Download presentation
Presentation is loading. Please wait.

1
“ If physicians would read two articles per day out of the six million medical articles published annually, in one year, they would fall 82 centuries behind in their reading. ” Miser WF, Critical Appraisal of the Literature. J Am Board Fam Pract, 12(4):315-333, 1999.
: ,")
2
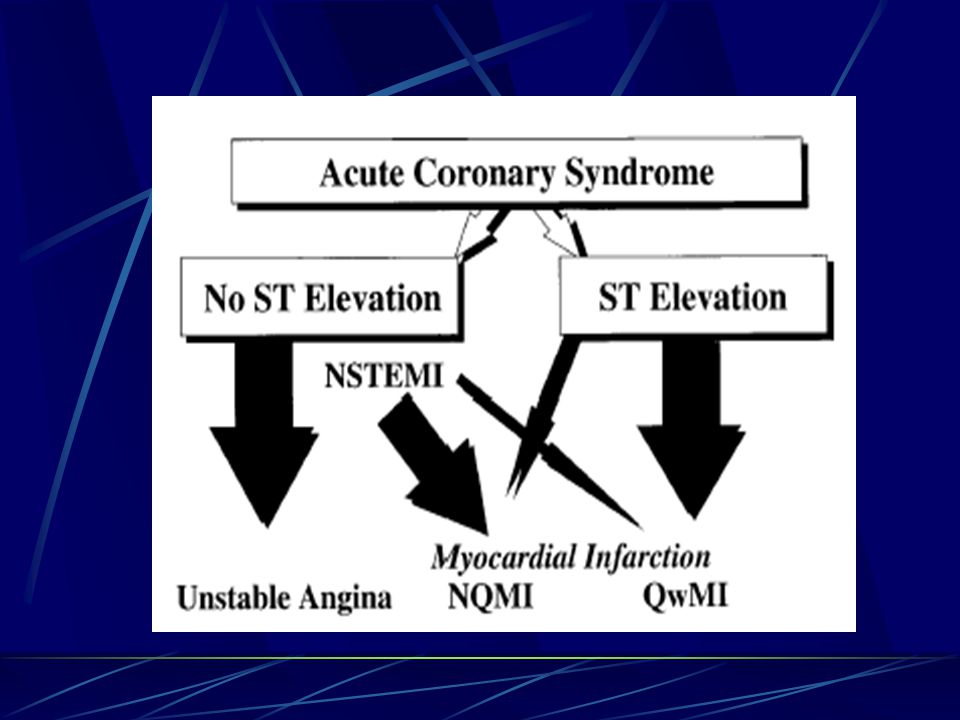
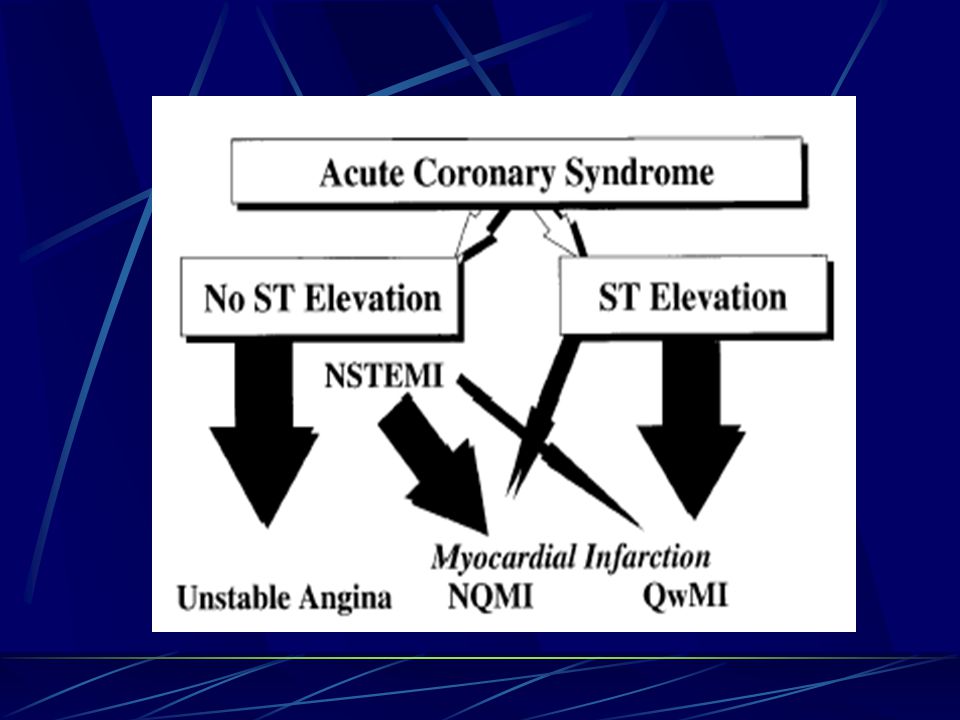
Acute Coronary Syndromes Coronary artery disease is the leading cause of death in the United States. Acute Coronary Syndrome (ACS) includes any constellation of symptoms compatible with acute myocardial ischemia: Acute MI (AMI) with ST-segment elevation and depression Q-wave and non-Q wave Unstable Angina (UA)
 includes any constellation of symptoms compatible with acute myocardial ischemia: Acute MI (AMI) with ST-segment elevation and depression Q-wave and non-Q wave Unstable Angina (UA).")
4
Acute Coronary Syndromes Can also be divided into: STEMI UA NSTEMI

5
The implication of ACS is for early diagnosis for appropriate clinical management, and placement in an environment with continuous EKG and defibrillation capability, where an EKG can be obtained and immediately interpreted. Priority is to identify patients with AMI to be considered for immediate reperfusion Rx, and recognize other potential catastrophic causes of sudden decompensation such as aortic dissection.

6
ST-Elevation Myocardial Infarction (STEMI) Pre-hospital Management Initial Management in the ER Reperfusion Therapy Initial Adjunctive Treatments Risk Stratification after MI
 Pre-hospital Management Initial Management in the ER Reperfusion Therapy Initial Adjunctive Treatments Risk Stratification after MI")
7
Pre-hospital Management Time is myocardium, regardless of the strategy to reperfusion. Prompt reperfusion: limits myocardial necrosis Preserves LV function Reduces mortality

8
Pre-hospital Management Most pts don ’ t seek care for 2 or more hours Pts should promptly administer ASA Dial 911 EMS should take pt to facility that can do PCI 16% reduction in mortality in pts given thrombolytic Rx before hospitalization ? Safety of Rx before correct dx & selection

9
Initial Management in the ER

10
STEMI Protocols in the ER result in rapid ID and Rx Initial diagnostic tests: EKG continuous monitoring of rhythm, HR & BP targeted Hx and PE stat blood for cardiac markers, heme, chemistry clotting and lipids chest X-ray

11
Selecting Optimal Reperfusion Rx for Pts with STEMI

13
Reperfusion Therapy Success depends on time to therapy < 30 minutes for thrombolytic rx > < 90 minutes for primary PCI Both are effective for achieving reperfusion

14
PCI in STEMI If it can be done rapidly, less risk of recurrent MI Stents better than POBA: < restenosis, better success rates

15
PCI not Available Or Long Door to Balloon (DB) Time Peripheral Hospital > mortality if DB time is > 2 hours If DB time > 1 hour, PCI is no better than fibrinolytic Rx
 Time Peripheral Hospital > mortality if DB time is > 2 hours If DB time > 1 hour, PCI is no better than fibrinolytic Rx")
16
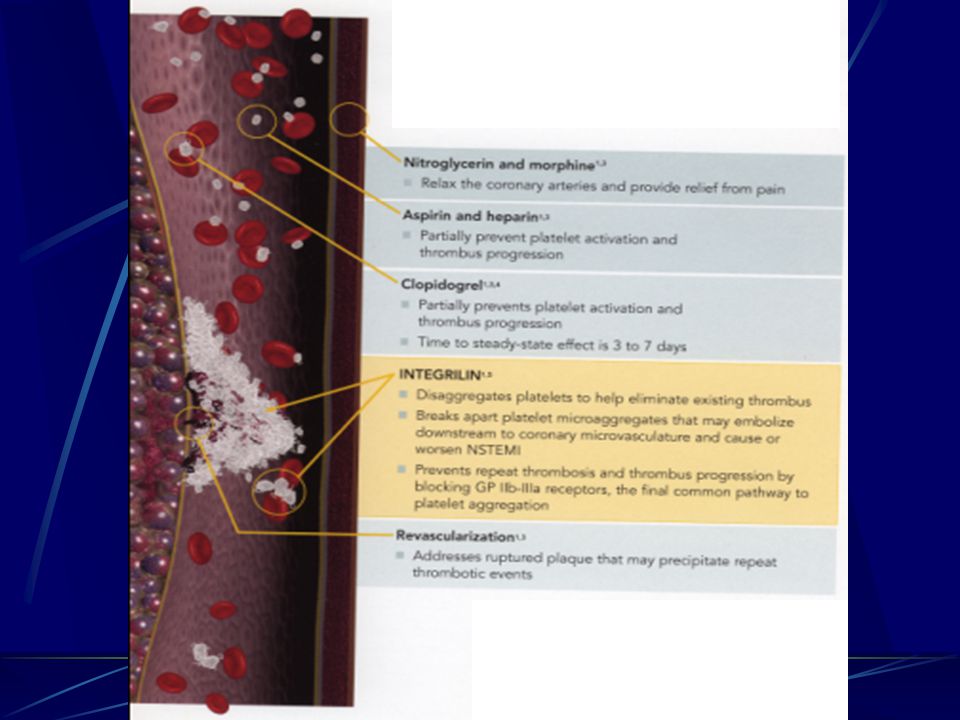
Initial Adjunctive Treatments Platelet activation and aggregation are important in STEMI causing persistence of thrombotic occlusions and resistance to fibrinolytic Rx and risk of reocclusion. Pathways leading to platelet activation and aggregation are thus targets of therapy.

17
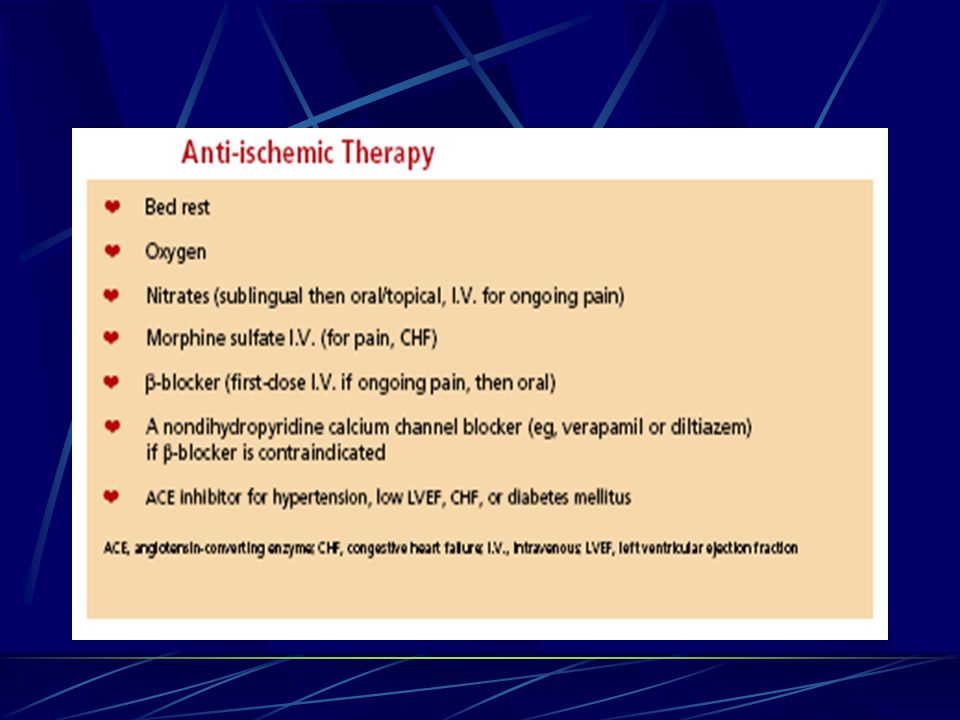
Initial Adjunctive Treatments ASA given to all (160 – 325mg) Plavix in pts allergic to ASA Glycoprotein IIb/IIIa inhibitors for all undergoing PCI Thrombin Inhibitors (UFH or LMWH) O 2 NTG IV B-blockers ACE-I Analgesia
 Plavix in pts allergic to ASA Glycoprotein IIb/IIIa inhibitors for all undergoing PCI Thrombin Inhibitors (UFH or LMWH) O 2 NTG IV B-blockers ACE-I Analgesia")
18
Risk Stratification after MI Ischemic Risk LV Function Arrhythmic Substrate

19
Ischemic Risk Identifying residual ischemia is to identify high-risk pts who will benefit from revascularization. Post MI stress test – not necessary in pts who had PCI

20
LV Function LV function and Valvular disease usually assessed with echocardiography Myocardial stunning may persist for 2 weeks

21
Assessment of Risk for Arrhythmia Important to assess risk or early or late arrhythmic deaths is important after STEMI ICD implants in pts with low LVEF after MI reduces mortality Accuracy of prediction is not good

23
Unstable Angina and Non--ST-Segment Elevation MI UA and NSTEMI

25
1.5 million patients annually admitted to hospitals in US Many advances in last few years: Antiplatelet therapies Cholesterol lowering B-blockade

26
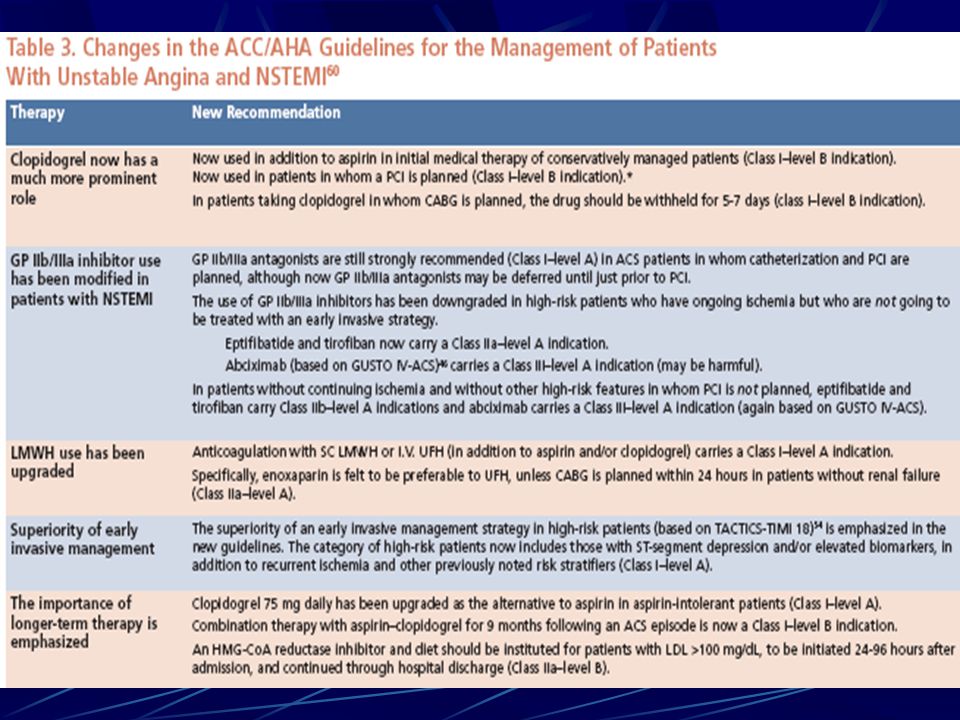
ACC/AHA

27
Overview of Guidelines

28
Features with Higher Liklihood of ACS

29
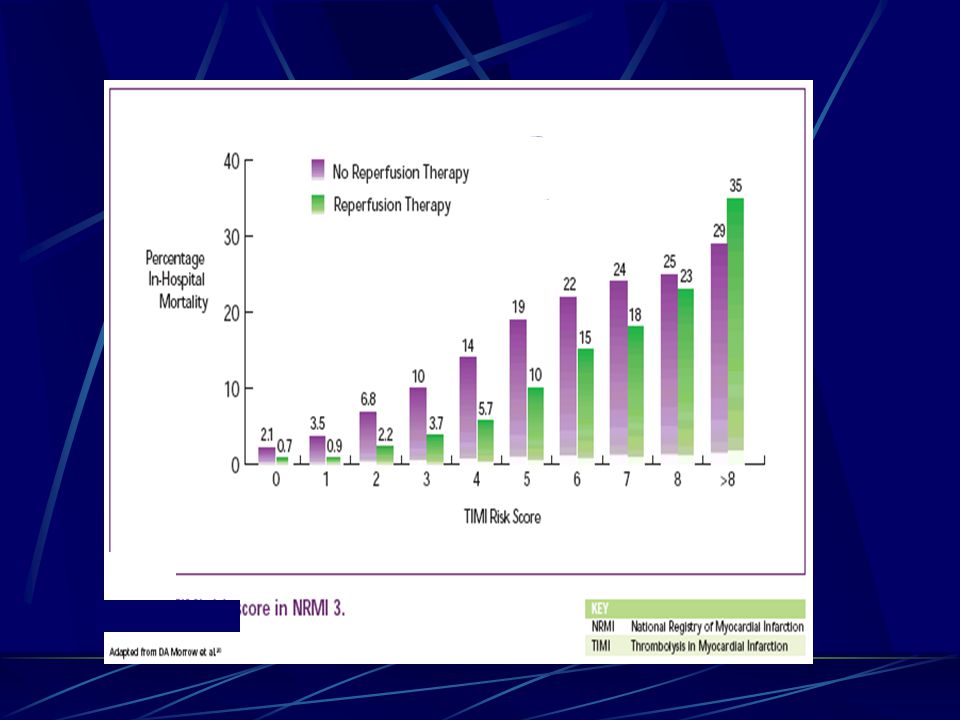
TIMI Risk Score for UA/NSTEMI Predicts Risk of Death, MI, or Recurrent Ischemia

30
Effects of Plavix Stratified by TIMI Risk Score at 12 Months

31
Benefit of IIb/IIIa Inhibitors in UA/NSTEMI by Troponin

32
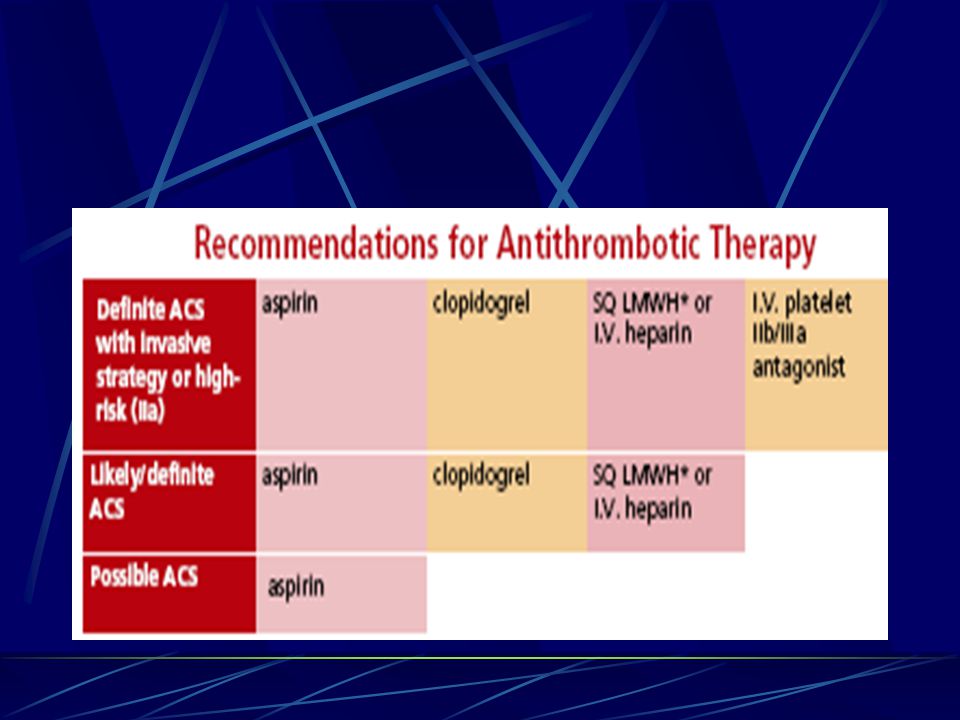
Antiplatelet Treatment Antiplatelet Therapy is the Cornerstone in the Management of UA/NSTEMI

33
Antiplatement Therapy ASA reduces events by 50% to 70% compared with placebo. (160-325mg in hospital, 81mg at discharge). Plavix (Clopidogrel) in patients who cannot take ASA.
. Plavix (Clopidogrel) in patients who cannot take ASA..")
34
Antiplatement Therapy Clopidogrel is a class I recommendation in addition to ASA CURE Trial Clopidogrel + ASA had 20% reduction of CV death, MI and stroke vs ASA alone in both high and low risk pts with UA/NSTEMI. The benefits were seen at 2 hours and 1 year. 31% reduction in cardiac events at 1 and 12 months

35
Glycoprotein IIb/IIIa Inhibitors Upstream Management with Integrilin (eptifibatide) shows clear benefit, Reopro (abciximab) none in pts treated conservatively Aciximab is strongly beneficial in pts undergoing PCI Pts at high risk benefit from GP IIb/IIIa inhibitors
 shows clear benefit, Reopro (abciximab) none in pts treated conservatively Aciximab is strongly beneficial in pts undergoing PCI Pts at high risk benefit from GP IIb/IIIa inhibitors")
36
UFH and LMWH All pts with US/NSTEMI Incremental benefit over ASA alone Lovenox (enoxaparin) (LMWH) superior to UFH in reducing recurrent cardiac events Beware of pts with bleeding histories
 (LMWH) superior to UFH in reducing recurrent cardiac events Beware of pts with bleeding histories")
39
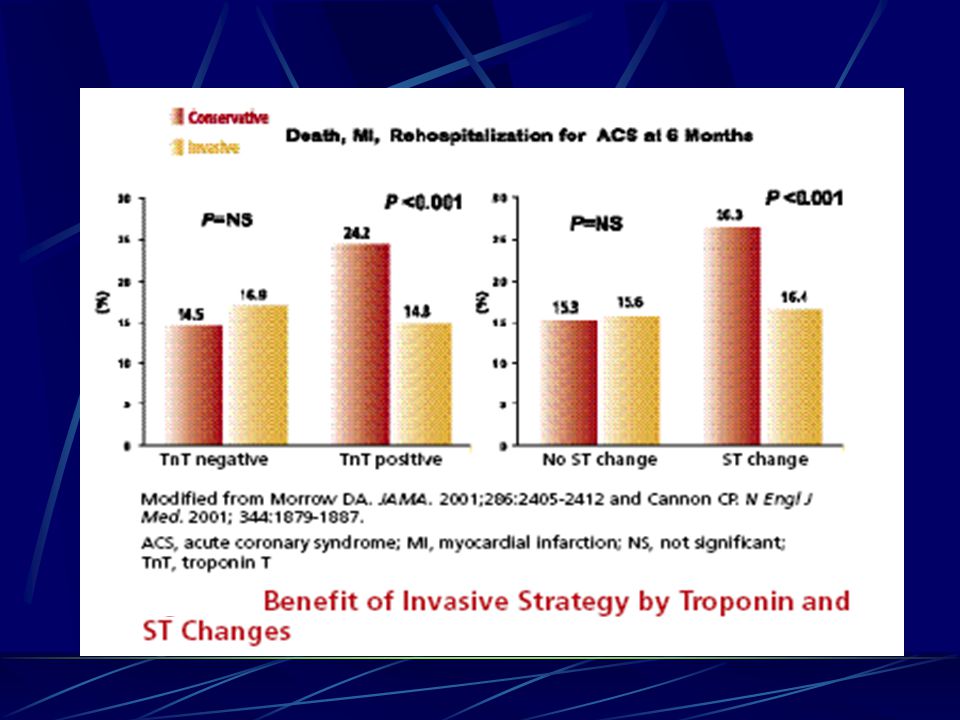
Invasive vs Conservative Strategy Especially in high risk pts (ST changes and Tp positive

40
An early invasive strategy is cost- effective with a cost of $17,500 per life saved

42
Summary of Hospital Strategy

43
Summary of Invasive Strategy

44
Long Term Therapy

Similar presentations














 Definition of ACS Signs and symptoms of ACS Gender and age related difference in ACS Pathophysiology.>")
 CAD is most common form of heart disease and causes premature death. In UK, 1 in 3 men and.>")

. ACS Pathophysiology is that of a ruptured or eroded atheromatous plaque. Pathophysiology is that of a ruptured or eroded.>")



