Download presentation
Presentation is loading. Please wait.

1
Idiopathic Thrombocytopenic Purpura
Dr. Padma Poddutoori, PGY3 , I.M Dr. Sohail Chaudhry, Attending physician, Hemeoncology

2
Definition ITP is an immune-mediated disorder of platelet destruction caused by antibodies. These antibodies react with platelet glycoproteins, particularly glycoprotein IIb-IIIa, the platelet fibrinogen receptor and glycoprotein Ib.

3
Classification of ITP Acute and Chronic Primary and secondary
Acute ITP is common in children following viral exanthems or upper respiratory infections.60% recover in 4-6 wks and >90% in 3-6 m.caused by immune complexes that contain viral antigens that bind to pl. Fc receptors or by Ab produced against viral Ag that cross react with pl. Chronic : indolent form of thrombocytopenia that persists for many years Secondary: SLE, HIV, Hep C, immunodeficieny or lymphoproliferative disorders[B cell malignancies-CLL and large granular leukemias]

4
Who develops ITP? Typically a woman between 18 and 40 yrs.
Female to male incidence: 3:1 Gender disparity disappears largely in elderly

5
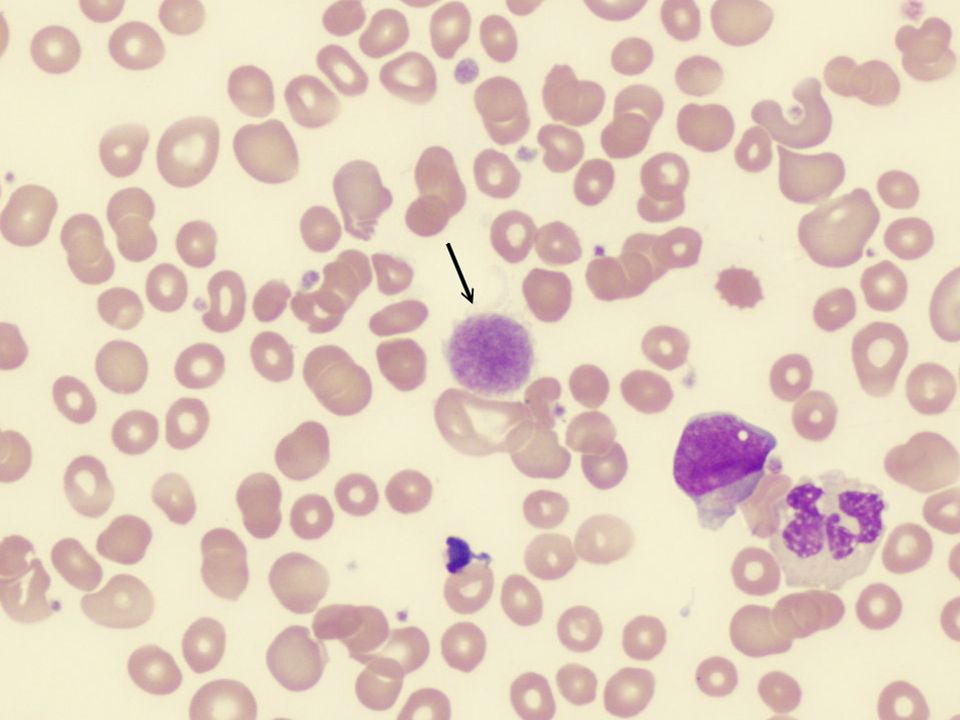
How do we diagnose ITP ITP is a diagnosis of exclusion
Isolated thrombocytopenia in an otherwise healthy individual, with an otherwise unremarkable peripheral smear, with/without physical findings of evidence of bleeding. What is the best diagnostic test? Response to treatment especially to IVIG or IV anti-D, even if transient is the single best diagnostic test

6
Diagnosis contd….. What is the role of antiplatelet antibodies in the diagnosis of ITP? We do not rely on measuring anti platelet antibodies to make or exclude a diagnosis of ITP They are also seen in % of pts with certain causes of “non immune” thrombocytopenias[e.g Chr. Liver dz, MDS] These assays lack sensitivity to exclude a diagnosis of ITP

7
When do we perform bone marrow examination
Over 60 yrs of age[as the incidence of MDS is significant] In those who do not show a robust response[>50,000] to treatment Often prior to splenectomy When more than one cell lines are involved

8
What is the role of H.pylori in ITP?
Remissions induced by eradication of asymptomatic H.pylori were reported in studies from Japan and Italy, but is not our experience Consider testing in those with GI symptoms and in chronic cases

9
Who do we treat? Our usual practice is to maintain a somewhat higher platelet count of 30,000. Major bleeding including spontaneous ICH occurs predominantly in pts with platelet counts<20,000, generally <10,000 The risk of bleeding depends on the age of individual, comorbidities and the medications

10
Treatment Emergency- IV methylprednisolone [1 gm/day for 1-3 days]
IVIG [1 gm/kg/day for 2-3 days] +/-IV anti-D [75mcg/kg] +/-IV Vincristine[1-2 mg] +/-Platelet transfusion +/-Factor VIIa[if unresponsive to other modalities of treatment, if immediate response is needed, e.g. ICH]
![Treatment Emergency- IV methylprednisolone [1 gm/day for 1-3 days]](http://slideplayer.com/slide/2993955/11/images/10/Treatment+Emergency-+IV+methylprednisolone+%5B1+gm%2Fday+for+1-3+days%5D.jpg "IVIG [1 gm/kg/day for 2-3 days] +/-IV anti-D [75mcg/kg] +/-IV Vincristine[1-2 mg] +/-Platelet transfusion. +/-Factor VIIa[if unresponsive to other modalities of treatment, if immediate response is needed, e.g. ICH]")
11
Treatment contd….. Initial treatment for non emergent indications
Prednisone 1 mg/kg/day +/- IV anti-D[50-75mcg/kg] +/- IVIG[1 gm/kg/day x 2-3 days as needed] OR Dexamethasone[40 mg/day po x 4 days/month]

12
Treatment contd….. Persistent ITP: Low dose prednisone[<10 mg/day]
IV anti-D[50-75mcg/kg/dose] IV anti-CD20[Rituximab] [375mg/m2 q week x 4] Danazol [10-15 mg/kg/day po] Treatment for 3-12 months from diagnosis
![Treatment contd….. Persistent ITP: Low dose prednisone[<10 mg/day]](http://slideplayer.com/slide/2993955/11/images/12/Treatment+contd%E2%80%A6..+Persistent+ITP%3A+Low+dose+prednisone%5B%3C10+mg%2Fday%5D.jpg "IV anti-D[50-75mcg/kg/dose] IV anti-CD20[Rituximab] [375mg/m2 q week x 4] Danazol [10-15 mg/kg/day po] Treatment for 3-12 months from diagnosis.")
13
Splenectomy Indications:
Whose disease does not abate by 1 yr after diagnosis Who do not show a durable response to therapy Who are intolerant to therapy We use IVIG, IV anti-D or pulse doses of corticosteroids to boost the pl count prior to surgery Immunize pts 2 wks prior to surgery with polyvalent pneumococcal, H.influenzae type b and meningococcus 85% attain hemostatic response after splenectomy and 2/3rds achieve durable response.

14
Chronic ITP Pl count<20-30,000 First line therapies:
IV anti-CD20[Rituximab] Or Danazol +azathioprine or mycophenolate mofetil Prednisone or IVIG prn Second line therapy: Cyclophosphamide or cyclosporine Third line therapy: Combination chemotherapy Stem cell transplantation

15
Newer therapies Thrombopoeitin receptor agonist- Eltrombopag
It is an oral small-molecule non peptide platelet growth factor It increased pl counts[to 50,000 or more] in a dose dependant manner[50 or 75 mg] in pts with relapsed or refractory ITP with pl count <30,000 This was attained in 80% of pts within 2 wks

16
Newer therapies contd…..
Romiplostim[Nplate] A thrombopoeitin receptor agonist Should only be used in pt s with chronic ITP with insufficient response to steroids, IG or splenectomy and in pts whose degree of thrombocytopenia and clinical condition increase the risk for bleeding Dosage: initial dose of 1 mcg/kg s.q q wkly[max of 10 mcg/kg], increase by 1 mcg/kg/wk as needed to achieve and maintain pl count >50,000.stop after 4 wks if no improvement in pl counts or if pl count >400 Adverse reactions:dizziness, insomnia, arthralgia, myalgia, pain in extremity, abdomen, shoulder,dyspepsia and paresthesia Precautions: increases the risk for reticulin deposition in bone marrow-may result in marrow fibrosis with cytopenias; may increase risk for MDS

17
A 70 yr old woman is evaluated for a 4 m h/o easy bruisability
A 70 yr old woman is evaluated for a 4 m h/o easy bruisability. Her medical history is otherwise non contributory. Physical exam and vitals are normal.CBC showed a Hb of 11.5, WBC of 4500 and pl of 35,000. Evidence of thrombocytopenia is noted on PBS. Pt is treated with prednisone, 1mg/kg/day. After 3 wks, pl count is 30,000. Which is the most appropriate next step: 1.Increase prednisone dose 2.Add anti-Rh D Ig 3.Perform bone marrow aspiration and biopsy 4.perform splenectomy

18
Bone marrow aspirate and biopsy should be done in pts with suspected ITP who do not respond to prednisone therapy.

19
A 32 yr old woman is evaluated during a routine exam
A 32 yr old woman is evaluated during a routine exam. She feels well and takes no medications. She has not had excessive bruising, epistaxis or gingival bleeding. She is not pregnant.PMH is otherwise non contributory. Physical exam and vitals are normal.CBC is normal except pl 40,000.PBS shows a decreased no. of pl, otherwise is normal. Which of the following is the most appropriate next step in management of this pt? 1.Antiplatelet antibody measurement 2.Bone marrow examination 3.Trial of prednisone 4.Periodic monitoring of pl count

20
Isolated thrombocytopenia in an otherwise healthy young pt is most commonly due to ITP Pts with ITP and low risk of bleeding as demonstrated by a pl count of >40,000 require only periodic monitoring of pl count. Measurement of antiplatelet glycoprotein abs may occasionally helpful in pt s with complex clinical and lab findings. Therapy for ITP is usually not initiated until pl count falls to <30,000.

21
A 34 yr old woman is evaluated prior to undergoing mammoplasty
A 34 yr old woman is evaluated prior to undergoing mammoplasty.during her teenage years, she was diagnosed with “abnormal blood” for which she received prednisone. She does not believe this therapy reversed her hematologic abnormality. Also has occasional epistaxis and heavy menses but no prior surgery or significant trauma.she has no children and takes only OTC antihistamines and tylenol prn. Her mother and sister had ITP for which her sister was treated with corticosteroids. Physical exam and vitals are normal.CBC unremarkable except pl count of 40,000. PBS shows a giant platelet. Which of the following is the most likely diagnosis: 1.Inherited thrombocytopenic condition 2.ITP 3.Drug induced thrombocytopenia 4.Pseudothrombocytopenia

22
An inherited thrombocytopenic disorder should be suspected in otherwise healthy pts with a low platelet count, giant pl on PBS, a family history of thrombocytopenia and who are refractory to steroids. ITP is not an inherited condition. The May-Hegglin anomaly, characterized by giant platelets and often only producing modest bleeding manifestations, is the likely inherited disorder in this patient.

24
THANK YOU!

Similar presentations

















 Thrombocytopenic Purpura AM Report 5/25/2010.>")

