Download presentation
Presentation is loading. Please wait.

1
Jayne Turner FY1 Arrowe Park 2013

2
WASH HANDS/ALCOHOL GEL!!! Introduce yourself Check patient’s name and DOB Explain what you are about to do and gain consent Position appropriately (45degrees) and expose
 and expose.")
3
Generally unwell? Weight loss? SOB? Use of accessory muscles, unable to complete sentences, rate and depth of respiration, pursed lip breathing Signs of pain Any audible wheeze or stridor or cough Any signs of cyanosis (peripheral) Oxygen Nebulisers Sputum pot
 Oxygen Nebulisers Sputum pot.")
4
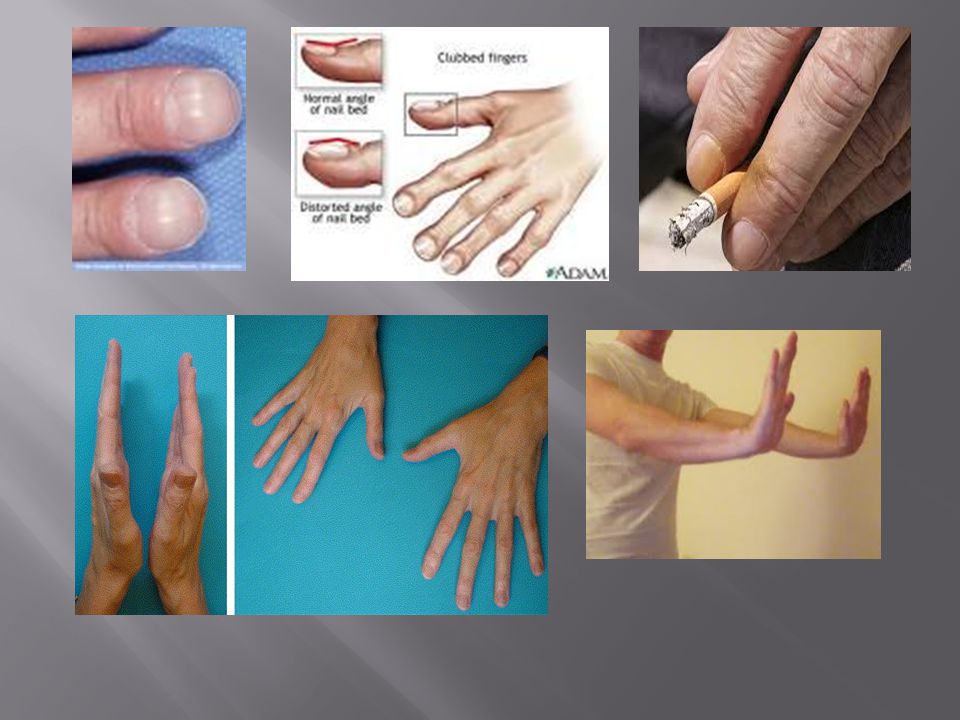
Flapping tremor – CO2 retention Tremor – B agonists Tar staining Capillary refill <2secs Clubbing (lung cancer, mesothelioma, fibrosis, bronchiectasis, cystic fibrosis) Wasting/weakness of intrinsic muscles (T1 lesion i.e. Pancoasts tumor Painful wrists (Hypertrophic pulmonary osteoarthropathy –HPOA – lung cancer) Pulse rate Respiratory rate – count for 15secs and multiply by 4
 Pulse rate Respiratory rate – count for 15secs and multiply by 4.")
6
Raised JVP – right sided heart failure (chronic lung disease/PE), obstruction Eyes – ptosis (miosis/constricted pupil and anhidrosis) of Horner’s syndrome, conjuctival pallor Tongue – central cyanosis Tracheal deviation – always warn the patient!! – deviated away from pneumothorax and towards collapse

8
Chest shape – carinatum, pectus excavatum, scoliosis Scars – always look around axilla Radiotherapy marks – tattoos

9
Always compare both sides <5cm in deep inspiration is abnormal Reduced expansion always suggests pathology on that side

10
Percussion using left hand middle finger flat against chest and tapping middle phalanx with middle finger of right hand Compare both sides

11
Resonant = normal lung Hyper resonant = pneumothorax, large bullae, COPD Dull = Consolidation, collapse, fibrosis “Stony dull” = pleural effussion

12
Ask patient to breath deeply in and out through their mouth while listen Ask yourself Are breath sounds present? Are breath sounds equal on both sides? Any added sounds – wheeze, crackles, pleural rubs? Breath sounds can be quiet/decreased with COPD (normal lung replaced by air)
.")
13
Added breath sounds: Wheeze = narrowed airways – can be monophonic (partial obstruction due to tumor) or polyphonic (multiple different size airways due to asthma/COPD) Crackles = re-opening of airways on inspiration which have become blocked during expiration – can be fine/high pitched (pulmonary oedema, fibrosis) or coarse (bronchiectasis, pneumonia)
 or polyphonic (multiple different size airways due to asthma/COPD) Crackles = re-opening of airways on inspiration which have become blocked during expiration – can be fine/high pitched (pulmonary oedema, fibrosis) or coarse (bronchiectasis, pneumonia)")
14
Ask patient to say “99” while auscultating areas of chest Increased resonance – consolidation or fibrosis Decreased resonance – pleural effusion or collapse

15
From behind the patient examine the submental, submandibular, and tonsillar glands and the deep cervical chain of glands in the anterior triangles of the neck. Examine for scalene node with index or middle finger dipping behind the clavicle. Have sternocleidomastoid relaxed by asking patient to flex head towards side of examination.

17
Look for ankle oedema – R sided Heart failure Check calves for swelling, tenderness – PE Thank the patient Turn to examiner and state that you would also like to check obs chart, including oxygen saturations. Bedside tests could include peak flow, sputum sample, ABG, CXR Present you findings

18
TRACHEA CAN BE DEVIATED IF LARGE ENOUGH EXPANSION reduced PERCUSSION stony dull AIR ENTRY reduced VOCAL RESONANCE reduced

19
TRACHEA central EXPANSION reduced PERCUSSION reduced VOCAL RESONANCE increased Bronchial breathing/coarse crackles

20
TRACHEA can be deviated towards affected side EXPANSION reduced PERCUSSION reduced BREATH SOUNDSreduced

21
TRACHEA can be deviated away in tension pneumothorax EXPANSION reduced PERCUSSION increased BREATH SOUNDS reduced/absent

22
..ANY QUESTIONS?

Similar presentations