may suggest that the patient be tested for allergies to help isolate substances to which he or she has a strong allergic reaction.
, especially in children. Hunched shoulders. Chest deformity. Nasal swelling. Increased secretions or polyps, and. Indications of an allergic skin condition. The physician may suggest that the patient be tested for allergies to help isolate substances to which he or she has a strong allergic reaction.")
22
Peak Flow Meter is a basic tool in a GPs office
SCREENING TEST Diagnosis of asthma can be suspected by demonstrating the presence of airway obstruction using Peak flow meter. PEFR amplitude ? Peak Flow Meter is a basic tool in a GPs office

23
DIAGNOSTIC TEST Diagnosis of asthma can be confirmed by demonstrating the presence of reversible airway obstruction using Spirometry.
24
SPIROMETRY Let me now take you through to the understanding of the basics of spirometry
25
SPIROMETRY Basic Issues

26
LUNG FUNCTION TESTS Tests of Ventilation Tests of Diffusion
Tests of Perfusion Tests for V-P Mismatch

27
LUNG FUNCTION TESTS Tests of Ventilation Tests of Diffusion
Tests of Perfusion Tests for V-P Mismatch

28
VENTILATION Peak Expiratory Flow Rate
Simple, Peak flow meter is used Flow volume loop , Flow time curve Detailed, Spirometry is used

29
PEAK FLOW METER Diagnosis of ASTHMA or COPD can be
confirmed by demonstrating the presence of airway obstruction using Spirometry.

30
PEFR - Pros and Cons Advantages Disadvantages With in 1 to 2 minutes,
Inexpensive (meter costs less than Rs.1000) Simple, useful for frequent follow up use Disadvantages Very much effort dependent Insensitive to small changes Small airways cannot be assessed Large inter & intra subject variation;↓accurate
 Simple, useful for frequent follow up use. Disadvantages. Very much effort dependent. Insensitive to small changes. Small airways cannot be assessed. Large inter & intra subject variation;↓accurate.")
31
SPIROMETRY

32
Spirometry - Pros and Cons
Advantages Evaluates smaller as well as larger airways Relatively easy to use and maintain Reversibility can be tested with IBD and steroids Diagnostic as well as management assessments Disadvantages Cost about 50,000 + computer and printer Takes time to perform – 10 to 15 minutes Requires training – at least one day course

33
Spirometry Maneuver In single breath test
A few normal tidal respirations Then deeeeep inspiration Momentary breath holding Very forced and fast expiration As hard and as fast as he/she can blow out Then deep, quick and full inspiration Repeat at least 3 times – take the best

34
Spirometry Results FVC Forced Vital Capacity
FEV1 Forced Expiratory Volume in the first second FEV1÷FVC Ratio of the above two PEFR Peak Expiratory Flow Rate FET Forced Expiratory Time

35
Spirometry Normal Values
There are no fixed ‘Normal’ values Dependent on age, sex, ht, wt, ethnicity Observed value expressed as predicted value % FVC Normal if > 80% of predicted FEV1 Normal if > 80% of predicted FEV1/FVC At least 75% PEFR Normal if > 80% of predicted FET Less than 4 seconds

36
Obstructive v/s Restrictive
Parameter Normal Obstructive Restrictive Problem ‘Air out’ and ‘Air in’ normal Unable to get ‘Air out’ ‘Air in’ FVC 80 % of pred Normal or ↓ ↓,↓TLC FEV1 ↓-80% or less FEV1 ÷ FVC Min. of 75% ↓-70% or less Normal or ↑ PEFR FET in sec Less than 4 Prolonged > 4 Normal - < 4

37
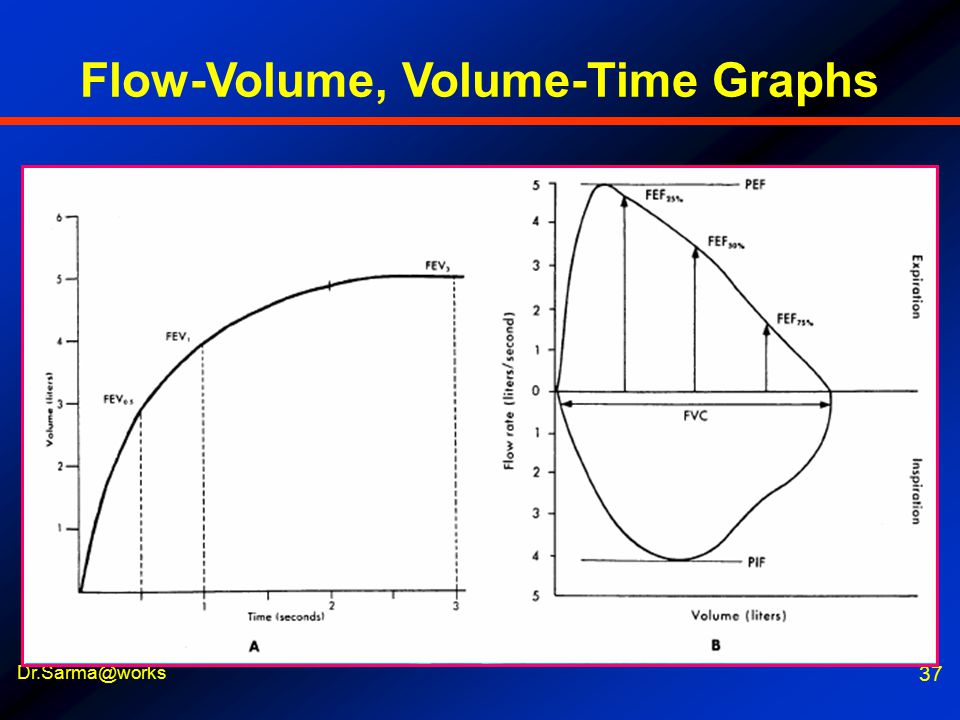
Flow-Volume, Volume-Time Graphs
38
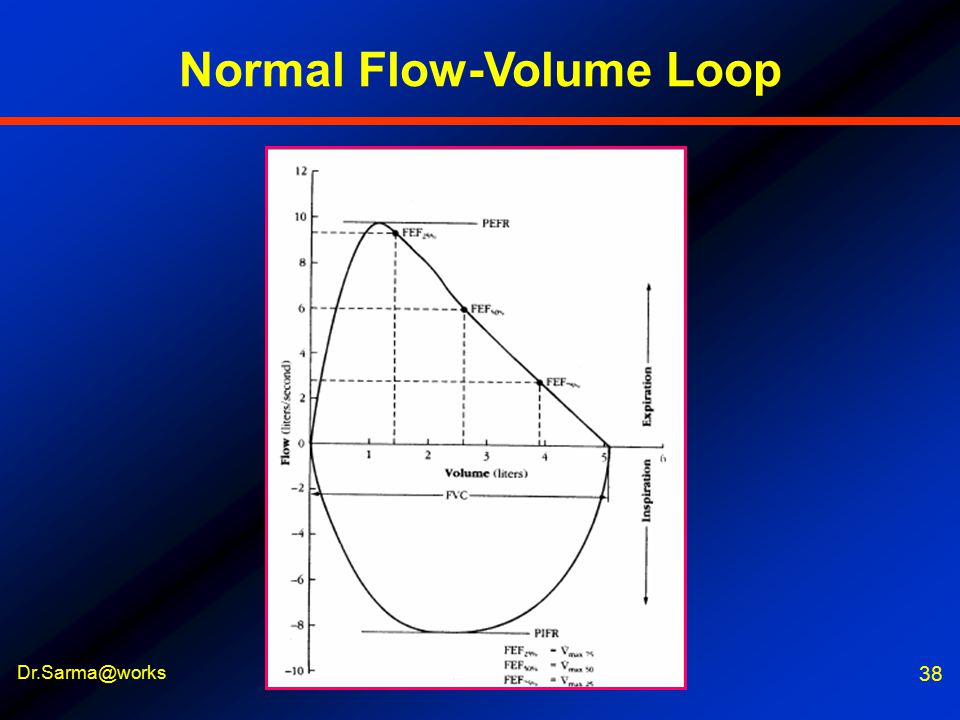
Normal Flow-Volume Loop
39
Flow-Volume Loop in disease
ASTHMA COPD ILD Mild reversible obstruc Severe irreversible obstr Severe restrictive dis

40
Office Spirometry

41
BACK TO ASTMA Now, with this understanding of spirometry, let us proceed to look at the management of Asthma
42
CLASSIFICATION OF SEVERITY
CLASSIFY SEVERITY Clinical Features Before Treatment Nighttime Symptoms Symptoms FEV1 STEP 4 Severe Persistent Continuous Limited physical activity <60% predicted Variability >30% Frequent STEP 3 Moderate Persistent Daily Use b2-agonist daily Attacks affect activity >60%-<80% predicted Variability >30% >1 time week STEP 2 Mild Persistent >80% predicted Variability 20-30% >1 time a week but <1 time a day >2 times a month < 1 time a week Asymptomatic and normal PEF between attacks STEP 1 Intermittent >80% predicted Variability <20% <2 times a month The presence of one of the features of severity is sufficient to place a patient in that category. Global Initiative for Asthma (GINA) WHO/NHLBI, 2002
 WHO/NHLBI,")
43
GOALS IN ASTHMA CONTROL
Achieve and maintain control of symptoms Prevent asthma episodes or attacks Minimal use of reliever medication No emergency visits to doctors or hospitals Maintain normal activity levels, including exercise Maintain pulmonary function as close to normal as possible Minimal (or no) side effects from medicine
 side effects from medicine.")
44
Preventers (long term) Peak Flow meter Spirometry Patient education
TOOL KIT WE HAVE Relievers (Quick) Preventers (long term) Peak Flow meter Spirometry Patient education
 Preventers (long term) Peak Flow meter. Spirometry. Patient education.")
45
ASTHMA Rx. in INDIA TOADAY
Completely control symptoms and Make their life normal As good as abroad (even better) General practice physicians Doesn’t need Chest Physicians !
 General practice physicians. Doesn’t need Chest Physicians !")
46
IT IS A DUAL PROBLEM Bronchial inflammation – perpetual
Allergic inflammation and edema Inflammatory mediators – perpetuate edema and excite bronchospasm Bronchial hyper reactivity to triggers Bronchospasm – acute attacks This needs two different types of medicines – relievers & preventers

47
WHAT ARE RELIEVERS ? Spasm needs reliever Bronchodilator drugs
Rescue medications Quick relief of symptoms Used during acute attacks Action lasts for 4-6 hrs Not for regular use at all

48
RELIEVERS Short acting 2 agonists - SABA Salbutamol, Terbutaline
Levo-salbutamol (Levolin) Anti-cholinergics Ipatropium Xanthines Theophylline (Deriphyllin group)
 Anti-cholinergics. Ipatropium. Xanthines. Theophylline (Deriphyllin group)")
49
WHAT ARE PREVENTERS ? Prevent future attacks
Reduce allergic inflammation Reduce inflammatory mediators Reduce hyper-responsiveness Long term control of asthma Prevent airway remodeling For regular use – well or ill

50
PREVENTERS Corticosteroids Xanthines Prednisolone, Betamethasone
Beclomethasone, Budesonide Fluticasone Long acting 2 agonists-LABA Bambuterol, Salmeterol Formoterol, Bambuderol Anti-leukotrienes Montelukast, Zafirlukast, Pranlukast Xanthines Theophylline SR Mast cell stabilizers Sodium cromoglycate Nedocromil sodium Ketotifen, Ceterizine Combinations Salmeterol/Fluticasone Formoterol/Budesonide Salbutamol/Beclomethasone

51
CERTAIN ABBREVIATIONS
ICS Inhaled corticosteroids IBD Inhaled bronchodilators SABA Short acting βagonists LABA Long acting βagonists LTA Leukotrine antagonists OCS Oral corticosteroids SR Sustained release AchB Acetyl choline blockers

52
NEW APPROACHES Omalizumab injection Monoclonal antibody against
Immunoglobin E (anti-IgE) Monoclonal antibody to block the allergic antibody, IgE
 Monoclonal antibody to block the allergic antibody, IgE.")
53
PLEASE REMEMBER If our patient uses reliever medication every day, or even more than three or four times a week, preventer medication must be added to the treatment plan and reliever medication has to be with drawn. GINA Workshop Report, December 2000

54
LET US QUESTION ? Are we giving the right drug ?
Are we giving the drug in right form ? Are we using the correct technique ? ? With all intervention programs, evaluation is necessary to provide answers to two questions. First, “Are we doing the right thing?”---in other words, are we applying approaches that have been demonstrated through scientific research to improve the health of those to whom the intervention is applied? And second, “Are we doing things right?”---in other words, as we apply this proven approach, are we applying it correctly? A well-designed surveillance system coupled with appropriate process measures will provide the answers to these evaluation questions.

55
WHAT HAPPENS WITH WRONG Rx. ?
This diagram first shows you the caliber and appearance of a normal airway. Below it, you can see an inflamed, asthmatic airway. With some treatment, the patient reaches the airway below that, but does not normalize. Most asthma patients in our country shuttle between these 2 types of airways and rarely reverse back to normal for a long time (i.e. sustained control). The consequence of this poor control is a ‘remodeled airway after years of poor control. This airway is like an ‘inflexible’ lead pipe, a so-called fixed obstruction. Such a patient behaves similarly to a patient with COPD, and the prognosis is bad, unlike asthma diagnosed earlier and treated early.
. The consequence of this poor control is a ‘remodeled airway after years of poor control. This airway is like an ‘inflexible’ lead pipe, a so-called fixed obstruction. Such a patient behaves similarly to a patient with COPD, and the prognosis is bad, unlike asthma diagnosed earlier and treated early.")
56
THE STORY OF ASTHMA TREATMENT
This is the story of asthma treatment in India. Patients develop airway inflammation (swelling) and then start shuttling between “part” treatment and “no” treatment. This shuttling occurs in most of our patients in India. It is only with regular inhaled steroid that this airway will return to normal. This should be our objective in asthma management. Remodeled
 and then start shuttling between part treatment and no treatment. This shuttling occurs in most of our patients in India. It is only with regular inhaled steroid that this airway will return to normal. This should be our objective in asthma management. Remodeled.")
57
All Asthma drugs should ideally be taken through the inhaled route.
MOST IMPORTANT All Asthma drugs should ideally be taken through the inhaled route.

58
WHAT CHANGES THEIR LIFE ?
ICS Inhaled corticosteroids ICS are the most potent and effective anti-inflammatory medication currently available for Asthma * *GINA (NHLBI & WHO Workshop Report), December 1995 *Guidelines for the diagnosis and management of Asthma NIH, NHLBI, May 1997
, December *Guidelines for the diagnosis and management of Asthma NIH, NHLBI, May")
59
Corticosteroids ?? Inhaled medicines ??
LET US BELIEVE FIRST Corticosteroids ?? Inhaled medicines ?? Patients’ wrong belief Parents / Grand parents Neighbours / ‘friends’ First of all, let us believe in science Let us explain and convince them Let us change their lives – to happy lives

60
Instead of asthma controlling our patient
REMEMBER Instead of asthma controlling our patient allow our patient to control his / her asthma

61
WHY INHALATION Rx. Oral Inhaled route Slow onset of action
Large dosage used Greater side effects Erratic absorption Not useful in acute illness Inhaled route Rapid onset of action Less amount of drug Drug delivered to the site of mischief Better tolerated Treatment of choice in acute symptoms

62
PREVENTERS Inhaled corticosteroids
Budesonide/ beclomethasone/ fluticasone – use any Start ( mcg/day approx. in 2 divided doses) Maintain for 3 months Taper slowly and keep at 200 mcg Safe for long-term use (years) The safest and most effective preventive medication for asthma are obviously the inhaled corticosteroids. Don’t spend hours trying to decide which one to use. Use any. So long as the inhaler is used correctly and regularly. It is recommended to start with slightly higher doses of about 800 to 1000 mcg per day , maintain that dose for at least 3 months before gradually stepping down the dose to the minimal effective dose. In very mild persistent asthma , you could also start with doses of 400 mcg per day. Inhaled corticosteroids are never to be administered for days or weeks , but months to years.
 Maintain for 3 months. Taper slowly and keep at 200 mcg. Safe for long-term use (years) The safest and most effective preventive medication for asthma are obviously the inhaled corticosteroids. Don’t spend hours trying to decide which one to use. Use any. So long as the inhaler is used correctly and regularly. It is recommended to start with slightly higher doses of about 800 to 1000 mcg per day , maintain that dose for at least 3 months before gradually stepping down the dose to the minimal effective dose. In very mild persistent asthma , you could also start with doses of 400 mcg per day. Inhaled corticosteroids are never to be administered for days or weeks , but months to years.")
63
ICS – HOW SAFE ? They are very safe
Even in small children for several years 30% of Olympic athletes use ICS Not anabolic (performance-enhancing) steroid Even highest ICS dose is safer than low dose oral steroid or beta agonist Best “Addiction” for asthmatics This slide just illustrates a lot of misconceptions about the use of inhaled corticosteroids. Tiny tots can be given these drugs safely for several years. International athletic meets permit the use of these drugs for asthma control. These are not to be confused with Ben Johnson’s ‘steroid !’ That was an anabolic steroid which is classified as a performance-enhancing steroid and therefore banned at athletic meets. People who feel they are addicted to these drugs should realise that there is no better addiction for an asthmatic! In fact it is sad to see so many patients using regular low doses of oral steroid ( for years on end )for asthma control, and who have never used a steroid inhaler in their life; let alone the highest possible dose of inhaled steroid, before becoming dependent on oral steroid.
 steroid. Even highest ICS dose is safer than low dose oral steroid or beta agonist. Best Addiction for asthmatics. This slide just illustrates a lot of misconceptions about the use of inhaled corticosteroids. Tiny tots can be given these drugs safely for several years. International athletic meets permit the use of these drugs for asthma control. These are not to be confused with Ben Johnson’s ‘steroid !’ That was an anabolic steroid which is classified as a performance-enhancing steroid and therefore banned at athletic meets. People who feel they are addicted to these drugs should realise that there is no better addiction for an asthmatic! In fact it is sad to see so many patients using regular low doses of oral steroid ( for years on end )for asthma control, and who have never used a steroid inhaler in their life; let alone the highest possible dose of inhaled steroid, before becoming dependent on oral steroid.")
64
ICS SAFE EVEN FOR A CHILD?
400 mcg/day (budesonide) Over 9 years of continuous use No growth retardation Uncontrolled asthma causes growth retardation Pedersen & Agertoft NEJM 2000 A landmark study done by Agertoft and Pedersen was published 2 years ago which has dispelled most doubts about the safety of inhaled corticosteroids in children. 332 children were recruited in this study with a mean age of 3.4 years in the steroid treated group. The mean Budesonide dose was 412 mcg per day through the study. Although growth rates were significantly reduced during the first years of Budesonide treatment, these changes were not significantly associated with adult height. It was concluded that children who receive budesonide for long-term treatment of their asthma attain normal adult height. It is also clear now that uncontrolled asthma is far more likely to cause growth retardation.
 Over 9 years of continuous use. No growth retardation. Uncontrolled asthma causes growth retardation. Pedersen & Agertoft NEJM A landmark study done by Agertoft and Pedersen was published 2 years ago which has dispelled most doubts about the safety of inhaled corticosteroids in children. 332 children were recruited in this study with a mean age of 3.4 years in the steroid treated group. The mean Budesonide dose was 412 mcg per day through the study. Although growth rates were significantly reduced during the first years of Budesonide treatment, these changes were not significantly associated with adult height. It was concluded that children who receive budesonide for long-term treatment of their asthma attain normal adult height. It is also clear now that uncontrolled asthma is far more likely to cause growth retardation.")
65
PREGNANCY AND ASTHMA Don’t x-ray (if possible)
All asthma medication is safe Even oral corticosteroids are safe for exacerbations Uncontrolled asthma during pregnancy is a serious risk factor for foetal distress and anoxia Thorax Supplement Gynecologists often stop asthma treatment once pregnancy has occurred. This is another misconception that needs to be dispelled. All anti-asthma drugs are safe during pregnancy. As far as possible inhaled medication should be used. However, if a pregnant asthmatic develops an exacerbation, then even oral or parenteral steroids may need to be promptly begun. The risks to the foetus are far higher from uncontrolled asthma during pregnancy than due to any of the anti-asthma drugs. Asthma during pregnancy has an unpredictable course ( some patients actually feel better, some worsen and some remain the same ) and therefore patients should be strongly advised to continue their preventive medication throughout their pregnancy. An excellent position paper in Thorax has outlined guidelines for the management of asthma during pregnancy.
 and therefore patients should be strongly advised to continue their preventive medication throughout their pregnancy. An excellent position paper in Thorax has outlined guidelines for the management of asthma during pregnancy.")
66
Add Leukotriene modifier
ICS not Effective ? Check Inhaler Technique / Check Regular Use Add LABA Formoterol / Salmeterol Add SR Theophylline What if inhaled steroids don’t work ? First check whether the patient is using his inhaler correctly . If he is using it correctly, then check whether he is using it regularly. Most patients who come to Chest Physicians with uncontrolled asthma are either not using any preventive medication or even if they have been prescribed it, are using the inhaler wrongly or irregularly. Only once you are sure that the inhaled steroid is being used correctly and regularly, do you consider the usage of add-on medication. The first choice add-on medication would be long-acting beta2-agonist , followed by a leukotriene modifier and finally sustained-release theophylline. Increasing the dose of inhaled steroid as was formerly recommended , is no longer a preferred option. Increase dose of inhaled steroid Add Leukotriene modifier

67
Step up and down - ACUTE SABA (IBD) in full doses
SABA Increase frequency or Nebulize SABA as above + IPA (IBD), then add OCS (Prednisolone) mg for 3 to 10 days - add ICS (1000 mcg) / day and maintain for 6 weeks minimum Gradually bring down doses and maintain with ICS If symptoms are not relieved – Check the technique and the compliance with Rx. Look for aggravating factors like GE Reflux, Emotions/ stress, Sinusitis Allergic Rhinitis, Persistent allergens No role for Theophylline; Oral SABA or LABA not very useful We should realise now that though these are new, oral anti-inflammatory drugs for asthma, they are nowhere near the potency of inhaled corticosteroids. Being oral, these drugs have become convenient for doctors and patients alike. Probably, one of the few indications to use these drugs first-line has been asthma in 2 to 5 years old children where one 4 mg chewable tablet needs to be given daily. In this age group it is impossible to objectively confirm a diagnosis of asthma and preventer treatment is usually based on clinical grounds. In the event of strong reluctance from parents to use inhaled steroids, a trial of montelukast may be worthwhile. Also, all patients feeling well or partly well with ‘regular’ bronchodilators are also candidates for Montelukast, since there will be at least some anti-inflammatory activity. However, this activity if far less than that of inhaled steroids.
, then add. OCS (Prednisolone) mg for 3 to 10 days - add. ICS (1000 mcg) / day and maintain for 6 weeks minimum. Gradually bring down doses and maintain with ICS. If symptoms are not relieved – Check the technique and the compliance with Rx. Look for aggravating factors like. GE Reflux, Emotions/ stress, Sinusitis. Allergic Rhinitis, Persistent allergens. No role for Theophylline; Oral SABA or LABA not very useful. We should realise now that though these are new, oral anti-inflammatory drugs for asthma, they are nowhere near the potency of inhaled corticosteroids. Being oral, these drugs have become convenient for doctors and patients alike. Probably, one of the few indications to use these drugs first-line has been asthma in 2 to 5 years old children where one 4 mg chewable tablet needs to be given daily. In this age group it is impossible to objectively confirm a diagnosis of asthma and preventer treatment is usually based on clinical grounds. In the event of strong reluctance from parents to use inhaled steroids, a trial of montelukast may be worthwhile. Also, all patients feeling well or partly well with ‘regular’ bronchodilators are also candidates for Montelukast, since there will be at least some anti-inflammatory activity. However, this activity if far less than that of inhaled steroids.")
68
The Step Care Approach - Prevent
ICS ICS + LABA (IBD) ICS + LABA (IBD) + Double Dose ICS ICS (DD) + LABA + LTA (oral) ICS (DD) + LABA + LTA + OCS ICS (DD) + LABA + LTA + OCS + TIO (IBD) SR Theophylline may be add on SABA or LABA Oral + IPA (IBD) may be useful add on No long acting steroid injections No injectable or short acting Theophylline We should realise now that though these are new, oral anti-inflammatory drugs for asthma, they are nowhere near the potency of inhaled corticosteroids. Being oral, these drugs have become convenient for doctors and patients alike. Probably, one of the few indications to use these drugs first-line has been asthma in 2 to 5 years old children where one 4 mg chewable tablet needs to be given daily. In this age group it is impossible to objectively confirm a diagnosis of asthma and preventer treatment is usually based on clinical grounds. In the event of strong reluctance from parents to use inhaled steroids, a trial of montelukast may be worthwhile. Also, all patients feeling well or partly well with ‘regular’ bronchodilators are also candidates for Montelukast, since there will be at least some anti-inflammatory activity. However, this activity if far less than that of inhaled steroids.
 ICS + LABA (IBD) + Double Dose ICS. ICS (DD) + LABA + LTA (oral) ICS (DD) + LABA + LTA + OCS. ICS (DD) + LABA + LTA + OCS + TIO (IBD) SR Theophylline may be add on. SABA or LABA Oral + IPA (IBD) may be useful add on. No long acting steroid injections. No injectable or short acting Theophylline. We should realise now that though these are new, oral anti-inflammatory drugs for asthma, they are nowhere near the potency of inhaled corticosteroids. Being oral, these drugs have become convenient for doctors and patients alike. Probably, one of the few indications to use these drugs first-line has been asthma in 2 to 5 years old children where one 4 mg chewable tablet needs to be given daily. In this age group it is impossible to objectively confirm a diagnosis of asthma and preventer treatment is usually based on clinical grounds. In the event of strong reluctance from parents to use inhaled steroids, a trial of montelukast may be worthwhile. Also, all patients feeling well or partly well with ‘regular’ bronchodilators are also candidates for Montelukast, since there will be at least some anti-inflammatory activity. However, this activity if far less than that of inhaled steroids.")
69
Leukotriene Modifiers
Oral leukotrine antagonist – anti inflammatory Not as effective as inhaled steroid May be first-line for 2 to 5 yr. olds. Montelukast available; Zafirlukast is not in India 4 mg, 5 mg, 8 mg tabs available Can be add on to ICS, IBD inhalers We should realise now that though these are new, oral anti-inflammatory drugs for asthma, they are nowhere near the potency of inhaled corticosteroids. Being oral, these drugs have become convenient for doctors and patients alike. Probably, one of the few indications to use these drugs first-line has been asthma in 2 to 5 years old children where one 4 mg chewable tablet needs to be given daily. In this age group it is impossible to objectively confirm a diagnosis of asthma and preventer treatment is usually based on clinical grounds. In the event of strong reluctance from parents to use inhaled steroids, a trial of montelukast may be worthwhile. Also, all patients feeling well or partly well with ‘regular’ bronchodilators are also candidates for Montelukast, since there will be at least some anti-inflammatory activity. However, this activity if far less than that of inhaled steroids.

70
NOT ALL ARE SAME !! Beclomethasone 6 hrly + Salbutamol 6th hrly
Budesonide 12 hrly + Salmeterol 12 hrly Salmeterol 12 hrly + Ipatropium 12 hrly Fluticasone 24 hrly + Formoterol 24 hrly Formoterol 24 hrly + Tiotropium 24 hrly Choice is based on If need is urgent and uncontrolled – 6 hrly If need is maintenance, well contr. – 12 hrly If stabilized and wants convenience – 24 hrly We should realise now that though these are new, oral anti-inflammatory drugs for asthma, they are nowhere near the potency of inhaled corticosteroids. Being oral, these drugs have become convenient for doctors and patients alike. Probably, one of the few indications to use these drugs first-line has been asthma in 2 to 5 years old children where one 4 mg chewable tablet needs to be given daily. In this age group it is impossible to objectively confirm a diagnosis of asthma and preventer treatment is usually based on clinical grounds. In the event of strong reluctance from parents to use inhaled steroids, a trial of montelukast may be worthwhile. Also, all patients feeling well or partly well with ‘regular’ bronchodilators are also candidates for Montelukast, since there will be at least some anti-inflammatory activity. However, this activity if far less than that of inhaled steroids.

71
Formoterol + Budesonide combination - the Flexible Preventer
Quickly gains control Asthma worsening This illustrates beautifully the flexible nature of Formoterol- Budesonide combination in asthma practice. Starting off with 2 Rotacaps twice daily, patients gradually get better, and after 2 months the dose can be stepped down to 1 Rotacap twice daily. During exacerbations of asthma, the dose may have to be increased again to 2 Rotacaps twice daily for a a few months and can be again reduce once control is achieved for a couple of months at least. For patients who are controlled on 1 Rotacap twice daily for prolonged periods of time, one could even consider tapering further to a dose of just 1 Rotacap once daily. This is extremely convenient to your patients, you can imagine. Almost like taking a one-a-day tablet for hypertension control! Reduce to lowest adequate dose that maintains control Asthma signs Maintains control Maintains control 2x2 2x2 1x1 1x2 1x2 Time

72
Why doctors don’t use inhalation therapy
Status quo : “my practice is good or ‘great’” Oral therapy is easy Too busy Difficulty in convincing Cost Headache to explain Many doctors feel that if they are busy in practice, they don’t need to really update themselves on newer advances in management. This is extremely true for asthma. Patients more and more, want precise information from their doctor about their disease, it’s prognosis and the best available treatment. Doctors who tend to ignore new developments in treatment often get left behind when it comes to managing difficult patients. In fact, being very busy in practice can often be a disadvantage when it comes to the time you can spend with the patient. More and more patients are complaining that their doctors don’t give them enough time. This is dangerous because poor communication between the patient and doctor is one of the commonest reasons of consumer court cases against doctors. Doctors cannot any longer opt for second best options for lack of time because more and more patients expect the best treatment from their doctor. Cost of inhalation therapy is also becoming less and less of an issue when patients realise the huge amounts of money they have to pay when they get hospitalised for asthma. Therefore, patients will soon no longer tolerate excuses from doctors on why they never received any inhalation therapy.

73
DRUG DELIVERY OPTIONS Metered dose inhalers (MDI)
Dry powder inhalers (Rotahaler) Spacers / Holding chambers Nebulizers
 Spacers / Holding chambers. Nebulizers.")
74
Demonstration of the correct technique
Ask the patient to demonstrate to you the technique

75
DRUG DELIVERY - OPTIONS
Dexterity Hand grip strength Co-ordination Severity of COPD Educational level Age of the patient Ability to inhale and synchronize pMDI – Metered Dose Inhalers Rotahalers, Diskhalers Spacehalers Nebulizers Oxygen mixed delivery Oral tablets, syrups Parenteral – I.M or I.V use

76
WHAT DRUG DELIVERY METHOD ?
Very young or very old MDI + LV Spacer Elderly MDI + SV spacer Young children > 7 yrs DPI (Rotahaler) Adults edu. understood MDI alone Adults no co-ordination DPI (Rotahalers) Clinic setting MDI + Spacer Clinic - emergency Nebulizer Choice is to be individualized Trial and error may be needed Cost may be a factor We should realise now that though these are new, oral anti-inflammatory drugs for asthma, they are nowhere near the potency of inhaled corticosteroids. Being oral, these drugs have become convenient for doctors and patients alike. Probably, one of the few indications to use these drugs first-line has been asthma in 2 to 5 years old children where one 4 mg chewable tablet needs to be given daily. In this age group it is impossible to objectively confirm a diagnosis of asthma and preventer treatment is usually based on clinical grounds. In the event of strong reluctance from parents to use inhaled steroids, a trial of montelukast may be worthwhile. Also, all patients feeling well or partly well with ‘regular’ bronchodilators are also candidates for Montelukast, since there will be at least some anti-inflammatory activity. However, this activity if far less than that of inhaled steroids.
 Adults edu. understood MDI alone. Adults no co-ordination DPI (Rotahalers) Clinic setting MDI + Spacer. Clinic - emergency Nebulizer. Choice is to be individualized. Trial and error may be needed. Cost may be a factor. We should realise now that though these are new, oral anti-inflammatory drugs for asthma, they are nowhere near the potency of inhaled corticosteroids. Being oral, these drugs have become convenient for doctors and patients alike. Probably, one of the few indications to use these drugs first-line has been asthma in 2 to 5 years old children where one 4 mg chewable tablet needs to be given daily. In this age group it is impossible to objectively confirm a diagnosis of asthma and preventer treatment is usually based on clinical grounds. In the event of strong reluctance from parents to use inhaled steroids, a trial of montelukast may be worthwhile. Also, all patients feeling well or partly well with ‘regular’ bronchodilators are also candidates for Montelukast, since there will be at least some anti-inflammatory activity. However, this activity if far less than that of inhaled steroids.")
77
DRUG DELIVERY - OPTIONS

78
INHALATION DEVICES Rotahaler Dry powder Inhaler Metered dose
inhaler or MDI Spacer Spacehaler

79
MDI + LARGE VOLUME SPACER
As you can see here how easy it is to use an MDI + spacer with a baby mask for a small child. Just apply the mask snugly over the child’s nose and mouth and then press down on the inhaler. Keep the mask tightly attached to the child’s face for at least 30 seconds for one dose. Remember even if the child cries, the child is breathing and therefore, receives the dose adequately.

80
ROTAHALER – DRY POWDER Overcomes hand-lung coordination
problems encountered with MDIs. Can be easily used by children, elderly and arthritic patients. Can take multiple inhalations if the entire drug has not been inhaled in one inhalation.

81
THE ZEROSTAT ADVANTAGE
Non - static spacer made up of polyamide material Increased respirable fraction ® Increased deposition of drug in the airways Increased aerosol half - life ® Plenty of time for the patient to inhale after actuation of the drug No valve ® No dead space ® Less wastage of the drug Small, portable, easy to carry ® Child friendly

82
DISKHALER – NEBULISER

83
NEBULISED THERAPY Severe breathlessness despite using inhalers
Assessment should be done for improvement Choice between a facemask or mouth piece Equipment servicing and support are essential Dosage 0.5 ml of Ipatropium + 0.5 ml of Salbutamol + 5 ml of NaCl (not DW) If decided to use ICS (FEV1 < 50%) – 0.5 ml of Budusonide is added to the above 15 minutes and slow or moderate flow rate Can be repeated 2 to 3 times a day – Mouth Wash
 If decided to use ICS (FEV1 < 50%) – 0.5 ml of Budusonide is added to the above. 15 minutes and slow or moderate flow rate. Can be repeated 2 to 3 times a day – Mouth Wash.")
84
PATIENT EDUCATION Explain nature of the disease (inflammation)
Explain action of prescribed drugs Stress the need for regular, long-term therapy That way only we can convince Allay fears and concerns Peak flow testing Symptom, treatment diary

85
PATIENT EDUCATION Asthma is a common disorder
It can happen to anybody, May not be life long It is not caused by supernatural forces Asthma is not contagious, All kin needn’t be affected Recurrent attacks of cough with or without wheeze Between attacks people with asthma lead normal lives as anyone else In most cases, there is some family history of allergy

86
PATIENT EDUCATION Asthma can be effectively controlled, although it cannot be cured. Effective asthma management programs include education, objective measures of lung function, environmental control, and pharmacologic therapy. A stepwise approach to pharmacologic therapy is recommended. The aim is to accomplish the goals of therapy with the least possible medication.

87
YOURS FAITHFULLY REQUESTS
A little time spent talking to our patients - really is a great investment. This may make all the difference between a happy life and pulmonary invalidity

88
Can We dare to make them pulmonary invalids ?
LET US GIVE THEM Can We dare to make them pulmonary invalids ? LIFE TIME HAPPINESS

Similar presentations

>")
 Airway.>")




 -based on the recognition of a characteristic pattern of symptoms and signs and the absence of an alternative.>")


 By Chris Callan 23 April 2008.>")




 Diagnosis and management of chronic asthma in line with current BTS guidelines (Dr Lowery) 3 x Case.>")



