Download presentation
Presentation is loading. Please wait.

1
Head and Neck Trauma Hosseini M. M.D Head and Neck Surgeon
Head and Neck Trauma Hosseini M. M.D Head and Neck Surgeon Rasoul Akram Hospital Iran University

3
Airway Vascular system Nervous system Esophagus/Hypopharynx Bone

4
Signs and symptoms of penetrating neck trauma
Airway Respiratory distress Stridor Cyanosis Hemoptysis Hoarseness Tracheal deviation Subcutaneous emphysema Sucking wound

5
Vascular system Hematoma Persistent bleeding Neurologic deficit
Absent pulse Hypovolemic shock Bruit Thrill Change of sensorium

6
Nervous system Hemiplegia Quadriplegia Coma Cranial nerve deficit
Change of sensorium Hoarseness

7
Esophagus / hypopharynx
Subcutaneous emphysema Dysphagia Odynophagia Hematemesis Hemoptysis Tachycardia Fever

10
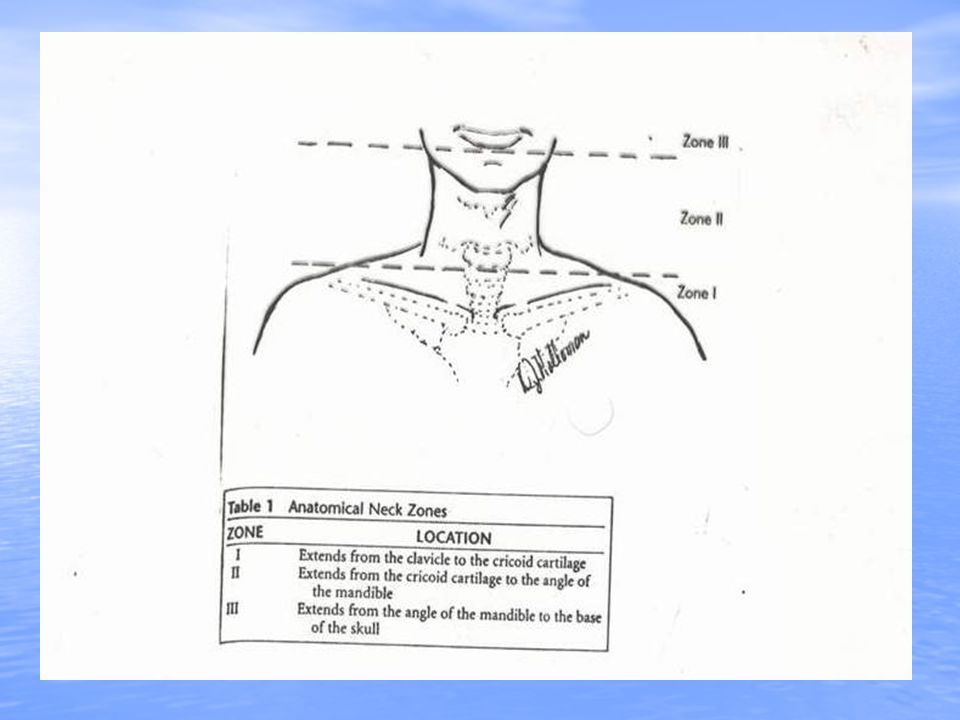
Zone I : 1-Close proximity to thorax (dangerous)
2-Protect by bony thorax and clavicle 3-Surgical exploration is difficult 4-Mortality 12% 5-Mandatory exploration is not recommended 6-Angiography 7-Right side : median sternotomy 8-Left side : left anterior thoracotomy Zone I :

11
Zone II : 1-The most involved zone (60% - 75%)
2-Mandetory versus selective

12
Zone III : 1- Protect by skeletal structures
2- Surgical exploration is difficult (need to divide or displace the mandible) 3-Cranial nerves injuries 4- Angiography and barium swallow (in stable patients and no lifethreating symptoms) 5-Frequent intraoral examination
 3-Cranial nerves injuries. 4- Angiography and barium swallow. (in stable patients and no lifethreating symptoms) 5-Frequent intraoral examination.")
15
- Temporal (frontal) Inability to raise the eyebrow - Zygoma (malar) Inability to close the eyelids - Buccal Inability to smile - Marginal mandibular Inability to frown
 Inability to raise the eyebrow - Zygoma (malar) Inability to close the eyelids - Buccal Inability to smile - Marginal mandibular Inability to frown")
16
Facial nerve injuries 1-Maxillofacial trauma
2-Serious functional disabilities and aesthetic defects 3-Posterior half of parotid gland has deep laceration 4-Repaired five or main trunk (clean,sharp division)
")
17
Signs of immediate Lifethreatening Injuries
1-Massive bleeding 2-Expanding hematoma 3-Nonexpanding hematoma in the presence of hemodynamic instability 4-Hemomediastinum 5-Hemothorax 6-Hypovolemic shock

18
Diagnostic evaluation
1- Full examination of the unclothed body (entrance - exit ) 2- Full neurologic examination 3- Chest X - Ray ( Hemothorax pneumothorax-pneumomediastinum) 4- Cervical spine X- Ray 5- Flexible endoscopy – arteriography (24 hours available)
 2- Full neurologic examination. 3- Chest X - Ray ( Hemothorax. pneumothorax-pneumomediastinum) 4- Cervical spine X- Ray. 5- Flexible endoscopy – arteriography. (24 hours available)")
19
Angiography Indications : Wounds near vessel in zone I or zone III
Contraindications : Expanding hematoma Profound shock Uncontrolled bleeding Accuracy : %

20
Barium swallow Indications : Hematemesis Contraindications : Intubated
Drooling Dysphagia Vocal cord paralysis Contraindications : Intubated Saliva in wound Unstable pt. Accuracy : 90%

21
Direct laryngoscopy and broncoscopy
Indications : Vocal cord paralysis Hoarseness Tenderness or crepitance over larynx Subcutaneous emphysema Hemoptysis Contraindications : None Accuracy : %

22
Esophagoscopy Indications Suspected but unconfirmed injury
by Barium swallow Intubated Laryngeal or tracheal injury Vascular injury in zone II or zone III Contraindications : None Accuracy : %

23
The leading cause of death
From penetrating neck injuries is hemorrhago from vascular structures ( 50% )
")
24
Mandatory Versus Elective Exploration
1-Lifethreatening 2-Not lifethreatening

25
Stable patients: 1-Mandatory exploration for all
penetrating neck wounds 2-Selective exploration with observation

26
Subcutaneous emphysema In the neck or face
1-Sinus 2- Hypopharynx 3- Laryngothracheal complex 4- Pulmonary parenchyma 5- Esophagus

27
Esophageal injuries 1-Blunt (rare) 2-16/288 (when penetrate platysma)
3-Air in mediastinum 4-Pain 5-Hematemesis 6-Hoarseness 7-Barium swallow 8-Endoscopy (rigid) 9-N.P.O (7-10 days)
 9-N.P.O (7-10 days)")
28
Small injuries of Trachea
Primary repair No tracheotomy Absorbable sutures (3-0 or 4-0) Transversely sutures Ring above and below No drain
 Transversely sutures. Ring above and below. No drain.")
29
Large defects Anterior : Convert to tracheotomy Posterior &lateral :
Close primary & tracheotomy Very large defect : Primary anastomosis(5-6 rings)
")
30
Initial management 1-Airway 2-Blood perfusion maintenance 3-Clarification and classification of the severity of wound

33
Parotid duct injuries - Opening opposite the second upper molar
- Orifice of Stensen s duct should be probed - Repair over catheter

41
Penterating Neck Injury
Is immediately life-threatening Is not

42
Signs Of Immediate L. T. -Massive bleeding -Expanding hematoma
-Nonexpanding hematoma in the presence of hemodynamic instability -Hemomediastinum -Hemothorax -Hemovolemic shock

43
Stable patient -Mandatory exploration for all pent.neck wounds
-Selective exploration and observation -50-70% of pt. had negative exploration

44
-World war II mortality of penetrating neck wound 7-15%
-End of vietnam war 3-6%

45
Transcervical injuries should be reported seperately from zone I , II , III injuries.
Transcervical penetrating neck wounds when the projectile crosses the midline , have 100% vascular or aerodigestive injury.

46
Initial management 1-Airway establishment
2-blood perfusion maintenance 3-clarification & classification of severity of the wounds

47
Airway a-Intubation b-cricothyroidectomy c-tracheostomy

48
Direct transcervical tracheal intubation
Oral cavity Pharynx larynx

49
X-ray Anterior Lateral Chest x-ray

50
Esophageal perforation
Gastrografin swallow If g. is negative a barium swallow perform Flexible esophagoscopy 86% Contrast swallow 90% Rigid esophagoscopy Flexible+Rigid endoscopy

51
Air in the soft tissue:neck exploration
NG tube(neck level)+methylene blue
+methylene blue.")
52
Early esophageal perforation
Debridment Two layer closure Wound irrigation Adequate drainage Muscle flap Appropriate AB

53
Extensive esophageal injury
Lateral cervical esophagostomy Later definitive repair

54
Direct laryngoscopy Bronchoscopy Rigid esophagoscopy anesthesia (spine fracture)
")
55
Air in the soft tissue Hemoptysis Hematemesis Others

56
24 hours (3 times) 48-72 hours
 hours")
57
Laryngotracheal injury
Laryngeal laceration (stenosis+voice) repair early(24h) Significant glottic and supraglottic laceration+displaced cartilage surgical approximation
 repair early(24h) Significant glottic and supraglottic laceration+displaced cartilage surgical approximation.")
58
Endoscopy+CT a-Small laceration (observation)
b-Large laceration (thyrotomy or open fracture reduction)+mucosal repair
+mucosal repair.")
59
Simple tracheal laceration repair without tracheostomy
Severe tracheal injury weeks tracheostomy (below or at the site of injury)
")
Similar presentations



























 –Zone II injury –haemodynamically stable.>")


