Download presentation
Presentation is loading. Please wait.

1
Penetrating Neck Injuries

2
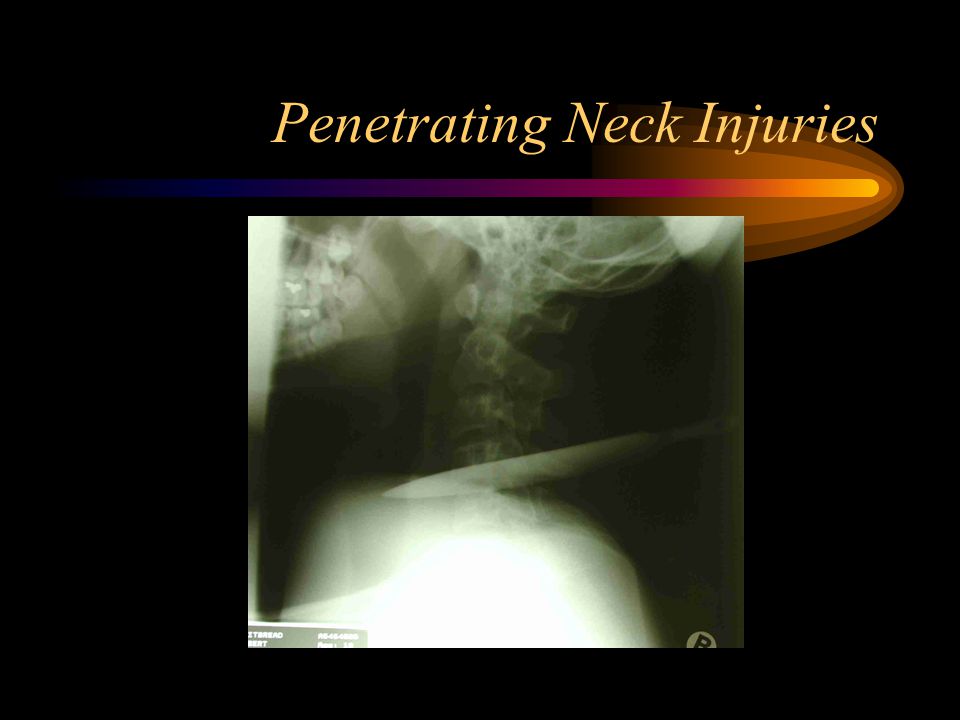
Case 1 –19 year old male in Casuarina –stabbed back of neck with steak knife (8cm) –Zone II injury –haemodynamically stable
 –Zone II injury –haemodynamically stable")
3
Penetrating Neck Injuries

5
Case 2 –27 year old male –stabbed in anterior triangle –Zone I injury –required resuscitation at scene –fixed dilated pupils on presentation

6
Penetrating Neck Injuries

7
Epidemiology –stab wounds or low velocity missiles –young, otherwise healthy and intoxicated –carotid artery involved in 6% –account for 22% of all cervical vascular trauma

8
Penetrating Neck Injuries Classification –Anterior/Posterior neck triangles –Zones I = Between clavicle and cricoid II = cricoid and angle of mandible III = angle of mandible to BOS

9
Penetrating Neck Injuries Zone II most common (47%) Zone I (18%) and Zone III (19%) multiple zones (16%)
 Zone I (18%) and Zone III (19%) multiple zones (16%)")
10
Penetrating Neck Injuries Injuries –arterial –venous –neurological –oesophagus –airways

11
Penetrating Neck Injuries Findings: airways –airways obstruction –haemoptysis –air bubbling through wound –subcutaneous emphysema –hoarseness –painful swallowing –haematemesis

12
Penetrating Neck Injuries Findings: vascular –haemodynamic instability –haematoma –reduced pulses (CA, STA, RA) –bruit/thrill
 –bruit/thrill")
13
Penetrating Neck Injuries Findings: neurological –GCS –focal UMN signs –cranial nerves (VII, IX, X, XI, XII) –cervical spinal cord –Horner’s syndrome –Brachial plexus
 –cervical spinal cord –Horner’s syndrome –Brachial plexus")
14
Penetrating Neck Injuries Management –ABCD –surgical exploration for ‘hard’ signs of vascular injury (shock, active beeding, enlarging haematoma, bruit/thrill) –stable patients with Zone I and III injuries: angiography with selective intervention
 –stable patients with Zone I and III injuries: angiography with selective intervention")
15
Penetrating Neck Injuries Zone II Controversies –Mandatory versus Selective exploration –Accuracy of physical examination –investigation

16
Penetrating Neck Injuries Mandatory exploration –Apffelstaedt et al. World J Surg 1994 393 consecutive patients over 20 months 30% of (+) neck explorations had absent clinical signs low morbidity/mortality in negative explorations investigations have false (-) and false (+) rates
 neck explorations had absent clinical signs low morbidity/mortality in negative explorations investigations have false (-) and false (+) rates.")
17
Penetrating Neck Injuries Selective exploration –Demetriades et al. World J Surg 1997 223 patients over 20 months, 176 had angiography 34(19%) had positive angiography, 8% required treatment 34 patients with soft signs, 8 had (+) angiogram but only 1 required treatment mandatory exploration leads to high rate (30-89%) of unnecessary operations
 had positive angiography, 8% required treatment 34 patients with soft signs, 8 had (+) angiogram but only 1 required treatment mandatory exploration leads to high rate (30-89%) of unnecessary operations.")
18
Penetrating Neck Injuries Physical Examination –Sekharan et al, J Vasc Surg 2000 145 zone II injuries, retrospective chart review 31 had hard signs, 90% (+) exploration 23 had angiogram due to proximity to major structures or involving more than 1 zone. 91patients were observed without imaging or surgery with no evidence of subsequent vascular injury up to 2 weeks.

19
Penetrating Neck Injuries Physical Examination –accuracy of 99% in diagnosing significant vascular injuries with a false negative rate comparable to angiography. –However most studies are prolonged retrospective studies with no uniform protocol –May miss occult lesions such as smooth narrowings, intimal irregularities and small psedoaneurysms and AV fistulas

20
Penetrating Neck Injuries Duplex Ultrasound –Demetriades et al. 99 patients had duplex 11 lesions correctly identified (6 VA, 4 CA, 1 SCA) 1 missed lesion (CCA/VA small intimal tears) sensitivity 91%, specificity 100%, PPV 100% and NPV 99%.
 1 missed lesion (CCA/VA small intimal tears) sensitivity 91%, specificity 100%, PPV 100% and NPV 99%..")
21
Penetrating Neck Injuries CT –Mazolewski et al. J Trauma 2001 14 stable patients Level 2 sensitivity 100%, specificity 91%, PPV 75% and NPV 100%

22
Penetrating Neck Injuries vertebral artery injury –clinical presentation and outcome related to associated injuries. –72% have no evidence of arterial trauma –low incidence of brain stem ischaemia with unilateral VA ligation

23
Penetrating Neck Injuries oesophageal injury –very low prevalence –Demetriades et al only symptomatic or obtunded patients should undergo investigations

24
Penetrating Neck Injuries venous injury –ligation for major cervicomediastinal venous trauma is generally well tolerated

Similar presentations




>")

>")












