Download presentation
Presentation is loading. Please wait.

1
HUMAN RENAL SYSTEM PHYSIOLOGY Lecture 11,12
By: Lect. Dr. Zainab al-Amily

2
Objectives Describe metabolic acidosis and its compensatory mechanism
Describe metabolic alkalosis and its compensatory mechanism Describe respiratory acidosis and its compensatory mechanism Describe respiratory alkalosis and its compensatory mechanism

3
is caused by a decreased HCO3 concentration in the blood.
Acid-base disorders METABOLIC ACIDOSIS is caused by a decreased HCO3 concentration in the blood. can result from: increased production of fixed acids such as ketoacids or lactic acid; ingestion of fixed acids such as salicylic acid; Methanol/formaldehyde poisoning; Ethylene glycol poisoning the inability of the kidneys to excrete the fixed acids produced from normal metabolism; or loss of HCO3 via the kidneys or the gastrointestinal tract (Diarrhea)
")
4
The arterial blood profile seen in metabolic acidosis is:
pH ↓ [HCO3 ] ↓ Pco2 ↓ Although metabolic acidosis can be caused by a frank loss of HCO3 , as in diarrhea most often it is caused by an excess of fixed acid in the body.

5
The following sequence of events occurs in generation of metabolic acidosis to produce this blood profile. 1. Gain of fixed H+. Excess fixed H is accumulated in the body either through increased production or ingestion of fixed acid or from decreased excretion of fixed acid. 2. Buffering. The excess fixed H is buffered in both ECF and ICF. In ECF, the H is buffered primarily by HCO3, which produces a decrease in HCO3 concentration. The decrease in HCO3 concentration causes a decrease in pH, In ICF, the excess fixed H is buffered by organic phosphates and proteins.

6
To utilize these intracellular buffers, H first must enter the cells.
H can enter the cells with an organic anion such as ketoanion, lactate, or formate, or it can enter the cells in exchange for K. When the H is exchanged for K, hyperkalemia occurs 3.Respiratory compensation. Decreased arterial pH stimulates peripheral chemoreceptors in the carotid bodies, which respond by causing hyperventilation. In turn, hyperventilation produces a decreased PCO2, which is the respiratory compensation for metabolic acidosis. [HCO3 ] ( ↓ Primary disturbance) Pco ( ↓ Respiratory compensation)
 Pco2 ( ↓ Respiratory compensation)")
7
The primary disturbance is decreased HCO3 concentration, which, by itself, would lead to a profound decrease in pH. The respiratory compensation,( hyperventilation), decreases the PCO2, which tends to normalize the ratio of HCO3/ PCO2 and to normalize the pH. 4. Renal correction. Buffering and respiratory compensation occur quickly. The ultimate correction of metabolic acidosis occurs in the kidneys and takes several days. The excess fixed H will be excreted as titratable acid and NH4 Simultaneously, new HCO3 will be synthesized and reabsorbed by the kidneys to replace the HCO3 that was consumed earlier in buffering. In this way, the blood HCO3 concentration will be returned to normal.
, decreases the PCO2, which tends to normalize the ratio of HCO3/ PCO2 and to normalize the pH. 4. Renal correction. Buffering and respiratory compensation occur quickly. The ultimate correction of metabolic acidosis occurs in the kidneys and takes several days. The excess fixed H will be excreted as titratable acid and NH4. Simultaneously, new HCO3 will be synthesized and reabsorbed by the kidneys to replace the HCO3 that was consumed earlier in buffering. In this way, the blood HCO3 concentration will be returned to normal.")
9
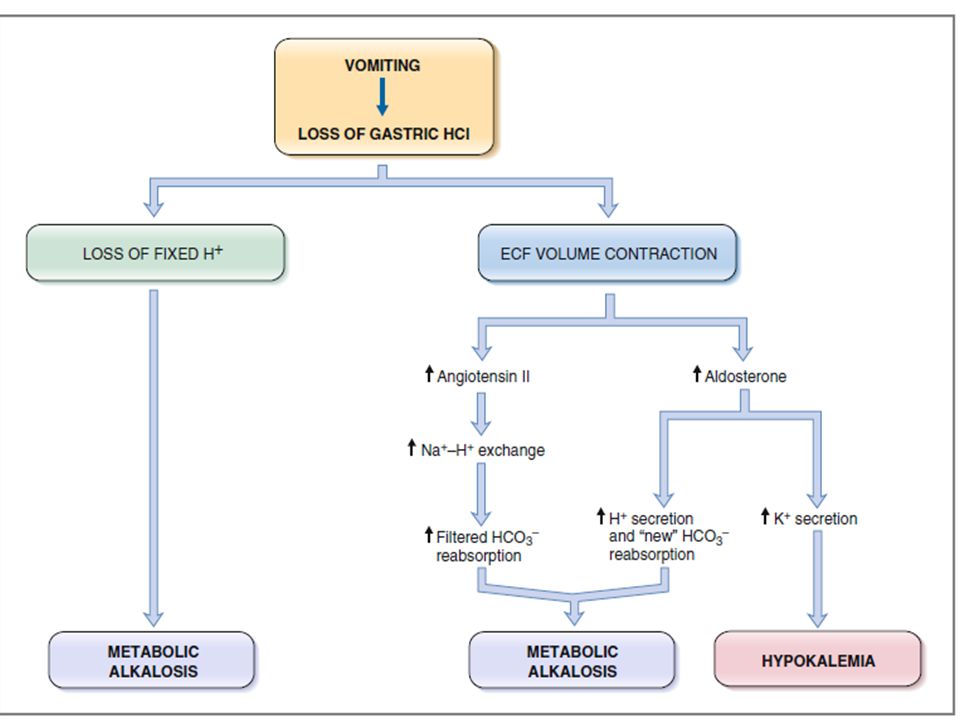
METABOLIC ALKALOSIS is caused by an increased HCO3-concentration in the blood. is the result of loss of fixed H from the gastrointestinal tract; loss of fixed H from the kidney (e.g.,hyperaldosteronism); administration of solutions containing HCO3 or ECF volume contraction (e.g., administration of diuretics)
; administration of solutions containing HCO3. or ECF volume contraction (e.g., administration of diuretics)")
10
The arterial blood profile seen in metabolic alkalosis
pH ↑ [HCO 3 ] ↑ Pco2 ↑ Although metabolic alkalosis can be caused by administration of HCO3, most often it is caused by loss of fixed acid from the body

11
The following sequence of events occurs in the generation of metabolic alkalosis to produce this blood profile. 1. Loss of fixed acid. The classic example of metabolic alkalosis is vomiting, in which HCl is lost from the stomach. The gastric parietal cells produce H and HCO3 from CO2 and H2O. The H is secreted with Cl into the lumen of the stomach to aid in digestion, and the HCO3 enters the blood. In normal persons, the secreted H moves from the stomach to the small intestine, where a low pH triggers the secretion of HCO3 by the pancreas. Thus, normally, the HCO3 added to blood by the parietal cells is later removed from blood in the pancreatic secretions.

12
when vomiting occurs, H is lost from the stomach and never reaches the small intestine.
HCO3 secretion from the pancreas, therefore, is not stimulated, and the HCO3- remains in the blood, resulting in an increase in HCO3- concentration. The increase in HCO3 concentration causes an increase in pH,

14
Which of the following is a cause of metabolic alkalosis?
(A) vomiting (B) Chronic renal failure (C) Ethylene glycol ingestion (D) diarrhea (E) Hypoaldosteronism
 vomiting. (B) Chronic renal failure. (C) Ethylene glycol ingestion. (D) diarrhea. (E) Hypoaldosteronism.")
15
2. Buffering. occurs in both ECF and ICF.
To utilize ICF buffers, H leaves the cells in exchange for K, and hypokalemia occurs. 3. Respiratory compensation. Increased arterial pH inhibits the peripheral chemoreceptors, which respond by causing hypoventilation. In turn, hypoventilation produces an increased PCO2, which is the respiratory compensation for metabolic alkalosis. [HCO 3 ] ( ↑ Primary disturbance) Pco2 ( ↑ Respiratory compensation
 Pco2 ( ↑ Respiratory compensation.")
16
The primary disturbance in metabolic alkalosis is an increased HCO3 concentration that, by itself, would lead to a profound increase in pH The respiratory compensation, hypoventilation, increases the PCO2, which tends to normalize the ratio of HCO3 /CO2 and to normalize the pH. 4. Renal correction. The correction of metabolic alkalosis should be the most straight forward of all the acid-base disorders.

17
Since the primary disturbance is increased HCO3 concentration, restoration of acid-base balance will take place when the excess HCO3 is excreted by the kidneys. This can be accomplished because the renal tubule has a finite reabsorptive capacity for filtered HCO3 When the filtered load of HCO3 exceeds the reabsorptive capacity, HCO3 is excreted in the urine, eventually reducing the HCO3 concentration to normal.

18
. A patient arrives at the emergency room with low arterial pressure, reduced tissue turgor, and the following arterial blood values: pH = 7.69 [HCO3 –] = 57 mEq/L PCO2 = 48 mm Hg Which of the following responses would also be expected to occur in this patient? (A) Hyperventilation (B) increased K+ secretion by the distal tubules (C) Increased ratio of H2PO4 – to HPO4–2 in urine (D) Exchange of intracellular H+ for extracellular K+ (E) Hyperaldosteronism
![A patient arrives at the emergency room with low arterial pressure, reduced tissue turgor, and the following arterial blood values: pH = 7.69 [HCO3 –] = 57 mEq/L PCO2 = 48 mm Hg Which of the following responses would also be expected to occur in this patient.](http://slideplayer.com/slide/4663503/15/images/18/A+patient+arrives+at+the+emergency+room+with+low+arterial+pressure%2C+reduced+tissue+turgor%2C+and+the+following+arterial+blood+values%3A+pH+%3D+7.69+%5BHCO3+%E2%80%93%5D+%3D+57+mEq%2FL+PCO2+%3D+48+mm+Hg+Which+of+the+following+responses+would+also+be+expected+to+occur+in+this+patient..jpg "(A) Hyperventilation (B) increased K+ secretion by the distal tubules (C) Increased ratio of H2PO4 – to HPO4–2 in urine (D) Exchange of intracellular H+ for extracellular K+ (E) Hyperaldosteronism .")
20
RESPIRATORY ACIDOSIS is caused by hypoventilation, which results in retention of CO2. The retention of CO2 can be caused by inhibition of the medullary respiratory center, paralysis of respiratory muscles, airway obstruction, or failure to exchange CO2 between pulmonary capillary blood and alveolar gas The arterial blood profile seen in respiratory acidosis is pH ↓ [HCO 3 ] ↑ Pco2 ↑

21
The following sequence of events occurs in the generation of respiratory acidosis to produce this blood profile: 1. Retention of CO2. Hypoventilation causes retention of CO2 and an increase in PCO2. The increased PCO2 is the primary disturbance in respiratory acidosis

22
2. Buffering. Buffering of the excess CO2 occurs exclusively in ICF, especially in red blood cells. To utilize these intracellular buffers, CO2 diffuses across the cell membranes. Within the cells, CO2 is converted to H and HCO3, and the H is buffered by intracellular proteins (e.g., hemoglobin) and by organic phosphates 3. Respiratory compensation. There is no respiratory compensation for respiratory acidosis, since respiration is the cause of this disorder.
 and by organic phosphates. 3. Respiratory compensation. There is no respiratory compensation for respiratory acidosis, since respiration is the cause of this disorder.")
23
4. Renal compensation. Renal compensation for respiratory acidosis consists of increased H excretion as titratable acid and NH4 and increased synthesis and reabsorption of new HCO3 . Reabsorption of new HCO3 increases the HCO3 concentration The Henderson-Hasselbalch equation can be used to understand why the increased HCO3 concentration is a compensatory response [HCO 3 ] ( ↑ Renal compensation) Pco ( ↑ Primary disturbance)
 Pco2 ( ↑ Primary disturbance)")
24
In acute respiratory acidosis, renal compensation
has not yet occurred, and the pH tends to be quite low On the other hand, in chronic respiratory acidosis, renal compensation is occurring, which increases the HCO3 concentration and tends to normalize both the ratio of HCO3/CO2 and the pH. The difference between acute and chronic respiratory acidosis lies in the renal compensation

25
RESPIRATORY ALKALOSIS
is caused by hyperventilation,which results in excessive loss of CO2. Hyperventilation can be caused by: direct stimulation of the medullary respiratory center, hypoxemia (which stimulates peripheral chemoreceptors), Mechanical ventilation The arterial blood profile seen in respiratory alkalosis is pH ↑ [HCO3 ] ↓ Pco2 ↓
, Mechanical ventilation. The arterial blood profile seen in respiratory alkalosis is. pH ↑ [HCO3 ] ↓ Pco2 ↓")
26
The following sequence of events occurs in the generation of respiratory alkalosis to produce this blood profile: 1. Loss of CO2. Hyperventilation causes an excessive loss of CO2 and a decrease in PCO2. The decreased PCO2 is the primary disturbance in respiratory alkalosis and, as predicted by the Henderson-Hasselbalch equation, causes an increase in pH The decreased PCO2 also causes a decreased concentration of HCO3

27
2. Buffering. Buffering occurs exclusively in ICF, particularly in red blood cells. In this case, CO2 leaves the cells and intracellular pH increases. 3. Respiratory compensation. As with respiratory acidosis, there is no respiratory compensation for respiratory alkalosis, since respiration is the cause of the disorder.

28
4. Renal compensation. Renal compensation for respiratory alkalosis consists of decreased excretion of H as titratable acid and NH4 and decreased synthesis and reabsorption of new HCO3 Decreased reabsorption of HCO3 decreases the HCO3 concentration The Henderson-Hasselbalch equation can be used to understand why the decreased HCO3 concentration is a compensatory response [HCO3 ] ( ↓ Renal compensation) Pco2 ( ↓ Primary disturbance)
 Pco2 ( ↓ Primary disturbance)")
29
In acute respiratory alkalosis, renal compensation
has not yet occurred, and pH is quite high In chronic respiratory alkalosis, renal compensation is occurring, which further decreases the blood HCO3 concentration and tends to normalize both the ratio of HCO3/CO2 and the pH. The difference between acute and chronic respiratory alkalosis lies in renal compensation

30
A patient has the following arterial blood values:
pH = 7.52 PCO2 = 20 mm Hg [HCO3–] = 16 mEq/L Which of the following statements about this patient is most likely to be correct? (A) He is hypoventilating (B) He has decreased ionized [Ca2+] in blood (C) He has almost complete respiratory compensation (D) He has an acid–base disorder caused by overproduction of fixed acid (E) Appropriate renal compensation would cause his arterial [HCO3–] to increase
 He is hypoventilating. (B) He has decreased ionized [Ca2+] in blood. (C) He has almost complete respiratory compensation. (D) He has an acid–base disorder caused by overproduction of fixed acid. (E) Appropriate renal compensation would cause his arterial [HCO3–] to increase.")
Similar presentations














![1. pH = - log [H + ] H + is really a proton Range is from 0 - 14 If [H + ] is high, the solution is acidic; pH < 7 If [H + ] is low, the solution.](/15/4651316/big_thumb.jpg "1. pH = - log [H + ] H + is really a proton Range is from 0 - 14 If [H + ] is high, the solution is acidic; pH < 7 If [H + ] is low, the solution.>")





 H + concentration in the body.>")
![Renal Acid-Base Balance. Acid An acid is when hydrogen ions accumulate in a solution. It becomes more acidic [H+] increases = more acidity CO 2 is an.](/20/5962628/big_thumb.jpg "Renal Acid-Base Balance. Acid An acid is when hydrogen ions accumulate in a solution. It becomes more acidic [H+] increases = more acidity CO 2 is an.>")
 concentration. More H + = more acidic = lower.>")