Download presentation
Presentation is loading. Please wait.

1
PHYSIOLOGY OF THE THYROID GLAND
Dr. Amel Eassawi

2
OBJECTIVES The student should be able to:
Describe the distribution of iodine in the body, dietary requirements for iodine and thyroid uptake of iodine. Identify the structure and formula for thyroxine (T4) and triiodothyronine (T3). Know the basic steps involved in the biosynthesis of T3 and T4. Identify the bound forms and quantities of T3 and T4 in circulation. Relate the plasma half-life of thyroid hormones to their biological effects. Describe the effects of TSH on thyroid activity. Describe the relationship of TSH, and TRH to T4 secretion. Know the physiological effects of thyroid hormone. Indicate the relative activities of T4 and T3. Describe the etiology, symptoms and treatment of thyrotoxicosis and hypothyroidism.
 and triiodothyronine (T3). Know the basic steps involved in the biosynthesis of T3 and T4. Identify the bound forms and quantities of T3 and T4 in circulation. Relate the plasma half-life of thyroid hormones to their biological effects. Describe the effects of TSH on thyroid activity. Describe the relationship of TSH, and TRH to T4 secretion. Know the physiological effects of thyroid hormone. Indicate the relative activities of T4 and T3. Describe the etiology, symptoms and treatment of thyrotoxicosis and hypothyroidism.")
3
Thyroid Gland The largest endocrine gland, located in the anterior neck. Consists of two lateral lobes connected by a median tissue mass called the isthmus

4
Thyroid Gland The largest endocrine gland, located in the anterior neck Located just below the larynx Consists of two lobes of endocrine tissue joined in middle by narrow portion of gland Consists of microscopic sacs known as thyroid follicles Interior filled with colloid, a protein-rich fluid (thyroglobulin) Between thyroid follicles are epithelial cells known as parafollicular cells (C-cells) produce hormone called calcitonin.
 Between thyroid follicles are epithelial cells known as parafollicular cells (C-cells) produce hormone called calcitonin.")
6
Thyroid Gland Histology
The thyroid gland consists of groups of thyroid follicles surrounded by connective tissue capsules Thyroid follicles are composed of a space, filled with the glycoprotein colloid, enclosed by a layer of follicular cells

7
THYROID GLAND FETAL DEVELOPMENT
Follicle cells able to synthesize thyroglobulin – 29th day of gestation Ability to concentrate iodide and synthesize T4 – 11th week Follicles fill with colloid – weeks Thyroid gland functional – 3rd month of fetal life

8
THYROID HORMONES Thyroid hormone – the body’s major metabolic hormone
Consists of two closely related iodine-containing compounds T4 – thyroxine T3 – triiodothyronine The parafollicular cells or “C” cells produce the hormone calcitonin. Calcitonin is a peptide hormone lowers blood calcium levels in children. Antagonistic to parathyroid hormone (PTH). Calcitonin targets the skeleton, where it: 1. Inhibits osteoclast activity (and thus bone resorption) and release of calcium from the bone matrix 2. Stimulates calcium uptake and incorporation into the bone matrix. Regulated by calcium ion concentration in the blood (negative feedback mechanism).
. Calcitonin targets the skeleton, where it: 1. Inhibits osteoclast activity (and thus bone resorption) and release of calcium from the bone matrix. 2. Stimulates calcium uptake and incorporation into the bone matrix. Regulated by calcium ion concentration in the blood (negative feedback mechanism).")
9
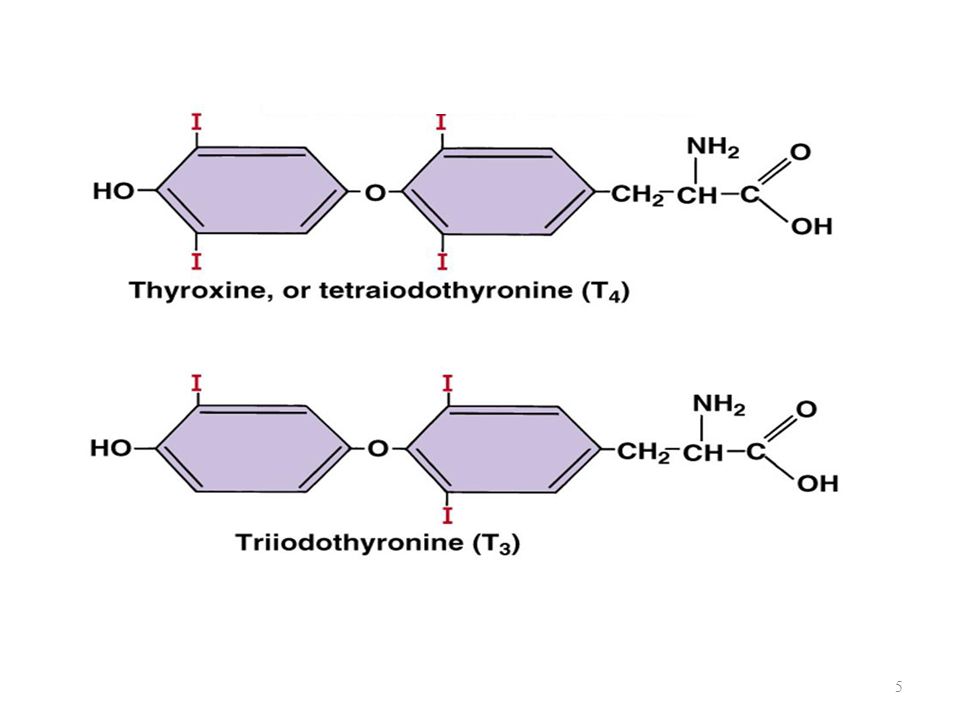
THYROID HORMONES The three thyroid hormones are:
1. Thyroxine (3,5,3’,5’- tetraiodothyronine) or T4: Principal hormone secreted by the thyroid follicle cells. Normal plasma levels of T4 range from 4.5 – 9.5 µg/mL. T4 has a circulating half-life of 7 days. 2. Triiodothyronine (3,5,3’ – triiodothyronine) or T3: Normal plasma concentrations of T3 range from ng/100mL. Most (2/3) of T3 is derived from peripheral deiodination of T4 by the kidney and liver. T3 has a ½ life of about 1 day and it is at least 3 times more potent than T4 on an equal molar basis. 3. Reverse T3 (3,3’,5’ – triiodothyronine) or rT3: Biologically inactive thyroidal product which circulates in the plasma at a concentration of about 48 ng/100mL. Most of rT3 is derived from peripheral conversion of T4.
 or T4: Principal hormone secreted by the thyroid follicle cells. Normal plasma levels of T4 range from 4.5 – 9.5 µg/mL. T4 has a circulating half-life of 7 days. 2. Triiodothyronine (3,5,3’ – triiodothyronine) or T3: Normal plasma concentrations of T3 range from ng/100mL. Most (2/3) of T3 is derived from peripheral deiodination of T4 by the kidney and liver. T3 has a ½ life of about 1 day and it is at least 3 times more potent than T4 on an equal molar basis. 3. Reverse T3 (3,3’,5’ – triiodothyronine) or rT3: Biologically inactive thyroidal product which circulates in the plasma at a concentration of about 48 ng/100mL. Most of rT3 is derived from peripheral conversion of T4.")
10
THYROID HORMONE SYNTHESIS
Basic ingredients: Tyrosine Synthesized in sufficient amounts by body Iodine Obtained from dietary intake Dietary Iodine Requirements: Approximately 100 µg/day of iodine are essential for the synthesis of normal amounts of thyroid hormones. The major source of iodide comes from the diet.

11
THYROID HORMONE SYNTHESIS
Steps in hormone synthesis and secretion: Iodide Trapping Organification Reaction Coupling Reaction Hormone Release Iodide Trapping: Transport of iodide is dependent on sodium gradient across basal membrane of follicle cell Sodium-iodide symporter (NIS) transports iodide atom against an electrochemical gradient.
 transports iodide atom against an electrochemical gradient.")
12
THYROID HORMONE SYNTHESIS
Organification Reaction: Activated iodine incorporated into tyrosine residue of thyroglobulin Coupling Reaction: Iodinated tyrosine linked to form T4 and T3 Peripheral Deiodination: Type I and 2 deiodination Organ specific Inactivation of T4 and T3 (D3)
")
13
TYHYROID HORMONES STORAGE AND SECREATION
Thyroglobulin and its attached residues of MIT, DIT, T3, and T4 are stored in the colloid until secreted. The thyroid gland has a large reservoir of hormone. In normal humans, about 250 µg of T4 per gram of wet weight can be stored in the gland. Inhibition of hormone synthesis by antithyroidal substances for as long as 2-weeks does not significantly reduce hormone levels in the blood. Secretion: Secretion of thyroid hormone involves endocytosis, specifically macropinocytosis and micropinocytosis of the colloid by the follicle cells and subsequent formation of vesicles containing the thyroglobulin molecule and its residues. The vesicles merge with lysosomes containing active proteases which hydrolyze the thyroglobulin molecule and release MIT, DIT, T4 and T3 into the cytoplasm. Subsequently, T4 and T3 diffuse into the plasma.

14
TYHYROID HORMONES STORAGE AND SECREATION
Deiodination: MIT and DIT are deiodinated in the cytoplasm by a microsomal NADPH-dependent deiodinase. The liberated iodide is either immediately used for the synthesis of new hormones in the colloid or lost into the circulation as an “iodide leak”. Deiodination of T4 to T3 occurs by thyroidal type 1 and 2 deiodinases. Excessive Thyroidal Iodide: Organification of iodine decreases in response to increasing thyroidal iodide. This phenomenon is called the “Wolff-Chaikoff effect”. As iodide levels remain high, the gland adapts and begins to make normal amounts of thyroid hormone.

15
Synthesis of Thyroid Hormone

16
Synthesis, Storage and Secretion of Thyroid Hormones

18
Pathway of Thyroid Hormone Synthesis

19
THYROID HORMONES TRANSPORT
T4 and T3 poorly soluble in water. Transported in plasma by binding proteins: 1. Thyroxine-binding globulin (TBG) 2. Transthyretin (TTR) Albumin 70-80% of T3 bound to (TBGs)
 2. Transthyretin (TTR) Albumin % of T3 bound to (TBGs)")
20
THYROID HORMONE REGULATION
Hypothalamic-Pituitary-Thyroid Axis Thyroid Gland Autoregulation Peripheral Regulation

22
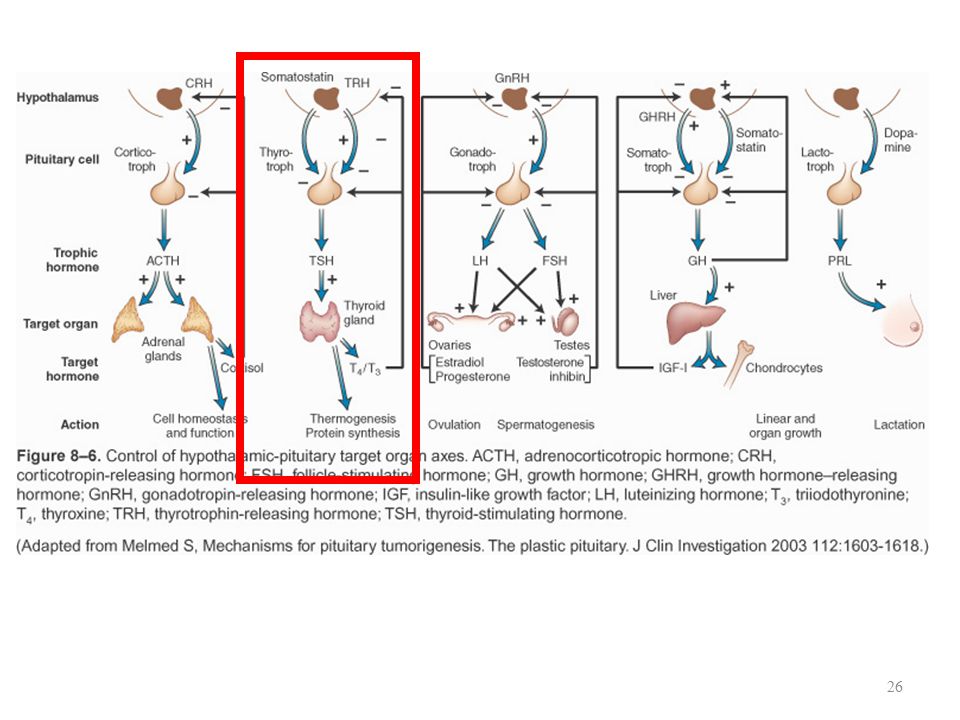
THYROID HORMONE REGULATION
Hypothalamic-Pituitary-Thyroid Axis Thyrotropin-releasing hormone (TRH) Tripeptide Released from hypothalamus/episodic secretory pattern Stimulates thyrotroph cells Thyroid-stimulating hormone (TSH) Glycoprotein secreted by thyrotrophs Regulates thyroid gland growth, secretion, and metabolism Thyrotrophs stimulated by TRH Present in fetal plasma – (18-26 weeks of gestation)
 Tripeptide. Released from hypothalamus/episodic secretory pattern. Stimulates thyrotroph cells. Thyroid-stimulating hormone (TSH) Glycoprotein secreted by thyrotrophs. Regulates thyroid gland growth, secretion, and metabolism. Thyrotrophs stimulated by TRH. Present in fetal plasma – (18-26 weeks of gestation)")
23
Thyroid Cell Functions Stimulated by TSH

24
THYROID HORMONE REGULATION
Thyroid-stimulating hormone (TSH) stimulates: Trapping mechanism Organification and coupling reactions Increase in follicle cell size Enlargement of Golgi apparatus
 stimulates: Trapping mechanism. Organification and coupling reactions. Increase in follicle cell size. Enlargement of Golgi apparatus.")
25
Hypothalamic-Pituitary-Thyroid Axis
Negative feedback regulation Anterior pituitary: primary feedback effect Free fraction of T4 and T3 participate T4 and T3 inhibit TRH and TSH

28
Regulation by Energy Intake/Adipose Stores

29
Environmental Regulation of Thyroid Hormone Secretion

30
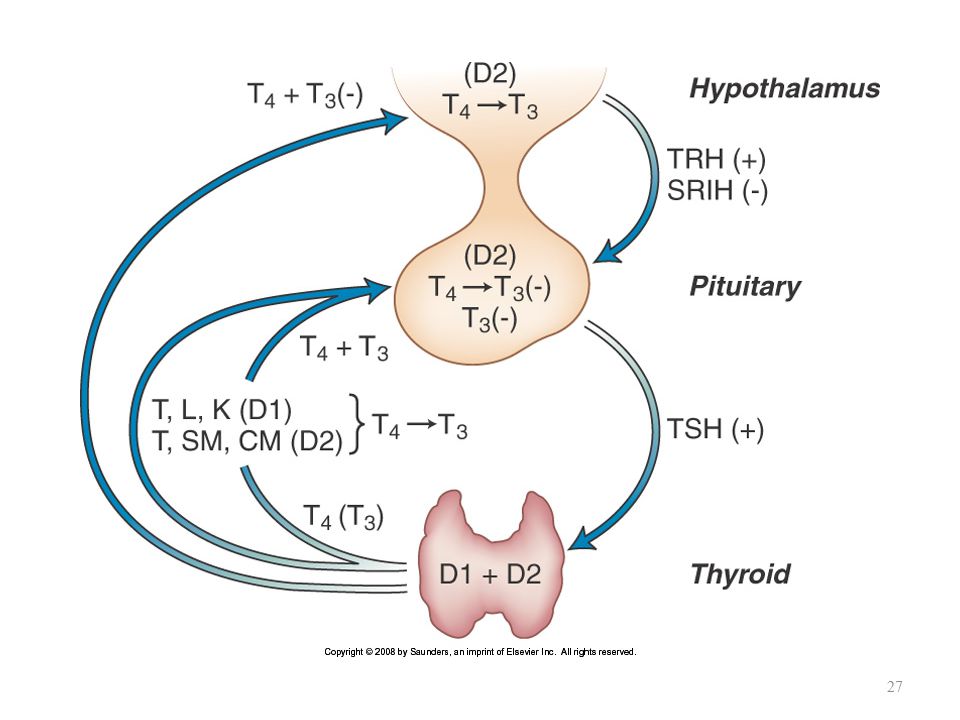
THYROID GLAND AUTOREGULATION
Thyroid Gland Autoregulation: Thyroid gland function is controlled by an autoregulation mechanism that maintains adequate thyroidal stores of T4 and T3 when plasma iodide levels vary outside normal limits. Peripheral Regulation of Thyroid Hormone Increases in thyroid hormone results in increased formation of the biologically inactive thyroidal product rT3.

31
Effects of Thyroid Hormone
Thyroid hormones bind to nuclear thyroid hormone receptor T3 is ten times more potent than T4

32
Thyroid hormone Effects
All body cells affected either directly or indirectly by thyroid hormone: 1. Main determinant of basal metabolic rate (BMR). BMR regulator of body's rate of O2 consumption & energy expenditure under resting conditions. 2. Influences synthesis and degradation of carbohydrate, fat, and protein. 3. Increases target-cell responsiveness to catecholamines by causing a proliferation of specific catecholamine target-cell receptors 4. Increases heart rate and force of contraction. 5. Essential for normal growth. Stimulates GH secretion and increases production of IGF-I by liver. Promotes effects of GH & IGF-I on synthesis of new structural proteins on skeletal growth. 6. Plays crucial role in normal development of nervous system.
. BMR regulator of body s rate of O2 consumption & energy expenditure under resting conditions. 2. Influences synthesis and degradation of carbohydrate, fat, and protein. 3. Increases target-cell responsiveness to catecholamines by causing a proliferation of specific catecholamine target-cell receptors. 4. Increases heart rate and force of contraction. 5. Essential for normal growth. Stimulates GH secretion and increases production of IGF-I by liver. Promotes effects of GH & IGF-I on synthesis of new structural proteins on skeletal growth. 6. Plays crucial role in normal development of nervous system.")
33
Thyroid Regulation of Cardiovascular Function

34
THYROID HORMONES ABNORMALITIES
Goiter - enlargement of the thyroid gland, causing a swelling in the front part of the neck. Hyperthyroidism Hypothyroidism

35
THYROID HORMONES ABNORMALITIES
Hypothyroidism –Primary: failure of thyroid gland (↓T3 & T4; ↑TSH); Goiter –Secondary: deficiency of TRH, TSH, or both (↓T3 & T4; ↓TSH and/or ↓ TRH); no Goiter (because thyroid gland is not being adequately stimulated) –Inadequate dietary supply of iodine (↓T3 & T4; ↑TSH), Goiter Symptoms of hypothyroidism: 1. Reduced BMR. 2. Poor tolerance to cold (lack of the calorigenic effect) 3. Gain excessive weight. 4. Easily fatigued (lower energy production) 5. Slow, weak pulse (caused by a reduction in the rate and strength of cardiac contraction and lowered cardiac output) 6. Exhibits slow reflexes and slow mental responsiveness (because of the effect on the nervous system; characterized by slow speech, and poor memory).
; Goiter. –Secondary: deficiency of TRH, TSH, or both (↓T3 & T4; ↓TSH and/or ↓ TRH); no Goiter (because thyroid gland is not being adequately stimulated) –Inadequate dietary supply of iodine (↓T3 & T4; ↑TSH), Goiter. Symptoms of hypothyroidism: 1. Reduced BMR. 2. Poor tolerance to cold (lack of the calorigenic effect) 3. Gain excessive weight. 4. Easily fatigued (lower energy production) 5. Slow, weak pulse (caused by a reduction in the rate and strength of cardiac contraction and lowered cardiac output) 6. Exhibits slow reflexes and slow mental responsiveness (because of the effect on the nervous system; characterized by slow speech, and poor memory).")
36
Thyroid Gland Abnormalities
Hypothyroidism Cretinism (Children): – Results from hypothyroidism from birth – Characterized by dwarfism & mental retardation as well as other general symptoms of thyroid deficiency. – At birth, child appears normal because thyroxine is received from mother through placenta – Symptoms: stop growth, abnormal bone development, low body temperature, lethargy, severly mentally retarded (short limbs, a large protruding tongue, coars dry skin, poor abdominal muscle, tone and an umbilical hernia).
: – Results from hypothyroidism from birth. – Characterized by dwarfism & mental retardation as well as other general symptoms of thyroid deficiency. – At birth, child appears normal because thyroxine is received from mother through placenta. – Symptoms: stop growth, abnormal bone development, low body temperature, lethargy, severly mentally retarded (short limbs, a large protruding tongue, coars dry skin, poor abdominal muscle, tone and an umbilical hernia).")
38
Thyroid Gland Abnormalities
Myxedema (Adult) Puffy appearance, primarily of face, hands, and feet –Term often used for myxedema in adults Symptoms: The patient becomes sluggish both mentally and physically and often feels cold. The hair becomes dry and the skin becomes dry and waxy. The tissues of the face swell. Treatment: – If diagnosed early, can be treated by administrating of T4. – Exception, if hypothyroidism caused by iodine deficiency; treated by dietary iodine.
 Puffy appearance, primarily of face, hands, and feet. –Term often used for myxedema in adults. Symptoms: The patient becomes sluggish both mentally and physically and often feels cold. The hair becomes dry and the skin becomes dry and waxy. The tissues of the face swell. Treatment: – If diagnosed early, can be treated by administrating of T4. – Exception, if hypothyroidism caused by iodine deficiency; treated by dietary iodine.")
39
MYXEDEMA Copyright © 2007 Elsevier Inc

40
Thyroid Gland Abnormalities
THYROTOXICOSIS: Excessive quantities of thyroid hormone. Causes: hyperthyroidism, thyroiditis, and excessive exogenous thyroid hormone.

41
Thyroid Gland Abnormalities
Hyperthyroidism Causes: Secondary: 1. Over secreation of hypothalamic or pituitary secretion (↑T3 and T4; ↑TRH and/or ↑TSH) Goiter 2. Over activity of thyroid in absence of overstimulation, e.g thyroid tumor, that not accompanied by a goiter. (though a goiter does not develop, a tumor may cause enlargement of thyroid, depending on nature or size of tumor) •Secretion of excessive amounts of T3 and T4 inhibits TSH, so there is no growth of the thyroid.
 Goiter. 2. Over activity of thyroid in absence of overstimulation, e.g thyroid tumor, that not accompanied by a goiter. (though a goiter does not develop, a tumor may cause enlargement of thyroid, depending on nature or size of tumor) •Secretion of excessive amounts of T3 and T4 inhibits TSH, so there is no growth of the thyroid.")
42
Thyroid Gland Abnormalities
Symptoms of hyperthyroidism: 1. Increased BMR. 2. Poor tolerance to hot 3. Excessive weight loss. 4. Easily fatigued (lower energy production) 5. Palpitations. 6. Excessive mental alertness, irritable, tense, anxious and excessively emotional.
 5. Palpitations. 6. Excessive mental alertness, irritable, tense, anxious and excessively emotional.")
43
Thyroid Gland Abnormalities
Hyperthyroidism – Graves’ disease – Autoimmune disease – Body mistakenly produces thyroid-stimulating immunoglobulins (TSI) also known as long-acting thyroid stimulator (LATS), – Antibodies act like TSH & stimulate thyroid gland to grow and over secrete thyroid hormones.
 also known as long-acting thyroid stimulator (LATS), – Antibodies act like TSH & stimulate thyroid gland to grow and over secrete thyroid hormones.")
44
Thyroid Gland Abnormalities
Graves Disease Risk factors include stress, increased iodine intake, smoking and unidentified environmental factors Exothalamus is associated in 50% of cases

45
(↑T3 & T4; ↓ TSH) Goiter
 Goiter")
47
(A) Characteristic signs of Graves' orbitopathy (A) subsequently corrected by orbital decompression surgery (B). Note the thyroid stare, the asymmetry, the proptosis, and the periorbital edema before correction Copyright © 2007 Elsevier Inc

48
Induction of Goiter by Hypo- and Hyperthyroid States

49
TREATMENT METHODOLOGIES
Treatment Goals for Hyperthyroidism: Inhibit or decrease synthesis and secretion of thyroid hormone Limit symptoms of hyperthyroidism Surgical removal of a portion of the over-secreting thyroid Administration of radioactive iodine Use of antithyroid drugs Treatment Goal for Hypothyroidism: Return of serum TSH levels to normal Synthetic thyroxine - levothyroxine

50
References Human physiology, Lauralee Sherwood, seventh edition.
Text book physiology by Guyton &Hall,11th edition. Physiology by Berne and Levy, sixth edition.

Similar presentations







 pages pp. 43-50 before Metabolism of thyroid hormones section; (2) pages 56 (Regulation.>")


 Triiodothyronine (T3) T4 and T3 regulate body metabolism.>")







. Its size depends on: 1. age … age size. 2. sex … female > male. 3.>")


. It has two lobes that are joined together.>")

