Download presentation
Presentation is loading. Please wait.

1
Gatmaitan, Raymond Vincent Golpeo, Kirsten C.
BLEEDING Gatmaitan, Raymond Vincent Golpeo, Kirsten C.

2
Case & Objectives A 2 year old boy was brought for check up due to multiple hematoma over both legs. Discuss bleeding tendencies based on their usual presentation Discuss bleeding tendencies based on the following parameter: PT, PTT Platelet BT, CT Discuss and correlate normal hemostasis with the laboratory findings

3
HEMOSTASIS – an active process that clots blood in areas of blood vessel injury, yet simultaneously limits the clot size only to the areas of injury. Primary Hemostasis – process of platelet plug formation at site of injury. Occurs within seconds of injury. Stops blood loss from the capillaries, small arterioles and venules 3 Critical events for effective primary hemostasis Platelet adhesion Granule release Platelet aggregation Secondary Hemostasis – Reactions of the plasma coagulation system resulting to fibrin formation. Occurs within several minutes for completion. Important in larger vessels.

7
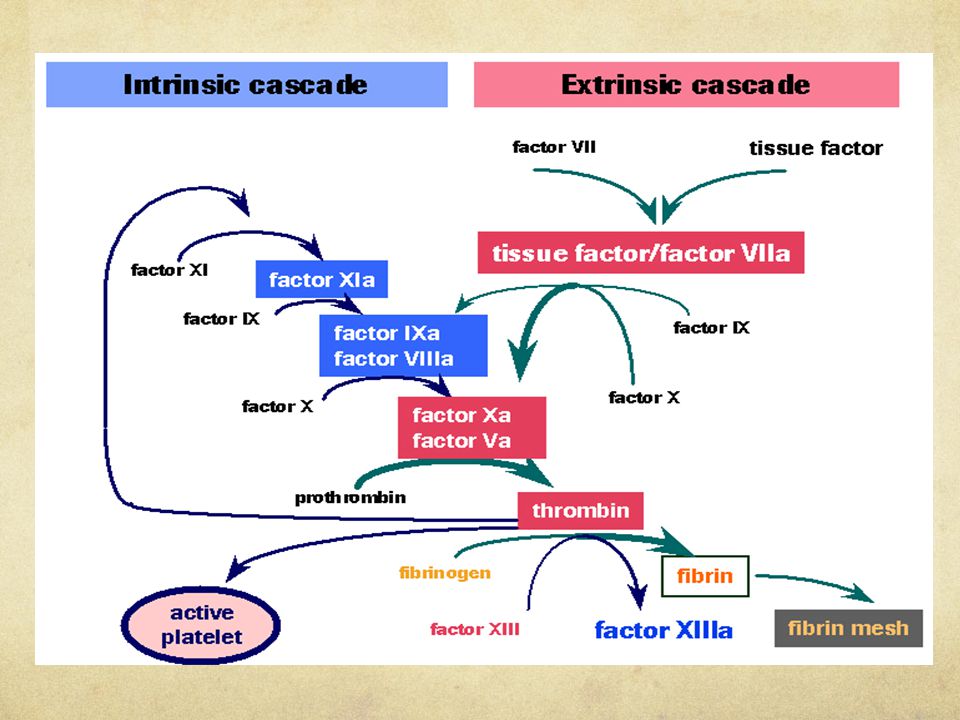
Coagulation Cascade

8
Presentation of Bleeding Disorders
In physical examination, it should focus on whether bleeding symptoms are primarily associated with mucous membranes or skin or the muscles and joints. Mucocutaneous bleeding (epistaxis, menorrhagia, hematuria, GI bleeding), petechiae on the skin and mucous membranes, and small ecchymotic lesions of the skin. DEFECTS in PLATELET or BLOOD VESSEL WALL INTERACTION Deep Bleeding into muscles and joints with much more extensive ecchymoses and hematoma formation. Hamarthrosis (Hemophilia A). CLOTTING FACTOR DEFECIENCY Some individuals with mild defects or deficiencies may have no abnormal findings on PE. Also, individuals with collagen matrix and vessel wall may have loose joints and lax skin associated with easy bruising (Ehlers-Danlos Syndrome)
, petechiae on the skin and mucous membranes, and small ecchymotic lesions of the skin. DEFECTS in PLATELET or BLOOD VESSEL WALL INTERACTION. Deep Bleeding into muscles and joints with much more extensive ecchymoses and hematoma formation. Hamarthrosis (Hemophilia A). CLOTTING FACTOR DEFECIENCY. Some individuals with mild defects or deficiencies may have no abnormal findings on PE. Also, individuals with collagen matrix and vessel wall may have loose joints and lax skin associated with easy bruising (Ehlers-Danlos Syndrome)")
9
Von Willebrand Disease (VWD) (platelet-type vWD)
Autosomal dominant Gain of function of platelet GPIb-IX-V complex – resembles vWD type 2B (adhesion disorder) Epistaxis, ecchymoses, menorrhagia, gingival hemorrhage example
 Epistaxis, ecchymoses, menorrhagia, gingival hemorrhage. example.")
10
Ecchymoses An ecchymosis is a collection of blood greater than 1 cM in sizeoutside the vascular tree, and within tissue. As a result of trauma, blood escapes from the vascular tree and accumulates in the tissues. Histologically, the lesion is characterized by the presence of red blood cells lying outside of capillaries. With time there is infiltration by inflammatory cells, primarily macrophages in which hemosiderin deposition can be seen several weeks to months after initial lesion.

11
Petichaie Petechiae are pinpoint, round spots that appear on the skin as a result of bleeding under the skin. The bleeding causes the petechiae to appear red, brown or purple. Petechiae may look like a rash. Usually flat to the touch, petechiae don't lose color (blanch) when you press on them. Petechiae may indicate a number of conditions that can be serious.
 when you press on them. Petechiae may indicate a number of conditions that can be serious.")
12
Hamarthrosis Hemophilic arthropathy is a rare joint-destroying disorder that is more prevalent before adulthood. It is usually seen in hemophilia A which is a sex-linked deficiency or abnormality of a plasma protein called factor VIII (FVIII) found in 1 of 5000 male births. Eventually osseous irregularity and erosion develop, accompanied by subchondral cysts. Synovial effusions are common and may appear radiodense due to hemosiderin deposition. An important diagnostic clue to hemophilic arthropathy during early phase is the preservation of joint space. Radiographically, in adolescents, the hyperemic joint may lead to localized, accelerated growth and limb-length discrepancies. Eventually osseous irregularity and erosion develop, accompanied by subchondral cysts. An important diagnostic clue to hemophilic arthropathy during this phase is the preservation of joint space. As osseous erosions continue, however, joint space narrowing is seen, associated with progressive, symmetric cartilaginous destruction. Eventually, complete obliteration of the joint space will occur and secondary degenerative signs, including osteophytes and eburnation, develop. With chronic disease, muscle imbalances and joint contractures may develop.
 found in 1 of 5000 male births. Eventually osseous irregularity and erosion develop, accompanied by subchondral cysts. Synovial effusions are common and may appear radiodense due to hemosiderin deposition. An important diagnostic clue to hemophilic arthropathy during early phase is the preservation of joint space. Radiographically, in adolescents, the hyperemic joint may lead to localized, accelerated growth and limb-length discrepancies. Eventually osseous irregularity and erosion develop, accompanied by subchondral cysts. An important diagnostic clue to hemophilic arthropathy during this phase is the preservation of joint space. As osseous erosions continue, however, joint space narrowing is seen, associated with progressive, symmetric cartilaginous destruction. Eventually, complete obliteration of the joint space will occur and secondary degenerative signs, including osteophytes and eburnation, develop. With chronic disease, muscle imbalances and joint contractures may develop.")
13
Laboratory Parameters
Platelet Count – Thrombocytopenia is the most common acquired cause of a bleeding disorders in children. Normal levels: X 109/L Bleeding Time – test for adequacy of primary hemostasis or platelet function. Prothrombin Time – assess the clotting ability of blood and assess the extrinsic and common pathway. Partial Thromboplastin Time – assess the coagulation proteins of the intrinsic system and the common pathway Bleeding Time - recommended criteria prior to testing 1. platelet count - >75,000/mm3 2. only 1 BT/24hrs unless patient has received therapy ex. platelet infusion 3. D/C heparin 6 hrs prior to testing Bleeding Time: Reference range: 1-3 mins. (Duke method) 2-7 mins (template Ivy method) usually significantly prolonged in the case of congenital or acquired platelet defects. Prolongation of BT seen in the following disorders: - thrombasthenia - Platelet count <75,000 - Bernard-Soulier - Von Willebrand ds. - Storage pool disease - uremia - aspirin ingestion liver failure PT - specific/only lab test to measure effectiveness of patients receiving Warfarin (Coumadin) therapy evaluates the presence of factors VII, V, and X, prothrombin, and fibrinogen. Reference range: seconds prolonged prothrombin time indicates a deficiency in above mentioned factors. Example of conditions with prolonged PT: vitamin K deficiency (vitamin K is a co-factor in the synthesis of functional factors II (prothrombin), VII, IX and X) liver disease (the liver is the site of synthesis of the plasma protein factors) patients receiving a vitamin K-competing coumarin drug such as warfarin PTT - Reference range: sec. Prolonged APTT seen in: deficiencies of either XII, XI, X, IX, VIII, V, II and fibrinogen (deficient factor has to be less than 20-40% of normal )
 2-7 mins (template Ivy method) usually significantly prolonged in the case of congenital or acquired platelet defects. Prolongation of BT seen in the following disorders: - thrombasthenia - Platelet count <75, Bernard-Soulier - Von Willebrand ds. - Storage pool disease - uremia. - aspirin ingestion - liver failure. PT - specific/only lab test to measure effectiveness of patients receiving. Warfarin (Coumadin) therapy. evaluates the presence of factors VII, V, and X, prothrombin, and fibrinogen. Reference range: seconds. prolonged prothrombin time indicates a deficiency in above mentioned factors. Example of conditions with prolonged PT: vitamin K deficiency (vitamin K is a co-factor in the synthesis of functional factors II (prothrombin), VII, IX and X) liver disease (the liver is the site of synthesis of the plasma protein factors) patients receiving a vitamin K-competing coumarin drug such as warfarin. PTT - Reference range: sec. Prolonged APTT seen in: deficiencies of either XII, XI, X, IX, VIII, V, II and fibrinogen (deficient factor has to be less than 20-40% of normal )")
14
PLATELET COUNT EFFECT >100,000/uL (100,000 – 140,000) Normal Bleeding Time 50, ,000/ uL Mild Prolonged Bleeding time <50, 000/uL Bleeding after minor trauma <20,000/uL Spontaneous bleeding

15
Laboratories Platelet BT/CT PT PTT Henoch Schonlien Purpura Normal
Hemolytic Uremic Syndrome Thrombotic Thrombocytopenic Purpura Decreased Idiopathic (immune) Thrombocytopenic Purpura Von Willebrand’s Disease Prolonged (poor platelet quality) Prolonged CLINICAL MANIFESTATIONS HSP – clinical diagnosis. Clinical triad: symmetric pupuric rashes, polyarthralgia and abdominal pain. May or may not have hematuria, (focal glomerulonephritis) HUS – RBC morphology (+) helmet cells, spherocytes, schistocytes and burr cells (peripheral smear) Thrombocytopenia- reduction of platelet count to <150 x 10 to the 9th/L. TTP – Pentad: fever, microangiopathic hemolytic anemia, thrombocytopenia, abnormal renal function and CNS shanges. (Peripheral Blood smear: schistocytes, spherocytes and helmet cells. Drug induced thrombocytopenia – valproic acid, phenytoin, sulfonamides, trimethoprim-sulfamethoxazole, seldom heparin
 Thrombocytopenic Purpura. Von Willebrand’s Disease. Prolonged (poor platelet quality) Prolonged. CLINICAL MANIFESTATIONS. HSP – clinical diagnosis. Clinical triad: symmetric pupuric rashes, polyarthralgia and abdominal pain. May or may not have hematuria, (focal glomerulonephritis) HUS – RBC morphology (+) helmet cells, spherocytes, schistocytes and burr cells (peripheral smear) Thrombocytopenia- reduction of platelet count to <150 x 10 to the 9th/L. TTP – Pentad: fever, microangiopathic hemolytic anemia, thrombocytopenia, abnormal renal function and CNS shanges. (Peripheral Blood smear: schistocytes, spherocytes and helmet cells. Drug induced thrombocytopenia – valproic acid, phenytoin, sulfonamides, trimethoprim-sulfamethoxazole, seldom heparin.")
16
Laboratories Platelet BT/CT PT PTT Factor VIII Deficiency Normal
Prolonged Factor IX Deficiency Vitamin K deficiency Increased Hemophilia A – decrease in factor VIII assay Hemophilia B – Decrease in factor IX assay

17
Peripheral Blood Smear
Abnormal RBC Morphology Hemolytic Uremic Syndrome (+) Helmet cells, spherocytes, schistocytes, and burr cells DIC (+) Schictocytes TTP (+) spherocytes, schistocytes, and burr cells
 Helmet cells, spherocytes, schistocytes, and burr cells. DIC. (+) Schictocytes. TTP. (+) spherocytes, schistocytes, and burr cells.")
18
Schistocytes - There are numerous fragmented RBC's seen here
Schistocytes - There are numerous fragmented RBC's seen here. Some of the irregular shapes appear as "helmet" cells. Such fragmented RBC's are known as "schistocytes" and they are indicative of a microangiopathic hemolytic anemia (MAHA) or other cause for intravascular hemolysis. There are only a few mechanisms by which erythrocytes become fragmented. The primary mechanism is via shearing of erythrocytes by fibrin strands (Fig. 3). This occurs when erythrocytes rapidly pass through microvasculature that is lined or meshed with fibrin strands. Endothelial lesions result in platelet aggregation, which subsequently leads to thrombosis and fragmentation of red blood cells.8,9 Diseases that are characterized by turbulent blood flow also form schistocytes. Spherocytes - Spherocytes (black arrow) are red blood cells which are smaller and denser than their normal counterparts. Their increased density stems from the loss of the red blood cell's characteristic biconcave shape. Hence, the observation of spherocytes in a blood smear is most often linked to immune-mediated hemolytic anemia. It is important to note that spherocytes may be difficult to identify.
 or other cause for intravascular hemolysis. There are only a few mechanisms by which erythrocytes become fragmented. The primary mechanism is via shearing of erythrocytes by fibrin strands (Fig. 3). This occurs when erythrocytes rapidly pass through microvasculature that is lined or meshed with fibrin strands. Endothelial lesions result in platelet aggregation, which subsequently leads to thrombosis and fragmentation of red blood cells.8,9 Diseases that are characterized by turbulent blood flow also form schistocytes. Spherocytes - Spherocytes (black arrow) are red blood cells which are smaller and denser than their normal counterparts. Their increased density stems from the loss of the red blood cell s characteristic biconcave shape. Hence, the observation of spherocytes in a blood smear is most often linked to immune-mediated hemolytic anemia. It is important to note that spherocytes may be difficult to identify.")
19
Giant Platelets Immune thrombocytopenic purpura (ITP) is one of the most common autoimmune disorders. ITP is caused by autoantibodies to platelets. The antigenic target in most patients appears to be the platelet GP IIb/IIIa complex. Platelets with antibodies on their surface are trapped in the spleen, where they are efficiently removed by splenic macrophages The peripheral smear shows a decreased number of platelets. Often, the smear shows giant platelets, which is a reflection of increased thrombopoietin-induced stimulation of the bone marrow
 is one of the most common autoimmune disorders. ITP is caused by autoantibodies to platelets. The antigenic target in most patients appears to be the platelet GP IIb/IIIa complex. Platelets with antibodies on their surface are trapped in the spleen, where they are efficiently removed by splenic macrophages. The peripheral smear shows a decreased number of platelets. Often, the smear shows giant platelets, which is a reflection of increased thrombopoietin-induced stimulation of the bone marrow.")
20
Developmental Hemostasis
Newborn infant has a reduced levels of most procoagulants and antcoagulants. There is more marked abnormality in the preterm infant. During gestation, there is no progressive maturation and increase of the clotting factors synthesized by the liver. The extremely premature infant will have prolonged PT and PTT as well as a marked reduction in anticoagulant proteins (protein C and S) Levels of fibrinogen, factor V, and VIII, VWF, and platelets are near- normal throughout the later stages of gestation. Protein C and S are physiologically reduced, the normal factors V and VIII are not balanced with their regulatory proteins. The net effect is that newborns (especially premature infants) are at increased risk for complications of bleeding, clotting, or both.
 Levels of fibrinogen, factor V, and VIII, VWF, and platelets are near- normal throughout the later stages of gestation. Protein C and S are physiologically reduced, the normal factors V and VIII are not balanced with their regulatory proteins. The net effect is that newborns (especially premature infants) are at increased risk for complications of bleeding, clotting, or both.")
21
Normal Values 30-36 weeks of Gestation Full Term 1-5 years old
PT(sec) 130 ( ) 13.0( ) 11( ) 11.1( ) PTT(sec) 53.6( ) 42.9( ) 30(24-36) 31(26-36) BT(min) 6(2.5-10) 7(2.5-13) Platelet X 109/L Reference Values for coagulation test in healthy children –Nelson’s
 130 ( ) 13.0( ) 11( ) 11.1( ) PTT(sec) 53.6( ) 42.9( ) 30(24-36) 31(26-36) BT(min) 6(2.5-10) 7(2.5-13) Platelet X 109/L. Reference Values for coagulation test in healthy children –Nelson’s.")
23
Correlation of Normal Hemostasis to Lab findings
RVIN…. Help…

24
Thank you!

Similar presentations


















i.>")



