Download presentation
Presentation is loading. Please wait.

2
Presented by: Carolyn Brown, M.Ed, RN, ARM, FCCWS National Director of Clinical Services C-3 Management of the Obese Population A Person Centered Care Approach

3
After attending this program the participant will be able to: 1.Define obesity and calculate Body Mass Index (BMI). 2.Discuss prevalence of obesity. 3.Identify unique and predictable clinical issues resulting from obesity and discuss assessment techniques for each. 4.Identify community resources to support bariatric care. 5.Review case study and identify appropriate supply and equipment needs. Learner Objectives

4
A life-long, progressive, life threatening, costly, genetically-related, multi-factorial disease of excess fat storage. Resource: American Society of Bariatric Surgery Obesity Bariatric (Greek) The practice of health care related to the treatment of obesity and associated conditions.
 The practice of health care related to the treatment of obesity and associated conditions..")
5
Obese Body Mass Index (BMI) of 30 or greater Morbid Obesity 100 lbs. greater than ideal body weight BMI of 40 or greater BMI of 35 with 2 or more co-morbidities Resource: American Society of Bariatric Surgery Who Is Obese

6
Body Mass Index (BMI)
")
8
Central Obesity Waist circumference is now considered a useful tool in predicting high risk, high cost comorbidities such as diabetes, high cholesterol, hypertension and coronary artery disease. Central Obesity identifies a risk category above that defined by BMI and may allow the clinical team to better predict cost of care and length of stay. Would waist circumference support the customer’s decision to rent or purchase!!! Men> 40 inches Women> 35 inches

9
Obesity Trends* Among U.S. Adults BRFSS, 1985 (*BMI 30, or ~ 30 lbs overweight for 5’4” woman) No Data <10% 10%-14% 15-19% 20-24% 25%
 No Data <10% 10%-14% 15-19% 20-24% 25%.")
10
Obesity Trends* Among U.S. Adults BRFSS, 1986 (*BMI 30, or ~ 30 lbs overweight for 5’4” woman) No Data <10% 10%-14% 15-19% 20-24% 25%
 No Data <10% 10%-14% 15-19% 20-24% 25%.")
11
Obesity Trends* Among U.S. Adults BRFSS, 1987 (*BMI 30, or ~ 30 lbs overweight for 5’4” woman) No Data <10% 10%-14% 15-19% 20-24% 25%
 No Data <10% 10%-14% 15-19% 20-24% 25%.")
12
Obesity Trends* Among U.S. Adults BRFSS, 1988 (*BMI 30, or ~ 30 lbs overweight for 5’4” woman) No Data <10% 10%-14% 15-19% 20-24% 25%
 No Data <10% 10%-14% 15-19% 20-24% 25%.")
13
Obesity Trends* Among U.S. Adults BRFSS, 1989 (*BMI 30, or ~ 30 lbs overweight for 5’4” woman) No Data <10% 10%-14% 15-19% 20-24% 25%
 No Data <10% 10%-14% 15-19% 20-24% 25%.")
14
Obesity Trends* Among U.S. Adults BRFSS, 1990 (*BMI 30, or ~ 30 lbs overweight for 5’4” woman) No Data <10% 10%-14% 15-19% 20-24% 25%
 No Data <10% 10%-14% 15-19% 20-24% 25%.")
15
Obesity Trends* Among U.S. Adults BRFSS, 1991 (*BMI 30, or ~ 30 lbs overweight for 5’4” woman) No Data <10% 10%-14% 15-19% 20-24% 25%
 No Data <10% 10%-14% 15-19% 20-24% 25%.")
16
Obesity Trends* Among U.S. Adults BRFSS, 1992 (*BMI 30, or ~ 30 lbs overweight for 5’4” woman) No Data <10% 10%-14% 15-19% 20-24% 25%
 No Data <10% 10%-14% 15-19% 20-24% 25%.")
17
Obesity Trends* Among U.S. Adults BRFSS, 1993 (*BMI 30, or ~ 30 lbs overweight for 5’4” woman) No Data <10% 10%-14% 15-19% 20-24% 25%
 No Data <10% 10%-14% 15-19% 20-24% 25%.")
18
Obesity Trends* Among U.S. Adults BRFSS, 1994 (*BMI 30, or ~ 30 lbs overweight for 5’4” woman) No Data <10% 10%-14% 15-19% 20-24% 25%
 No Data <10% 10%-14% 15-19% 20-24% 25%.")
19
Obesity Trends* Among U.S. Adults BRFSS, 1995 (*BMI 30, or ~ 30 lbs overweight for 5’4” woman) No Data <10% 10%-14% 15-19% 20-24% 25%
 No Data <10% 10%-14% 15-19% 20-24% 25%.")
20
Obesity Trends* Among U.S. Adults BRFSS, 1996 (*BMI 30, or ~ 30 lbs overweight for 5’4” woman) No Data <10% 10%-14% 15-19% 20-24% 25%
 No Data <10% 10%-14% 15-19% 20-24% 25%.")
21
Obesity Trends* Among U.S. Adults BRFSS, 1997 (*BMI 30, or ~ 30 lbs overweight for 5’4” woman) No Data <10% 10%-14% 15-19% 20-24% 25%
 No Data <10% 10%-14% 15-19% 20-24% 25%.")
22
Obesity Trends* Among U.S. Adults BRFSS, 1998 (*BMI 30, or ~ 30 lbs overweight for 5’4” woman) No Data <10% 10%-14% 15-19% 20-24% 25%
 No Data <10% 10%-14% 15-19% 20-24% 25%.")
23
Obesity Trends* Among U.S. Adults BRFSS, 1999 (*BMI 30, or ~ 30 lbs overweight for 5’4” woman) No Data <10% 10%-14% 15-19% 20-24% 25%
 No Data <10% 10%-14% 15-19% 20-24% 25%.")
24
Obesity Trends* Among U.S. Adults BRFSS, 2000 (*BMI 30, or ~ 30 lbs overweight for 5’4” woman) No Data <10% 10%-14% 15-19% 20-24% 25%
 No Data <10% 10%-14% 15-19% 20-24% 25%.")
25
Obesity Trends* Among U.S. Adults BRFSS, 2002 (*BMI 30, or ~ 30 lbs overweight for 5’4” woman) No Data <10% 10%-14% 15-19% 20-24% 25%
 No Data <10% 10%-14% 15-19% 20-24% 25%.")
26
Obesity Trends* Among U.S. Adults BRFSS, 2005 (*BMI 30, or ~ 30 lbs overweight for 5’4” woman) No Data <10% 10%-14% 15-19% 20-24% 25%
 No Data <10% 10%-14% 15-19% 20-24% 25%.")
27
Obesity Trends* Among U.S. Adults BRFSS, 1991, 1995, 2000 and 2005 (*BMI 30, or ~ 30 lbs overweight for 5’4” woman) 1991 2000 1995 2005 No Data <10% 10%-14% 15-19% 20-24% 25%
 No Data <10% 10%-14% 15-19% 20-24% 25%.")
28
A Changing Society Supersized Americans are forcing a re-examination of out of date weight limits. In 1960 the average passenger weight was established at 140lbs. Elevator manufacturers now display weight limits; no longer identify number of people. Airline industry is accommodating additional passenger width. -The added weight cost airlines an extra $300 million in fuel in 2005

29
2003 Charlotte – plane crash kills 21. FAA raised average passenger weight to 174lbs 2004 Baltimore – 36ft water taxi capsizes, 5 out of 25 people drowned. Boat was 700 lbs over 3500lb capacity 2005 NY – 47 elderly tourists capsized on Lake George. The US Park Service increased passenger weight capacity to 175lbs A Changing Society

30
The year 2006 was important for obesity according to a report published by the Center for Disease Control and Prevention (CDC). Obesity Update America’s number one health threat. Leading cause of preventable death, surpassing tobacco. $320 billion is spent annually on obesity.

32
Healthcare is fast becoming one of the most dangerous jobs in the U.S.

33
Work-related musculoskeletal Disorders (MSDs) result when there is a mismatch between the physical capacity of workers and the physical demands of their job U.S. Dept. of Labor, Occupational Safety and Health Administration Musculoskeletal Disorders

34
Most work related musculoskeletal injuries occur from repetitive injuries. Overexerting the spine causes painless micro tears in the spinal discs creating cumulative damage. Cumulative Trauma Disorder

35
A serious injury may seem to be caused by a single incident, however the real cause is often the specific injury coupled with years of progressive internal weakening and damage. Cumulative Trauma Disorder

36
Overexerting the spine may result from: Safe Patient Handling Lifting improperly Lifting weight beyond a safe lifting capacity Working in a “bent over” position

37
Benefits include and increase in patient satisfaction and mobility and a decrease in: Safe Patient Handling Workers comp costs Staff/patient injury Lost time claims Staff turnover New employee training costs

38
Barb S., Director of Safety Services at Kaiser Permanente Hospital in Fresno, CA reported 12 employee injuries over a 2 week period from routine care of a nearly 500 pound patient. Sten+Barr Medical Inc. Scenario

39
Aging Workforce Degenerative and arthritic discs, out of shape, overweight, poor posture Obese patients have increased in number and are sicker. Risk Factors

40
Provide quality care Prevent injury to patient and staff Minimize costs The Unique Challenge Medical community is challenged to:

42
Most Americans have little sympathy for the overweight individual. Obesity is associated with Lack of self discipline Self indulgence, low intelligence Laziness and non compliance Surveys identify that staff felt overwhelmed by the care needs of the obese and were concerned about injury to themselves and the patient Stereotyping Resource: National Institute of Health

44
Todd, a 240 pound, 6’3” physical therapist in Indianapolis had surgery on a shoulder muscle that tore when he was moving a 450-pound patient ”who decided to hang on to my right arm when he lost his balance” Sten+Barr Medical Inc. Scenario

45
As the baby boomer generation ages, they are likely to carry their weight problems into their senior years. Never before has the healthcare community experienced the aging obese. Bariatric Geriatric

46
Plan ahead Provide staff training on policies, procedures and clinical assessment. Provide staff with appropriate size supplies. Know the weight limitations of your equipment. Collect proper size supplies and adequate assistance. Plan the transfer or transport. Be certain the receiving area is prepared for the patient General Management Tips

47
All patients deserve competent, professional care. Negative perceptions about obesity can affect the caregivers approach to caring for the bariatric patient. Sensitivity and Respect Make eye contact, call patient by name Ask the patient how to best assist them Provide adequate privacy and space

49
Vital Signs Weight Respiratory Circulation Skin Gastrointestinal, Urinary Nutrition Mobility Pharmacology Medication Administration Bariatric Assessment

50
Pulse Carotid may be difficult to palpate Use radial site A radial pulse may be the easiest way to palpate pulses if the bariatric patient has a short, thick neck Vital Signs

51
Respirations May be unable to tolerate lying flat or deep breathing as the chest and abdomen exerts pressure on the diaphragm. Vital Signs Will have changes in mental status, lab values when experiencing respiratory difficulty. Reverse Trendelenburg position may facilitate lung expansion.

52
Respirations When listening for breath sounds displace skin folds, place the diaphragm of the stethoscope firmly over the exposed area. Listen over dependent areas where the lung tissue is closest to the chest wall and where fluid is most likely to collect. Ask the patient to inhale deeply Vital Signs –Observe cough and changes of mental status during assessment

53
Blood Pressure Equipment A standard-sized blood pressure cuff should not be used on an upper arm circumference of more than 13 inches. Vital Signs The width of the cuff must be 40% to 50% of the arm’s circumference to obtain an accurate reading. A variety of cuff sizes should be available. – too small = false high

54
Management Tips Consistently utilize bariatric BP cuff Secure cuff with tape if needed Use a cuff on the forearm and feel for the radial pulse to determine the systolic pressure Validate hypotension manually “ by ear” with doppler stethoscope – modify care plan Elevating the limb may make the first systolic “click” more audible Vital Signs

55
Weight Equipment Weigh only if pertinent to care Obtaining an accurate weight can be a challenge due to size and mobility Stand-up or sling scales are only accurate up to 350 lbs.

56
Weight Management Tips Evaluate the weight capacity of your scale Utilize a bariatric bed with a scale for mobility challenged Protect the patients dignity when recording weight

57
Clinical Issues Lung capacity does not increase with weight gain Weight on abdomen and chest restricts inspiration and expiration -Obesity Hypoventilation Syndrome (OHS) -Obstructive Sleep Apnea (OSA) Respiratory Fat deposits in the diaphragm and intercostal muscles limit breathing Increased soft tissue of head, neck and tongue creates a challenge in positioning and intubation High risk for rapid desaturation
 -Obstructive Sleep Apnea (OSA) Respiratory Fat deposits in the diaphragm and intercostal muscles limit breathing Increased soft tissue of head, neck and tongue creates a challenge in positioning and intubation High risk for rapid desaturation")
58
Management Tips Identify a rescue/alternative airway management plan Identify and maintain extra size supplies – masks, longer endotracheal tubes HOB 30 degrees CPAP or BiPAP for sleep apnea Monitor O 2 saturation frequently Position shoulders and neck as needed Maintain bed in reverse Trendelenburg’s position to facilitate lung expansion Provide specific Heimlich training Respiratory

59
Clinical Issues Hypertension, Hypotension Congestive Heart Failure Cellulitis Management Tips Circulation Turn patient to left side to evaluate heart sounds on the left lateral chest wall Use aortic or pulmonic areas to right and left of sternal border of the chest for best results

60
Clinical Issues Turning and positioning is difficult Moist conditions foster the growth of yeast and fungus Increased pressure and friction within the skin Surgical wounds are prone to dehiscence Blood supply to adipose tissue is poor Tubes and catheters cause areas of pressure Improper size equipment causes areas of pressure Poor thermoregulation - Potential dehydration resulting from increased perspiration Skin

61
Management Tips Exposing the entire body is required to identify skin breakdown, bleeding, rashes or source of odor Skin Carefully assess areas of skin on skin under breasts, abdominal fold, back fold and perineal area Keep skin folds clean and dry, use powders, talc, cornstarch or skin fold management product to reduce friction and moisture (Interdry) Sprinkle antifungal products as needed Change linen/gowns frequently.
 Sprinkle antifungal products as needed Change linen/gowns frequently.")
62
Management Tips Skin Provide proper size equipment which allows for turning, repositioning and pressure redistribution Reposition panniculus with side lying position Apply a binder to minimize pressure on abdominal incisions Add extension tubing Utilize tube and catheter holders Float heels on appropriate device

63
Clinical Issues Chronic constipation and/or incontinence may result from a reluctance to ambulate Increased insulin resistance Increased abdominal pressure may cause –Gastroesophageal reflux (GERD) –Hiatal hernia –Risk for aspiration Gastro Intestinal
 –Hiatal hernia –Risk for aspiration Gastro Intestinal")
64
Management Tips Provide proper equipment and opportunity Bowel sounds take longer to distinguish. - Mark the location to maintain consistency among staff. Document location and how long you listened. Girth measurement. - Mark abdomen, leave cloth tape in place Colostomy care may require vendor support Provide right-size commode, incontinence products and hygiene assistance Gastro Intestinal

65
Clinical Issues Functional incontinence and UTI may result from a reluctance to ambulate or lack of bariatric equipment Stress incontinence is caused by the large abdomen increasing intraabdominal pressure Urinary

66
Management Tips Encourage self toileting Ask about usual bowel and bladder routine Provide appropriate size commode chair, incontinence products and hygiene assistance including cleansers, barriers, hair dryer on cool Urinary

67
Management Tips Gather appropriate supplies and adequate assistance Lateral recumbent or supine position (female) Drop one leg to side of bed or use lift to elevate leg Approach from foot of bed Add extension tubing and secure Hang bag from foot board Catheter Insertion
 Drop one leg to side of bed or use lift to elevate leg Approach from foot of bed Add extension tubing and secure Hang bag from foot board Catheter Insertion")
68
Clinical Issues Most ignored assessment –Most common diagnosis = deferred –Embarrassing –Limited hygiene Increased endometrial cancer in obese women Gynecological Management Tips Gather appropriate supplies and adequate help –Longer speculum –Sit on metal bedpan Recommend pelvic floor relaxation

69
Clinical Issues Malnutrition, undernourished Lack essential nutrients necessary for healing Management Tips Complete a comprehensive assessment of nutritional status – Diet history – Evaluate lab data including serum albumin, pre-albumin, lymphocyte – Clinical examination – Anthropometric measurement Nutrition

70
Clinical Issues Chronic back pain Flattening of the arches of the feet Abdominal girth may obstruct the patients view of their feet, gait may be wide-based to accommodate a top- heavy mass, thighs may position legs further apart Transient parasthesias of the extremities may result from positioning or bunched clothing Sensory neuropathy and amputations Mobility

71
Management Tips Good body mechanics is essential for staff safety however it is no longer enough Interview patients about their normal level of activity Mobility – Tolerance for standing and walking – When was last time he or she walked – Ambulation aids and toileting routines Assess strength, movement and endurance of all extremities prior to activity

72
Mobility Note: Common and predictable complications related to obesity may result from caregivers inability to transfer and mobilize patients. An inadequately trained staff results in patient isolation

73
Management Tips Provide the proper size bed and mattress – Lock wheels, position bed against the wall – Raise bed to the highest setting to push – Trapeze allows the resident to assist – Trendelenburg facilitates boosting – Reverse Trendelenburg facilitates breathing – Scale weighs immobile patient Mobility Emergency preparedness plan must include evacuation of extended capacity equipment

74
Mobility Management Tips Provide the proper size and type of lift and sling Lifting requires a unique approach to protect the patient and reduce worker injury

75
Key Bed Commode Lift Transfer Devices

76
Clinical Issues Altered absorption of medication Drug levels may be subtherapeutic or toxic Management Tips Obtain accurate weight on admission Consult with pharmacist to verify dosing and administration routes are safe and effective Calculate dosage by : – Actual Body Weight for meds highly soluble in fat (opiates, analgesics) – Ideal Body Weight for meds distributed in lean tissue (acetaminophen, digoxin) Pharmacology
 – Ideal Body Weight for meds distributed in lean tissue (acetaminophen, digoxin) Pharmacology")
77
Clinical Issues Oral meds rely on normal pH for proper absorption, obesity encourages lower gastric pH Medication Administration Topical meds-cutaneous tissue is not well vascularized Subcutaneous injection may be inappropriate due to low vascularization Skin patches-cutaneous tissue is not well perfused IM administration may be difficult to access –delayed onset –accumulation causes overdose IV access may be difficult as veins are deep

78
Management Tips Assess dosages and administration routes Monitor effectiveness of weight calculated dosages to ensure therapeutic effect Oral/topical meds doses may need to be increased or given more frequently IM – use longer needles and whatever muscle is closest to surface. Medication Administration Peripherally inserted central catheter (PICC) if peripheral access is limited / long term Epidural drug absorption is uniform
 if peripheral access is limited / long term Epidural drug absorption is uniform.")
79
All obese patients have some degree of glucose intolerance which predisposes them to hyperglycemia Check glucose on all ill or dehydrated obese patients or any who report “thirst”, “fatigue”, “weakness”, increased urination” Glucose

80
Every preventive effort should be made to avoid falling or taking a position on the floor. If an incident should occur, getting up must be done without injury to the staff and patient. Motion Related Incidents Bring a footstool or solid chair close at hand as a balance point or resting spot for the patient Use a strong chair behind the shoulders to tilt into a sitting position Use a mechanical lift or blankets and adequate help to lift - Continue nursing care Call Emergency Services as needed Implement your Performance Improvement Process

81
Obese patients suffer more pain and disability from positions of restraint Restraints Adjust knee gatch to lessen strain on knees and prevent sliding downward Maintain high Fowlers Position to maximize respiratory efficiency Offer Range of Motion exercise Facilitate early restraint release

82
- Transport and transfer - Emergency assistance for unplanned transfer - Radiology services (Xray, CT, MRI, Ultrasound) - Funeral Services - Support and advocacy groups How do you increase bariatric census while cost effectively providing safe, quality care for this population of size? Your facility must become the Community Bariatric resource including solutions for: A Model for Success

83
Features of an ambulance specially designed to safely transport bariatric residents include: – EC box type resident compartment – 1000 # capacity – Gurney with hydraulic lift – Aluminum rear loading ramps – Winch system Contacts: American Medical Response www.amr-inc.com “Build Your Own Bariatric Unit” www.swambulance.com Transport and Transfer

84
Firefighters are perceived as “specially trained in rescue” Specialized lifting teams have been implemented in emergency rescue. Emergency Assistance

85
Standard imaging methods (X-rays, Ultrasound, CT Scan, MRI) cannot penetrate excessive fat, inhibiting diagnosis and treatment of the “technically difficult resident”. Resource: www.usa.siemens.com Proper diagnosis may be inconclusive and treatment is compromised because of obesity New York – Bronx Zoo receives dozens of calls requesting use of their large animal MRI Radiology Services

86
“Morticians are forced to purchase wider work tables, plus size caskets and vaults to place into larger cemetery plots.” Standard weight capacity for caskets is 300 lbs. “ 300lb plus bodies are becoming common and moving them is a danger to employees. A funeral director recently incurred a back injury and was out of work for a month after an abortive attempt to move an obese corpse”. Science Daily Oct 2005 Goliath Caskets specializes in up to 1000lb capacity (52 inches in width) Resources Goliathcaskets.com HillRom/Dimensions.com End of Life Solutions Funeral Services
 Resources Goliathcaskets.com HillRom/Dimensions.com End of Life Solutions Funeral Services.")
87
Body Size and levels of body fat have considerable effects on the operation of cremation equipment. Standard weight capacity is 300lbs. Cremation of heavy human remains requires: Resources: www.cremationassociation.org Larger capacity chamber with an adequate opening. Special positioning. Additional monitoring. Longer processing. Funeral Services

88
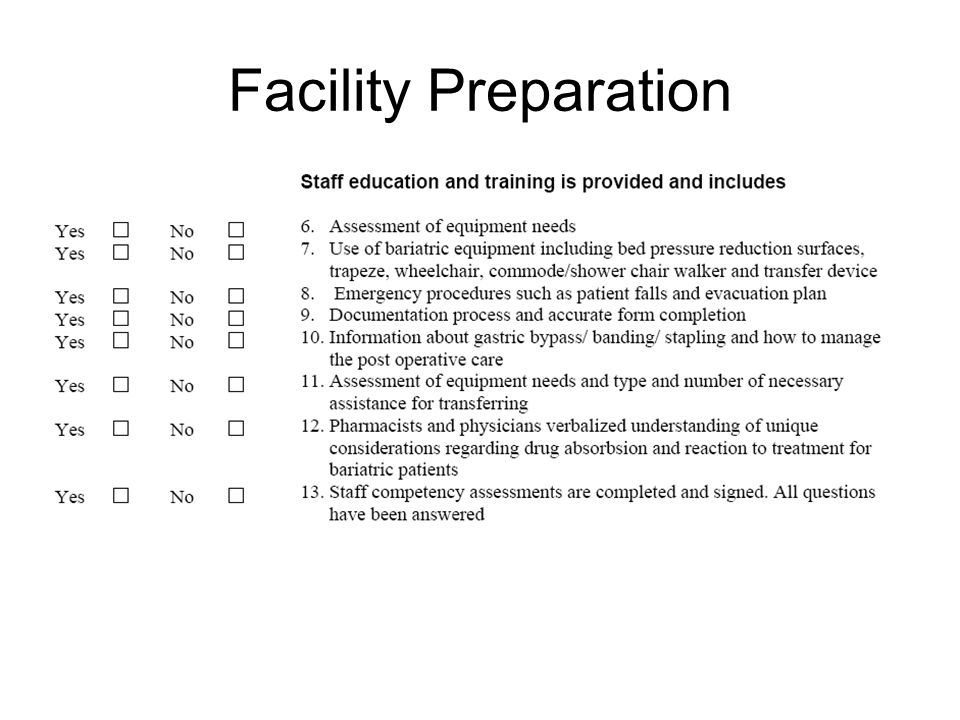
Facility Preparation

94
A case study is used to illustrate the unique challenges of bariatric care and encourage discussion about predicting and planning for the admission of an obese patient. Case Study Sonia is an alert 54 year old female who lived at home with her husband until she fell and fractured her left hip. Hip surgery (ORIF) was performed; during her hospital stay she developed a urinary track infection UTI) and 2 pressure ulcers; a Stage IV on her coccyx and Stage II on right heel.
 was performed; during her hospital stay she developed a urinary track infection UTI) and 2 pressure ulcers; a Stage IV on her coccyx and Stage II on right heel..")
95
Sonia’s diabetes, COPD and diabetics are controlled by oral medications however her respiratory symptoms have worsened as a result of her immobility. Her left hip incision is infected. Case Study Height: 4 ft 10 in Weight: 295 lbs BMI: 61 Waist Circumference: 56 Vital Signs Temperature 99.3 Pulse 98 Respirations 80 BP 188/130

96
Admitting Diagnosis: - Post Left Hip Fracture - Respiratory Disease( COPD ) - Diabetes - Pressure Ulcers - Urinary Track Infection( UTI ) - Dehydration - Pressure Ulcers - Hypertension - Arthritis Admitting Diagnosis
 - Diabetes - Pressure Ulcers - Urinary Track Infection( UTI ) - Dehydration - Pressure Ulcers - Hypertension - Arthritis Admitting Diagnosis")
97
Respiratory:Breath sounds diminished, dyspnea Skin:Moist and diaphoretic Non healing pressure ulcers Stage IV coccyx, Stage II R heel Infected L hip incision open and draining Edema: R and L feet and lower legs Elimination: Urge and Stress Incontinence, painful urination Constipation, last BM 12 days ago Abdomen distended Pain:L hip and L kneePain scale 8-9 BackPain scale 6 All major joints Pain scale 6 Admission Assessment

98
Sonia is uncooperative with transferring and repositioning due to her pain. Her long hospital stay and immobility have left her very weak and fearful of falling. The Stage IV pressure ulcer on her coccyx has heavy drainage and undermining. Comments

99
- Maintain hip precautions - Full weight bearing status - Out of bed - Turn and reposition q2h - Mattress per protocol - No concentrated sweets - Encourage fluids - Weigh weekly - BP and pulse qd - Pulse Oximetry q week and prn, -O 2 to maintain SAT 90% - Obtain BS qd, notify physician if BS is >160 - DiaBeta 1.25mg po qd - Cover L hip incision c border gauze and monitor for s/s of infection. Change qd/pm - Initiate Negative Pressure Wound Therapy (NPWT) to coccyx wound per protocol - Apply Hydrocolloid to R heel pressure ulcers, change q4d/prn - Generic antibiotic 500mg po qd - Lasix 40mg qd po - Benicar 20mg qd po - Demerol 100mg IM q 6h - Tylenol #3 po q6h prn for pain - Prednisone 10mg po qd - Ducolax (1) po hs prn Physician’s Orders Identify unique supplies, equipment and staff training necessary for Sonia’s care
 to coccyx wound per protocol - Apply Hydrocolloid to R heel pressure ulcers, change q4d/prn - Generic antibiotic 500mg po qd - Lasix 40mg qd po - Benicar 20mg qd po - Demerol 100mg IM q 6h - Tylenol #3 po q6h prn for pain - Prednisone 10mg po qd - Ducolax (1) po hs prn Physician’s Orders Identify unique supplies, equipment and staff training necessary for Sonia’s care.")
100
Pre-Admission Assessment

101
RecoverCare offers continuing education (CEU’s) from the convenience of your own computer. Visit us at: www.stenbarr.com/sbu.asp On-line Education Programs Practical Aspects of Bariatric Care

102
Please complete your Program Evaluation Thank You Carolyn Brown M.Ed., RN, ARM,FCCWS National Director of Clinical Services - RecoverCare Cbrown@recovercare.com 14350 Carlson Circle Tampa, Florida 33626

Similar presentations










? It’s the law!! Safe patient handling (SPH) means the use of engineering controls, transfer aids, or assistive devices.>")
















