Download presentation
Presentation is loading. Please wait.

1
Joint Hospital Surgical Grand Round KL FOK NDH/AHNH Department of Surgery

2
Neoadjuvant therapy for esophageal carcinoma

3
Definition Neoadjuvant- a term used to describe preliminary cancer therapy (usually chemotherapy or radiation therapy) that precedes a necessary second modality treatment. ( Dorland ’ s Medical Dictionary 28 th edition p1106) Neoadjuvant- a term used to describe preliminary cancer therapy (usually chemotherapy or radiation therapy) that precedes a necessary second modality treatment. ( Dorland ’ s Medical Dictionary 28 th edition p1106)
 Neoadjuvant- a term used to describe preliminary cancer therapy (usually chemotherapy or radiation therapy) that precedes a necessary second modality treatment. ( Dorland ’ s Medical Dictionary 28 th edition p1106).")
4
The Role of Surgery No doubt that surgery remains the mainstay for curative treatment for carcinoma of esophagus No doubt that surgery remains the mainstay for curative treatment for carcinoma of esophagus Good at local control Good at local control –T1 tumor without lymph node after curative resection (confined to submucosa) survival up to 80% –T1/2 N0 :40% 5 yr survival –T3N0: 25% 5 yr survival
 survival up to 80% –T1/2 N0 :40% 5 yr survival –T3N0: 25% 5 yr survival")
5
Limitation of Surgery Only 10 -20% of cases are operable Only 10 -20% of cases are operable Good at local control/ ??effectiveness in regional nodal control Good at local control/ ??effectiveness in regional nodal control

6
Limitation of surgery Once Lymph node involved 13%-15% survival only (varied with different specialist centers) Once Lymph node involved 13%-15% survival only (varied with different specialist centers) High chance of LN +ve 40-50% High chance of LN +ve 40-50% –T1 mucosal- 5% nodal met. –T1 submucosa- 25% nodal met.

7
Rationale for multi-modal therapy Local : downsizing effect ; so as to increase resectability Local : downsizing effect ; so as to increase resectability Regional: Decrease LN involvement which is an imminent poor prognostic factor Regional: Decrease LN involvement which is an imminent poor prognostic factor Systemic: Deal with micrometastasis Systemic: Deal with micrometastasis Synergistic effect of chemo& RT Synergistic effect of chemo& RT

8
Why neoadjuvant? Neoadjuvant versus Adjuvant Neoadjuvant versus Adjuvant –Better tolerance before major upper GI surgery (88% vs. 55 %) –Downstaging of tumor i.e. allowing surgery –May allow more conservative local control –Earliest means to tackle systemic spread
 –Downstaging of tumor i.e. allowing surgery –May allow more conservative local control –Earliest means to tackle systemic spread.")
9
Disadvantages of neoadjuvant? Neoadjuvant versus Adjuvant Neoadjuvant versus Adjuvant –Over-treat / unnecessary exposure of systemic toxicity in patient with early tumor –Delay surgical treatment –?increase surgical mortality/morbidity

10
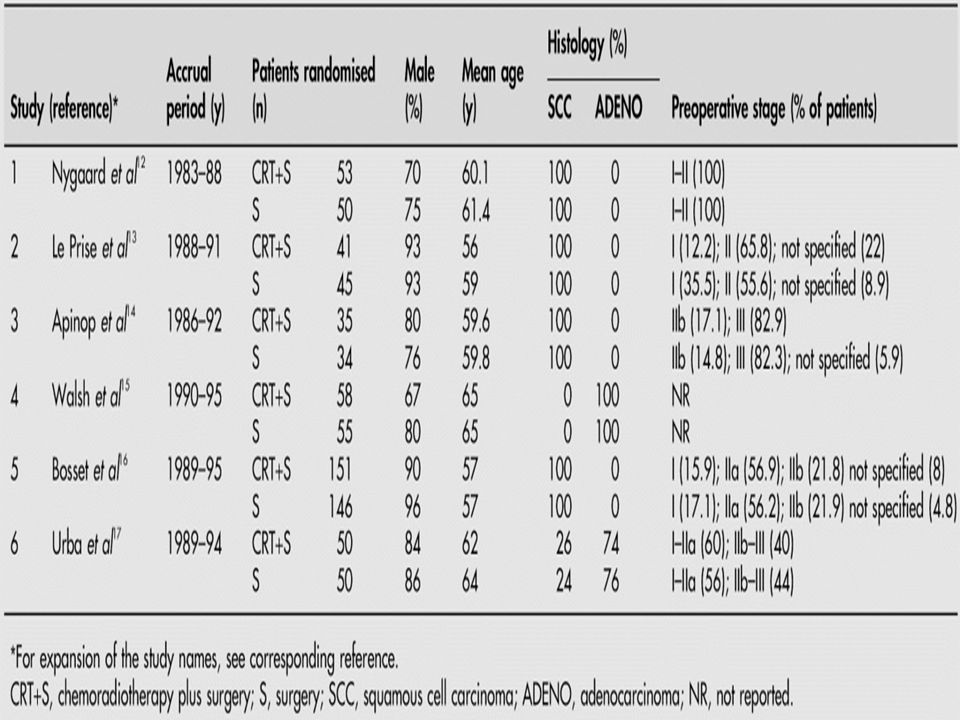
Neoadjuvant therapy- questions to answer ?Survival benefit/disease-free survival ?Survival benefit/disease-free survival ?Increase resectability/?downsizing ?Increase resectability/?downsizing ?Decrease lymph-node met. ?Decrease lymph-node met. AdenoCA vs. SCC AdenoCA vs. SCC Early stage/late stage Early stage/late stage

11
Radiotherapy Most of the study do not show any benefit in terms of survival/resectability/ LN involvement Most of the study do not show any benefit in terms of survival/resectability/ LN involvement –Launois B et al. (81)N=124 –Gignoux et al (87) N= 229 –Huang GJ et al (87) N=360
N=124 –Gignoux et al (87) N= 229 –Huang GJ et al (87) N=360.")
12
Chemotherapy UK MRC study +ve trial N= 802 UK MRC study +ve trial N= 802 –R0( 60% vs. 54%) –Median survival 16.8 vs. 14.9 months P=0.004 –2 yrs survival 43% vs. 34% US 0113 – ve trial (+ve survival benefit in responder) N= 450 US 0113 – ve trial (+ve survival benefit in responder) N= 450 Conflicting results:? due to delay in surgery/toxicity for non – responder Conflicting results:? due to delay in surgery/toxicity for non – responder
 –Median survival 16.8 vs months P=0.004 –2 yrs survival 43% vs. 34% US 0113 – ve trial (+ve survival benefit in responder) N= 450 US 0113 – ve trial (+ve survival benefit in responder) N= 450 Conflicting results:. due to delay in surgery/toxicity for non – responder Conflicting results:. due to delay in surgery/toxicity for non – responder.")
13
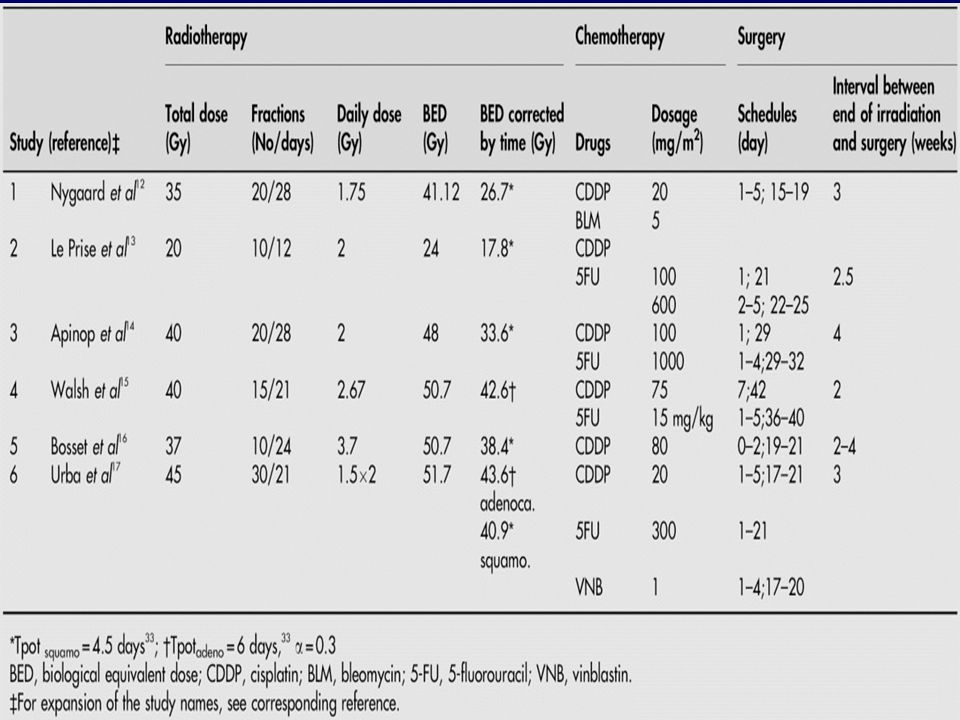
Chemoradiotherapy Chemotherapy serve as radiosensitiser Chemotherapy serve as radiosensitiser Chemotherapy can reduce or eliminate micrometastasis Chemotherapy can reduce or eliminate micrometastasis

15
Meta-analysis of RCT on overall 3 yrs survival

16
Meta-analysis of RCT on downstaging effect

17
Meta-analysis of RCT on postop. mortality

18
Summary Pros: Neoadjuvant chemoradiotherapy downstaging the tumor Neoadjuvant chemoradiotherapy downstaging the tumor Increase resectability Increase resectability Longer disease free survival Longer disease free survival Much improved median survival in complete responder (up to 50 months median survival; 3 yr survival 64%) Much improved median survival in complete responder (up to 50 months median survival; 3 yr survival 64%)
 Much improved median survival in complete responder (up to 50 months median survival; 3 yr survival 64%)")
19
Summary CONS no clear cut advantages in overall survival associated with higher operative mortality/morbidity ?over-treating the non-responder (up to 50-60%)
")
20
Unanswered question ? Any indicator for potential benefit of preop. chemoRT ? Any indicator for potential benefit of preop. chemoRT –?stage specific –?Histological type –?Genomic related

21
Perspective Non responder can up to 60-70 % Non responder can up to 60-70 % –Delay in operation –Higher operative mortality –Affect the overall survival of combined - modality treatment ?Response prediction ?Response prediction

22
Response prediction ?any significant prognostic and predictive marker ?any significant prognostic and predictive marker –Measuring of target molecule for which the chemo-agent works on eg: tumor thymidylate synthase, thymidine phosphorylase /chromosomal instabilty/p53 expression –Measuring the metabolic response: early interval PET scan

Similar presentations











 Karl Podratz MD PhD FACS.>")







