Download presentation
Presentation is loading. Please wait.

1
IMMUNE THROMBOCYTOPENIA Cathy Payne MSN, ACNP-BC Hematology/Oncology Nurse Practitioner Ironwood Cancer and Research Centers

2
OBJECTIVES Define ITP Terminology Epidemiology Mortality/Morbidity Pathophysiology Diagnosis ASH guidelines/Management

3
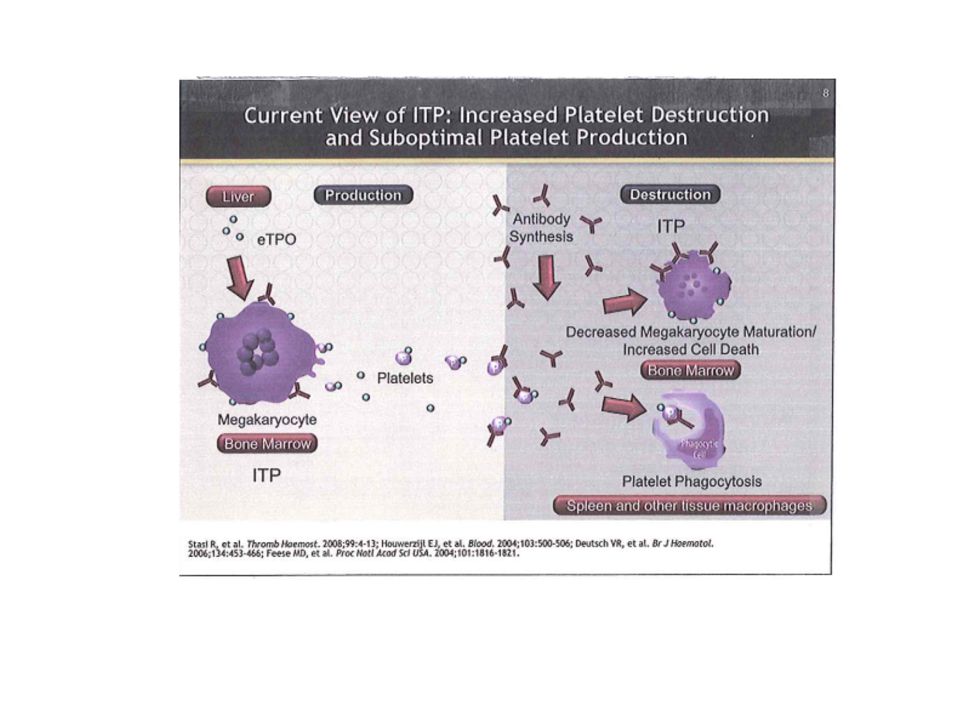
Immune Thrombocytopenia ITP is an autoimmune-mediated hematologic disorder, in which the patients immune system produces antibodies directed against platelet antigens resulting in immune mediated platelet destruction and/or suppression of platelet production Cines, D.B., Blanchet, VS, (2002) Immune thrombocytopenia purpura.
 Immune thrombocytopenia purpura.")
4
PATHOPHYSIOLOGY reduced platelet lifespan due to antibody mediated destruction, as well as impaired platelet production specific IgG autoantibodies produced by the patient’s B cells most often are directed against platelet membrane glycoproteins like GPIIb/IIIa inciting events- viral infections and systemic conditions, malignancies

7
TERMINOLOGY Diagnostic platelet count <100,000 Primary vs secondary Duration Severity Refractory ITP Response to treatment

8
EPIDEMIOLOGY 1 to 3 per 100,000 adults Young women Incidence increases with age with a slight male predominance

9
MORBIDITY/MORTALITY Most patients will have good outcomes with infrequent hospital admissions and no excess mortality compared with the general population patients with persistent severe thrombocytopenia not responding to therapy within first 2 years have considerable M/M Bleeding/infections cause of death

10
DIAGNOSING ITP HISTORY ethanol history liver disease drug history bleeding/bruising family history risk factors for HIV or hepatitis C and or B symptoms Symptoms of MDS autoimmune disorders recent viral infection history of transfusions

11
PHYSICAL EXAM petechiae purpura conjunctival bleeding retinal hemorrhages lesions on mucosal membranes enlarged liver or spleen lymph nodes sighs of sepsis, DIC or other severe systemic abnormalities pregnancy

12
COMPLETE BLOOD COUNT Isolated thrombocytopenia, plt count < 100,000 anemia only if significant bleeding otherwise normal red cell indices, WBC count and differential, normal coagulation parameters peripheral blood smear- schistocytes

13
LAB TESTS HIV and Hep C coagulation studies Helicobacter pylori thyroid funtion rheumatological studies Vitamin B12 and folate levels anti-platelet antibody testing- NO

14
BONE MARROW EXAM not always needed, but do if the etiology of thrombocytopenia is unclear any abnormality with History/Physical, blood smear or blood indices yes for those older than 60 years

15
DIFFERENTIAL DIAGNOSIS drug induced infections liver disease and hypersplenism microangiopathic processes MDS and other bone marrow disorders vasculitic purpura

16
ASH GUIDELINES/MANAGEMENT OF ITP INITIAL MANAGEMENT consider treatment for patients with a platelet count <30,000 longer courses of corticosteroids are preferred over shorter courses of corticosteriods or IVIG IVIG may be used in conjunction with corticosteriods if a more rapid increase in platelet count is required either IVIG (1g.kg for one dose, repeated as necessary) or anti-D (in appropriate patients) may be used as a first line treatment if corticosteriods are contraindicated
 or anti-D (in appropriate patients) may be used as a first line treatment if corticosteriods are contraindicated")
17
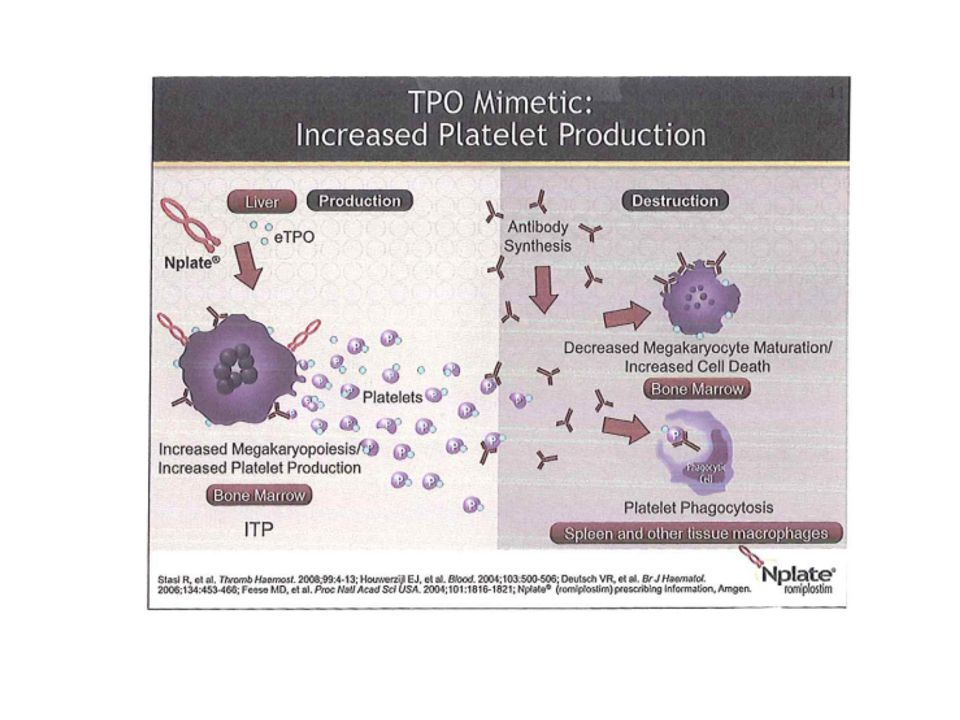
ASH GUIDELINES FOR SENCOND LINE THERAPY splenectomy rituximab thrombopoientin receptor agonist high dose dexamethasone immunosuppression

Similar presentations


















 Thrombocytopenic Purpura AM Report 5/25/2010.>")


