Download presentation
Presentation is loading. Please wait.

1
The Management of Acute Respiratory Distress Syndrome 署立桃園醫院 胸腔內科 林倬睿醫師

2
Outlines Introduction Introduction Ventilator strategy Ventilator strategy Adjunctive therapy Adjunctive therapy Case demonstration Case demonstration

3
定義 Definition 急性 Acute onset 急性 Acute onset 缺氧 PaO2/FiO2 < 200 mmHg 缺氧 PaO2/FiO2 < 200 mmHg CXR: bilateral infiltrates 雙側浸潤 CXR: bilateral infiltrates 雙側浸潤 排除心因性呼吸衰竭 PAWP < 18 mmHg, no clinical evidence of LA HTN 排除心因性呼吸衰竭 PAWP < 18 mmHg, no clinical evidence of LA HTN

4
致病原因 Direct injury Direct injury Pneumonia Pneumonia Gastric aspiration Gastric aspiration Drowning Drowning Fat and amniotic fluid embolism Fat and amniotic fluid embolism Pulmonary contusion Pulmonary contusion Alveolar hemorrhage Alveolar hemorrhage Toxic inhalation Toxic inhalation Reperfusion Reperfusion Indirect injury Indirect injury Severe sepsis Severe sepsis Transfusions Transfusions Shock Shock Salicylate or narcotic overdose Salicylate or narcotic overdose Pancreatitis Pancreatitis

5
Differential Diagnosis Left ventricular failure Left ventricular failure Intravascular volume overload Intravascular volume overload Mitral stenosis Mitral stenosis Veno-occlusive disease Veno-occlusive disease Lymphangitic carcinoma Lymphangitic carcinoma Interstitial and airway diseases Interstitial and airway diseases Hypersensitivity pneumonitis Hypersensitivity pneumonitis Acute eosinophilic pneumonia Acute eosinophilic pneumonia Bronchiolitis obliterans with organising pneumonia Bronchiolitis obliterans with organising pneumonia Lancet 2007; 369:1553-65

6
Prognosis & Outcome Predictive of death: advanced age, shock, hepatic failure Predictive of death: advanced age, shock, hepatic failure Overall 28-day mortality: 20-40% Overall 28-day mortality: 20-40% Lung function: returns to normal over 6-12 months Lung function: returns to normal over 6-12 months Common complications: neuropsychiatric problems, neuromuscular weakness Common complications: neuropsychiatric problems, neuromuscular weakness Lancet 2007; 369:1553-65

7
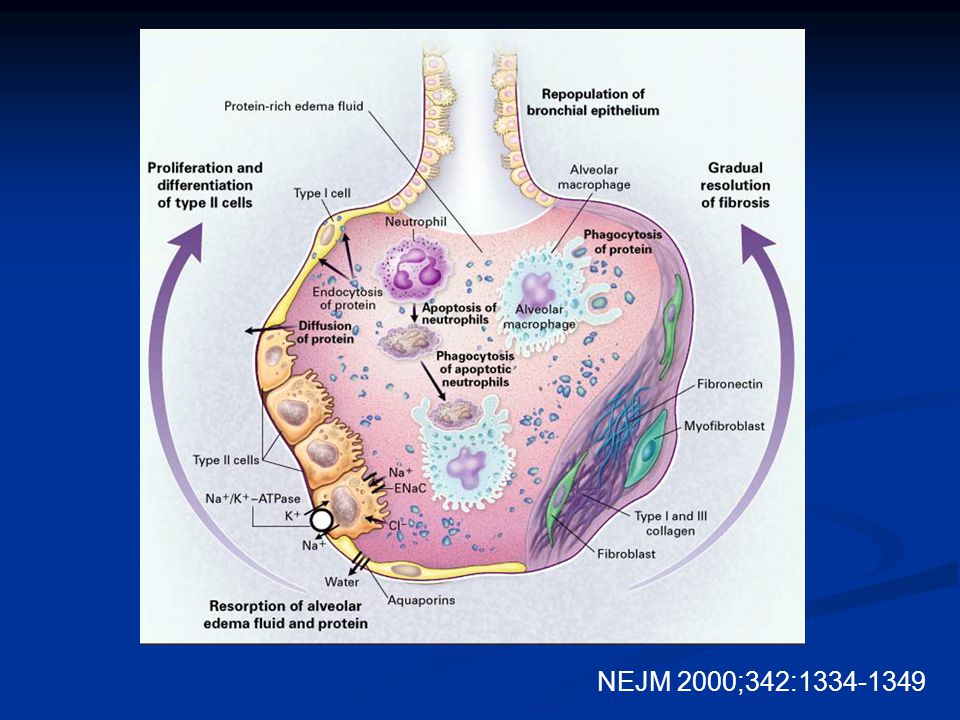
Pathophysiology Exudative phase Exudative phase Cytokines inflammation surfactant dysfunction atelectasis Cytokines inflammation surfactant dysfunction atelectasis Elastase epithelial barrier damage edema Elastase epithelial barrier damage edema Procoagulant tendency capillary thrombosis Procoagulant tendency capillary thrombosis Fibroproliferative phase Fibroproliferative phase Chronic inflammation Chronic inflammation Fibrosis Fibrosis neovascularisation neovascularisation Lancet 2007; 369:1553-65

8
NEJM 2000;342:1334-1349

11
Treatment No specific treatment No specific treatment Mainstay of treatment: supportive care Mainstay of treatment: supportive care Avoid iatrogenic complications Avoid iatrogenic complications Treat the underlying cause Treat the underlying cause Maintain adequate oxygenation Maintain adequate oxygenation

12
Supportive Care Prevention of deep vein thrombosis, gastrointestinal bleeding, and pressure ulcers Prevention of deep vein thrombosis, gastrointestinal bleeding, and pressure ulcers Semi-recumbent position Semi-recumbent position Enteral nutrition Enteral nutrition Infection control Infection control Goal-directed sedation practice Goal-directed sedation practice Glucose control Glucose control

13
Ventilator Strategy

14
Ventilator-induced Lung Injury (VILI) Barotrauma Barotrauma Volutrauma Volutrauma Atelectrauma Atelectrauma Biotrauma Biotrauma OverDistension Collapse
 Barotrauma Barotrauma Volutrauma Volutrauma Atelectrauma Atelectrauma Biotrauma Biotrauma OverDistension Collapse")
15
Volutrauma Increased alveolar wall stress (stretch) by high tidal volume Increased alveolar wall stress (stretch) by high tidal volume Parenchymal injury Parenchymal injury Gross physical disruption Gross physical disruption Stretch-responsive inflammatory pathways Stretch-responsive inflammatory pathways AJRCCM 1998; 157: 294-323
 by high tidal volume Increased alveolar wall stress (stretch) by high tidal volume Parenchymal injury Parenchymal injury Gross physical disruption Gross physical disruption Stretch-responsive inflammatory pathways Stretch-responsive inflammatory pathways AJRCCM 1998; 157:")
16
Atelectrauma Cyclic closing and reopening of alveoli Cyclic closing and reopening of alveoli Alveolar shear stress-related injury Alveolar shear stress-related injury Heterogeneous nature of lung aeration in ALI/ARDS Heterogeneous nature of lung aeration in ALI/ARDS PEEP PEEP PEEP Lung edema

17
The PEEP Effect NEJM 2006;354:1839-1841

18
Ventilator-induced Lung Injury (VILI) Upper Deflection point Lower Inflection point
 Upper Deflection point Lower Inflection point")
19
ARDS Network, 2000: Multicenter, randomized 861 patients Lung-protective ventilation Conventional ventilation Tidal Volume (ml/kg) 612 P plateau <30<50 PEEPProtocolProtocol Actual PEEP 8.19.1 Result (p<0.001) 31.0%39.8% Principle for FiO2 and PEEP Adjustment FiO20.30.40.50.60.70.80.91.0 PEEP55-88-101010-141414-1818-24 NEJM 2000; 342: 1301-1308 Lung-Protective Ventilation
 612 P plateau <30<50 PEEPProtocolProtocol Actual PEEP Result (p<0.001) 31.0%39.8% Principle for FiO2 and PEEP Adjustment FiO PEEP NEJM 2000; 342: Lung-Protective Ventilation")
20
Result: Result: Lower 22% mortality (31% vs 39.8%) Lower 22% mortality (31% vs 39.8%) Increase ventilator-free days Increase ventilator-free days Lung-Protective Ventilation NEJM 2000; 342: 1301-1308
 Lower 22% mortality (31% vs 39.8%) Increase ventilator-free days Increase ventilator-free days Lung-Protective Ventilation NEJM 2000; 342:")
21
Concerns when using lung- protective strategy… Heterogeneous distribution Heterogeneous distribution Hypercapnia Hypercapnia Auto-PEEP Auto-PEEP Sedation and paralysis Sedation and paralysis Patient-ventilator dyssynchrony Patient-ventilator dyssynchrony Increased intrathoracic pressure Increased intrathoracic pressure Maintenance of PEEP Maintenance of PEEP

22
Other Ventilator Strategies Lung recruitment maneuvers Lung recruitment maneuvers Prone positioning Prone positioning High-frequency oscillatory ventilation (HFOV) High-frequency oscillatory ventilation (HFOV)
 High-frequency oscillatory ventilation (HFOV)")
23
Lung Recruitment To open the collapsed alveoli To open the collapsed alveoli A sustained inflation of the lungs to higher airway pressure and volumes A sustained inflation of the lungs to higher airway pressure and volumes Ex.: PCV, Pi = 45 cmH2O, PEEP = 5 cmH2O, RR = 10 /min, I : E = 1:1, for 2 minutes Ex.: PCV, Pi = 45 cmH2O, PEEP = 5 cmH2O, RR = 10 /min, I : E = 1:1, for 2 minutes NEJM 2007; 354: 1775-1786

24
Lung Recruitment NEJM 2007; 354: 1775-1786

25
Lung Recruitment NEJM 2007; 354: 1775-1786

26
Potentially recruitable (PEEP 5 15 cmH2O) Potentially recruitable (PEEP 5 15 cmH2O) Increase in PaO2:FiO2 Increase in PaO2:FiO2 Decrease in PaCO2 Decrease in PaCO2 Increase in compliance Increase in compliance The effect of PEEP correlates with the percentage of potentially recruitalbe lung The effect of PEEP correlates with the percentage of potentially recruitalbe lung The percentage of recruitable lung correlates with the overall severity of lung injury The percentage of recruitable lung correlates with the overall severity of lung injury Lung Recruitment Sensitivity : 71% Specificity : 59% NEJM 2007; 354: 1775-1786
 Potentially recruitable (PEEP 5 15 cmH2O) Increase in PaO2:FiO2 Increase in PaO2:FiO2 Decrease in PaCO2 Decrease in PaCO2 Increase in compliance Increase in compliance The effect of PEEP correlates with the percentage of potentially recruitalbe lung The effect of PEEP correlates with the percentage of potentially recruitalbe lung The percentage of recruitable lung correlates with the overall severity of lung injury The percentage of recruitable lung correlates with the overall severity of lung injury Lung Recruitment Sensitivity : 71% Specificity : 59% NEJM 2007; 354:")
27
The percentage of potentially recruitable lung: The percentage of potentially recruitable lung: Extremely variable, Extremely variable, Strongly associated with the response to PEEP Strongly associated with the response to PEEP Not routinely recommended Not routinely recommended Lung Recruitment

28
Prone Position

29
Mechanisms to improve oxygenation: Mechanisms to improve oxygenation: Increase in end- expiratory lung volume Increase in end- expiratory lung volume Better ventilation- perfusion matching Better ventilation- perfusion matching More efficient drainage of secretions More efficient drainage of secretions

30
Prone Position NEJM 2001;345:568-573

31
Prone Position NEJM 2001;345:568-573

32
Improve oxygenation in about 2/3 of all treated patients Improve oxygenation in about 2/3 of all treated patients No improvement on survival, time on ventilation, or time in ICU No improvement on survival, time on ventilation, or time in ICU Might be useful to treat refractory hypoxemia Might be useful to treat refractory hypoxemia Optimum timing or duration ? Optimum timing or duration ? Routine use is not recommended Routine use is not recommended Prone Position

33
High-Frequency Oscillatory Ventilation (HFOV)
")
34
HFOV Frequency: 180-600 breaths/min (3-10Hz)
")
35
Effect of HFOV on gas exchange in ARDS patients AJRCCM 2002; 166:801-8

36
Survival difference of ARDS patients treated with HFOV or CMV 30-day: P=0.057 90-day: P=0.078 AJRCCM 2002; 166:801-8

37
HFOV HFOV Complications: Recognition of a pneumothorax Desiccation of secretions Sedation and paralysis Lack of expiratory filter Failed to show a mortality benefit Combination with other interventions ? Chest 2007; 131:1907-1916

38
Adjunctive Therapy Steroid treatment Steroid treatment Fluid management Fluid management Extracorporeal membrane oxygenation (ECMO) Extracorporeal membrane oxygenation (ECMO) Nitric oxide Nitric oxide Others Others
 Extracorporeal membrane oxygenation (ECMO) Nitric oxide Nitric oxide Others Others")
39
Steroid therapy NEJM 2006;354:1671-1684

40
Increase the number of ventilator-free and shock-free days during the first 28 day Increase the number of ventilator-free and shock-free days during the first 28 day Improve oxygenation, compliance and blood pressure Improve oxygenation, compliance and blood pressure No increase in the rate of infectious complications No increase in the rate of infectious complications Higher rate of neuromuscular weakness Higher rate of neuromuscular weakness Routine use of steroid is not supported Routine use of steroid is not supported Starting steroid more than 14 days after the onset of ARDS may increase mortality Starting steroid more than 14 days after the onset of ARDS may increase mortality Steroid therapy NEJM 2006;354:1671-1684

41
Fluid Management NEJM 2006;354:2564-2575

42
Fluid Management NEJM 2006;354:2564-2575

43
Fluid Management NEJM 2006;354:2213-24

44
Conservative strategy improves lung function and shortens the duration of ventilator use and ICU stay Conservative strategy improves lung function and shortens the duration of ventilator use and ICU stay No significant mortality benefit No significant mortality benefit The use of pulmonary artery catheter not routinely suggested The use of pulmonary artery catheter not routinely suggested Fluid Management

45
Extracorporeal Membrane Oxygenation (ECMO) No improvement on survival or time on ventilation No improvement on survival or time on ventilation Substantial risk of infection and bleeding Substantial risk of infection and bleeding Not routinely recommended Not routinely recommended
 No improvement on survival or time on ventilation No improvement on survival or time on ventilation Substantial risk of infection and bleeding Substantial risk of infection and bleeding Not routinely recommended Not routinely recommended")
46
Nitric Oxide Vasodilator Vasodilator Improve oxygenation and pulmonary vascular resistance Improve oxygenation and pulmonary vascular resistance No improvement on survival No improvement on survival Routine use is not recommended Routine use is not recommended

47
Unproven Treatments Ketoconazole Ketoconazole Pentoxyfilline and lisofylline Pentoxyfilline and lisofylline Nutritional modification Nutritional modification Antioxidants Antioxidants Neutrophil elastase inhibition Neutrophil elastase inhibition Surfactant Surfactant Liquid ventilation Liquid ventilation Lancet 2007; 369:1553-65

48
Conclusions The only treatment that shows mortality benefit: The only treatment that shows mortality benefit: lung-protective ventilation strategy lung-protective ventilation strategy Low tidal volume (6ml/Kg), high PEEP, adequate Pplat (<30 cmH2O) Low tidal volume (6ml/Kg), high PEEP, adequate Pplat (<30 cmH2O) Modalities to improve oxygenation: Modalities to improve oxygenation: Prone position, steroid, fluid treatment, steroid, HFOV, NO Prone position, steroid, fluid treatment, steroid, HFOV, NO Combining other treatments: Combining other treatments: Activated protein C, antibiotics, EGDT…etc Activated protein C, antibiotics, EGDT…etc
, high PEEP, adequate Pplat (<30 cmH2O) Low tidal volume (6ml/Kg), high PEEP, adequate Pplat (<30 cmH2O) Modalities to improve oxygenation: Modalities to improve oxygenation: Prone position, steroid, fluid treatment, steroid, HFOV, NO Prone position, steroid, fluid treatment, steroid, HFOV, NO Combining other treatments: Combining other treatments: Activated protein C, antibiotics, EGDT…etc Activated protein C, antibiotics, EGDT…etc")
Similar presentations






>")





 Dr. Meg-angela Christi Amores.>")





 Acute Respiratory Distress Syndrome (ARDS) Pathophysiology in ARDS Therapy.>")

