Download presentation
Presentation is loading. Please wait.

1
SLE and Kidney Disease in 2014 GERALD APPEL, MD GERALD APPEL, MD Professor of Clinical Medicine Columbia University –College of Professor of Clinical Medicine Columbia University –College of Physicians and Surgeons Physicians and Surgeons NY-Presbyterian Hospital New York, New York NY-Presbyterian Hospital New York, New York

2
Lupus and Kidney Disease What are the kidneys – how do they work? ( what is a nephrologist?) How does SLE involve the kidneys? How do you know if you have kidney involvement? Are there different patterns of Kidney disease with SLE? What happened with SLE Kidney disease ( lupus nephritis )in the past ? Can we treat kidney disease due to LN today? How successful are we? Will there be new ways to treat it tomorrow.
 How does SLE involve the kidneys. How do you know if you have kidney involvement. Are there different patterns of Kidney disease with SLE. What happened with SLE Kidney disease ( lupus nephritis )in the past . Can we treat kidney disease due to LN today. How successful are we. Will there be new ways to treat it tomorrow..")
3
Lupus and Kidney Disease What are the kidneys – how do they work? ( what is a nephrologist?) How does SLE involve the kidneys? How do you know if you have kidney involvement? Are there different patterns of Kidney disease with SLE? What happened with SLE Kidney disease ( lupus nephritis )in the past ? Can we treat kidney disease due to LN today? How successful are we? Will there be new ways to treat it tomorrow.
 How does SLE involve the kidneys. How do you know if you have kidney involvement. Are there different patterns of Kidney disease with SLE. What happened with SLE Kidney disease ( lupus nephritis )in the past . Can we treat kidney disease due to LN today. How successful are we. Will there be new ways to treat it tomorrow..")
4
Where can one find a kidney?

8
Lupus and Kidney Disease What are the kidneys – how do they work? ( what is a nephrologist?) How does SLE involve the kidneys? How do you know if you have kidney involvement? Are there different patterns of Kidney disease with SLE? What happened with SLE Kidney disease ( lupus nephritis )in the past ? Can we treat kidney disease due to LN today? How successful are we? Will there be new ways to treat it tomorrow.
 How does SLE involve the kidneys. How do you know if you have kidney involvement. Are there different patterns of Kidney disease with SLE. What happened with SLE Kidney disease ( lupus nephritis )in the past . Can we treat kidney disease due to LN today. How successful are we. Will there be new ways to treat it tomorrow..")
9
ISN/RPS Classification of LN Class I Minimal mesangial LN Class II Mesangial proliferative LN Class III Focal LN III (A): Active lesions: focal proliferative LN III (A/C): Active and chronic lesions III (C): Chronic inactive lesions with scars Class IV Diffuse LN IV-S (A): Active lesions: diffuse segmental proliferative LN IV-G (A): Active lesions: diffuse global proliferative LN IV-S (A/C): Active and chronic lesions IV-G (A/C): Active and chronic lesions IV-S (C): Chronic inactive lesions with scars IV-G (C): Chronic inactive lesions with scars Class V Membranous LN Class VI Advanced sclerotic LN ISN = International Society of Nephrology; RPS = Renal Pathology Society
: Active lesions: focal proliferative LN III (A/C): Active and chronic lesions III (C): Chronic inactive lesions with scars Class IV Diffuse LN IV-S (A): Active lesions: diffuse segmental proliferative LN IV-G (A): Active lesions: diffuse global proliferative LN IV-S (A/C): Active and chronic lesions IV-G (A/C): Active and chronic lesions IV-S (C): Chronic inactive lesions with scars IV-G (C): Chronic inactive lesions with scars Class V Membranous LN Class VI Advanced sclerotic LN ISN = International Society of Nephrology; RPS = Renal Pathology Society")
10
Lupus Nephritis Class I

11
Lupus Nephritis Class II

12
Lupus Nephritis Class III

14
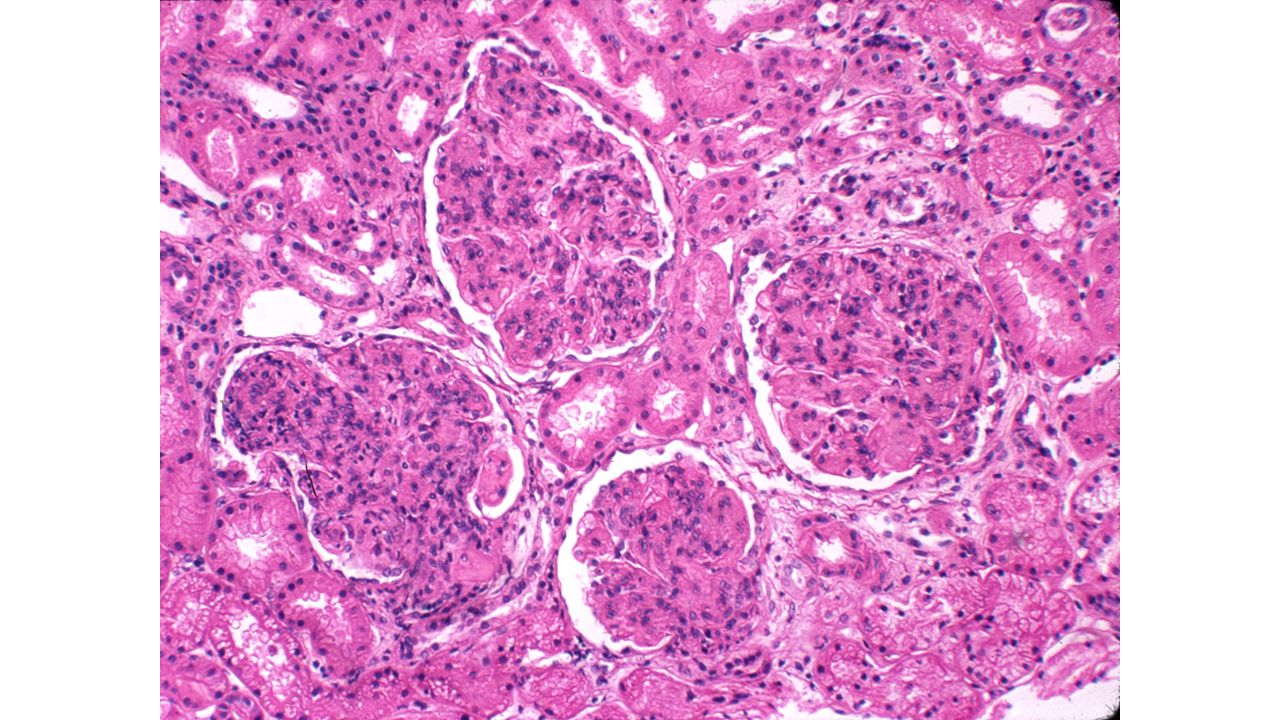
Histology WHO Class IV: Diffuse Endocapillary Proliferation With Karyorrhexis and Focal Necrosis Focal NecrosisEndocapillary Proliferation

15
Lupus Nephritis Class IV Pre-Rx Post-Rx

16
Lupus Nephritis Class IV

17
Lupus Nephritis Class V

18
End stage kidney due to chronic GN: Diffuse and global glomerulosclerosis, tubular atrophy & interstitial fibrosis

19
Lupus and Kidney Disease What are the kidneys – how do they work? ( what is a nephrologist?) How does SLE involve the kidneys? How do you know if you have kidney involvement? Are there different patterns of Kidney disease with SLE? What happened with SLE Kidney disease ( lupus nephritis )in the past ? Can we treat kidney disease due to LN today? How successful are we? Will there be new ways to treat it tomorrow.
 How does SLE involve the kidneys. How do you know if you have kidney involvement. Are there different patterns of Kidney disease with SLE. What happened with SLE Kidney disease ( lupus nephritis )in the past . Can we treat kidney disease due to LN today. How successful are we. Will there be new ways to treat it tomorrow..")
20
Case 3: Saleswoman with rash and arthritis A 29 year old saleswoman develops arthritis multiple joints, fever Exam: Lymphadenopathy, and a malar rash. Labs: –Urinalysis 3+ protein, 18-20 rbc’s –Creatinine 1.2 mg/dl –24 hr. protein 1.8 g per day –Complement 18% (normal 50-150%) –ANA positive, Anti-DNA antibody positive KIDNEY BIOPSY PERFORMED
 –ANA positive, Anti-DNA antibody positive KIDNEY BIOPSY PERFORMED.")
21
RBC cast forms a mold of tubular lumen

22
Diffuse proliferative lupus nephritis: Diffuse and global mesangial and glomerular capillary wall positivity for IgG Full house IF staining: IgG, IgM, IgA, C3, C1q

23
Lupus and Kidney Disease What are the kidneys – how do they work? ( what is a nephrologist?) How does SLE involve the kidneys? How do you know if you have kidney involvement? What happened with SLE Kidney disease ( lupus nephritis )in the past ? Can we treat kidney disease due to LN today? How successful are we? Will there be new ways to treat it tomorrow.
 How does SLE involve the kidneys. How do you know if you have kidney involvement. What happened with SLE Kidney disease ( lupus nephritis )in the past . Can we treat kidney disease due to LN today. How successful are we. Will there be new ways to treat it tomorrow..")
24
EventCy Therapy (n = 21) Combination Therapy (n = 20) n/n Hypertension10/20 Ischemic heart disease1/194/19 Hyperlipidemia7/208/19 Valvular heart disease9/197/21 Avascular necrosis6/216/20 Osteoporosis4/183/19 Premature menopause9/1610/18 Major infections7/219/20 Herpes zoster infection6/215/20 Side Effects of Cyclophosphamide in the past
 Combination Therapy (n = 20) n/n Hypertension10/20 Ischemic heart disease1/194/19 Hyperlipidemia7/208/19 Valvular heart disease9/197/21 Avascular necrosis6/216/20 Osteoporosis4/183/19 Premature menopause9/1610/18 Major infections7/219/20 Herpes zoster infection6/215/20 Side Effects of Cyclophosphamide in the past")
25
Lupus and Kidney Disease What are the kidneys – how do they work? ( what is a nephrologist?) How does SLE involve the kidneys? How do you know if you have kidney involvement? Are there different patterns of Kidney disease with SLE? What happened with SLE Kidney disease ( lupus nephritis )in the past ? Can we treat kidney disease due to LN today? How successful are we? Will there be new ways to treat it tomorrow.
 How does SLE involve the kidneys. How do you know if you have kidney involvement. Are there different patterns of Kidney disease with SLE. What happened with SLE Kidney disease ( lupus nephritis )in the past . Can we treat kidney disease due to LN today. How successful are we. Will there be new ways to treat it tomorrow..")
26
MMF + glucocorticoids (e.g. pulse methylprednisolone ) CYC + Glucocorticoids (e.g. pulse methylprednisolone) CYC + Glucocorticoids (e.g. pulse methylprednisolone) or EURO LUPUS Low-dose CYC EURO LUPUS Low-dose CYC NIH study Hi-dose CYC NIH study Hi-dose CYC or 6 months INDUCTION Proliferative LN ACR- KDIGO Treatment guidelines – CONFIDENTIAL Anti-MIF & LN Ad Board, July 13, 2011
 CYC + Glucocorticoids (e.g. pulse methylprednisolone) or EURO LUPUS Low-dose CYC EURO LUPUS Low-dose CYC NIH study Hi-dose CYC NIH study Hi-dose CYC or 6 months INDUCTION Proliferative LN ACR- KDIGO Treatment guidelines – CONFIDENTIAL Anti-MIF & LN Ad Board, July 13,")
27
Proliferative Lupus Nephritis – Maintenance Treatment ACR – KDIGO Treatment guidelines IMPROVED NOT IMPROVED MMF induction MMF induction MMF1-2g/d or AZA 2 mg/kg/d ± lo dose daily GC CYC (lo- or hi- dose) + pulse GC then daily GC CYC (lo- or hi- dose) + pulse GC then daily GC 6 months CYC induction CYC induction IMPROVED NOT IMPROVED MMF1-2g/d or AZA 2 mg/kg/d ± lo dose daily GC MMF 2-3g/d x 6 months + pulse GC then daily GC MMF 2-3g/d x 6 months + pulse GC then daily GC 6 months
 + pulse GC then daily GC CYC (lo- or hi- dose) + pulse GC then daily GC 6 months CYC induction CYC induction IMPROVED NOT IMPROVED MMF1-2g/d or AZA 2 mg/kg/d ± lo dose daily GC MMF 2-3g/d x 6 months + pulse GC then daily GC MMF 2-3g/d x 6 months + pulse GC then daily GC 6 months")
28
Lupus and Kidney Disease What are the kidneys – how do they work? ( what is a nephrologist?) How does SLE involve the kidneys? How do you know if you have kidney involvement? Are there different patterns of Kidney disease with SLE? What happened with SLE Kidney disease ( lupus nephritis )in the past ? Can we treat kidney disease due to LN today? How successful are we? Will there be new ways to treat it tomorrow.
 How does SLE involve the kidneys. How do you know if you have kidney involvement. Are there different patterns of Kidney disease with SLE. What happened with SLE Kidney disease ( lupus nephritis )in the past . Can we treat kidney disease due to LN today. How successful are we. Will there be new ways to treat it tomorrow..")
29
ELNT - 10 year FU - ESRD Houssiau FA et al. Ann Rheum Dis 2009,

30
ELNT - 10 year FU Houssiau FA et al. Ann Rheum Dis 2009, Jan 20 (Epub ahead of print)
")
31
ALMS TRIAL Primary Endpoint: Responders at Month 6 Response judged by blinded Clinical Endpoint Committee: Decrease in proteinuria to <3g if baseline nephrotic (≥3g/d), or by ≥50% in patients ith subnephrotic (<3g/d) proteinuria and Stabilization of serum creatinine level (24-week level ± 25% of baseline), or improvement MMF was not superior to IVC (p = 0.575) MMF IVC Appel, Contreras, Dooley et al JASN 2009
, or by ≥50% in patients ith subnephrotic (<3g/d) proteinuria and Stabilization of serum creatinine level (24-week level ± 25% of baseline), or improvement MMF was not superior to IVC (p = 0.575) MMF IVC Appel, Contreras, Dooley et al JASN 2009")
32
IVC MMF ALMS Trial - Renal Variables Serum creatinine and urine protein levels improved in both the MMF and IVC groups

33
Lupus and Kidney Disease What are the kidneys – how do they work? ( what is a nephrologist?) How does SLE involve the kidneys? How do you know if you have kidney involvement? Are there different patterns of Kidney disease with SLE? What happened with SLE Kidney disease ( lupus nephritis )in the past ? Can we treat kidney disease due to LN today? How successful are we? Will there be new ways to treat it tomorrow.
 How does SLE involve the kidneys. How do you know if you have kidney involvement. Are there different patterns of Kidney disease with SLE. What happened with SLE Kidney disease ( lupus nephritis )in the past . Can we treat kidney disease due to LN today. How successful are we. Will there be new ways to treat it tomorrow..")
34
Rituximab: Anti-CD20 Monoclonal Antibody Rituximab - FDA approved for the treatment of relapsed or refractory, CD20-positive B-cell NHLymphomas Approved for Rheumatoid Arthritis – used in 240,000 patients > 10 yrs Approved for ANCA+ glomerulonephritis since 2010 Chimeric murine/human monoclonal antibody Davies B, Shaw T. Presented at EULAR 2004. Maloney DG, et al. J Clin Oncol. 1997;15(10):3266-3274.
:")
35
Rituxilup Trial MPred + MMF + Rituximab vs MP + MMF + steroids ( ALMS regimen ) 19 Adult + 4 Peds Centers in UK; Europe 12 Centers in 3 networks; US Centers. Non-inferiority Trial of 252 LN patients Primary endpoint complete remission at 1 yr. Secondary Endpoints – Time to CR, Partial remissions, PR with histologic response, serious infections, SAEs, SRI score etc.

37
Navarra, et al. Lancet. 2011;377(9767):721-31 Furie, et al. Arthritis Rheum. 2011;63(12):3918-30 1 mg/kg belimumab 60 40 20 0 048 12 16202428323640444852 Visit Week SRI Responders (%) +++ * + * + * + * + * + * + * * p<0.05 + p<0.05 10 mg/kg belimumab Placebo 50 40 30 20 10 0 048162432 40 48 52 6068 76 Visit Week % SRI Responders * Belimumab – FDA Approved for SLE p<0.05 SRI, SLE Responder Index IMNL-SCT-019799
: mg/kg belimumab Visit Week SRI Responders (%) +++ * + * + * + * + * + * + * * p< p< mg/kg belimumab Placebo Visit Week % SRI Responders * Belimumab – FDA Approved for SLE p<0.05 SRI, SLE Responder Index IMNL-SCT")
38
Abatacept ( CTLA4Ig Co-Stimulatory Blocker ) Study in 300 LN PTS Background Rx: MMF up to 3 g/day plus corticosteroids Primary Outcome Measure: Time to complete response Abatacept 10/10 10 mg/kg days 1,15, 29, then Q 28 days Abatacept 10/10 10 mg/kg days 1,15, 29, then Q 28 days Abatacept 30/10 30 mg/kg x4, then 10 mg/kg Q 28 days Abatacept 30/10 30 mg/kg x4, then 10 mg/kg Q 28 days Placebo Days 1 and 15 (1 st and 2 nd dose) Day 337 Final dose Dose every 28 days Randomization 1:1:1 Courtesy of D Wofsy
 Study in 300 LN PTS Background Rx: MMF up to 3 g/day plus corticosteroids Primary Outcome Measure: Time to complete response Abatacept 10/10 10 mg/kg days 1,15, 29, then Q 28 days Abatacept 10/10 10 mg/kg days 1,15, 29, then Q 28 days Abatacept 30/10 30 mg/kg x4, then 10 mg/kg Q 28 days Abatacept 30/10 30 mg/kg x4, then 10 mg/kg Q 28 days Placebo Days 1 and 15 (1 st and 2 nd dose) Day 337 Final dose Dose every 28 days Randomization 1:1:1 Courtesy of D Wofsy")
39
Brad H. Rovin on behalf of the ACCESS Trial Group Treatment of LN with Abatacept and Low- Dose Pulse Cyclophosphamide: The ACCESS Trial Brad H. Rovin on behalf of the ACCESS Trial Group EuroLupus Low dose Cyclophosphamide and prednisone starting at 60 mg (tapering to 10 mg by week 12 ) Azathioprine 2 mg/kg/day PO maintenance Abatacept 500 mg or 1000 mg at 0, 2, 4, then Q4 wk until week 24 vs Placebo
 Azathioprine 2 mg/kg/day PO maintenance Abatacept 500 mg or 1000 mg at 0, 2, 4, then Q4 wk until week 24 vs Placebo.")
40
Proteasome Inhibitors N H H NB O OH OH O N N Bortezomib ™) ( Velcade™) Carfilzomib (Kyprolis) ManufacturerTakedaOnyx/Amgen StatusApproved Indications Myeloma & Mantle Cell Lymphoma Myeloma & Solid Tumors ClassBoronic AcidKetoepoxide Active Sites Targeted 5/LMP7/LMP2 5/LMP7
 ( Velcade™) Carfilzomib (Kyprolis) ManufacturerTakedaOnyx/Amgen StatusApproved Indications Myeloma & Mantle Cell Lymphoma Myeloma & Solid Tumors ClassBoronic AcidKetoepoxide Active Sites Targeted 5/LMP7/LMP2 5/LMP7")
41
Bortezomib for NZB/W F1: Kidney Disease Neubert Nat. Med. 2008

42
An Open Label Randomized Phase IV Study of the Safety and Efficacy of ACTHAR GEL in Patients with Membranous (Class V) Lupus Nephritis Principal Investigator: Brad H. Rovin MD, Ohio State University SCRN 0 1 2 3 4 5 6 9 12 Study Month ARM 1. Acthar Gel 80 IU administered subcutaneously 2 times per week, 12 patients ARM 2. Acthar Gel 80 IU administered subcutaneously 3 times per week, 13 patients Administration of ActharFollow-Up Primary Objectives: To determine the safety and tolerability of Acthar Gel in patients with Class V lupus nephritis To determine the efficacy of Acthar Gel in patients with Class V lupus nephritis as CRR+PRR

43
Treatment of Severe LN in the Future Treatment will still be divided into an induction and maintenance phase. Induction therapy will consist of Cyclophosphamide (usually IV ) or MMF or Newer regimens e.g. older drugs combined with CNI’s, ACTH, proteosome inhibitors, or corticosteroid free Rituximab regimens. Maintenance therapy will consist of MMF or AZA or rituximab or other newer agents. Use of combinations of immunosuppressives will increase. One Regimen Will Not Fit All
 or MMF or Newer regimens e.g. older drugs combined with CNI’s, ACTH, proteosome inhibitors, or corticosteroid free Rituximab regimens. Maintenance therapy will consist of MMF or AZA or rituximab or other newer agents. Use of combinations of immunosuppressives will increase. One Regimen Will Not Fit All.")
44
Lupus and Kidney Disease What are the kidneys – how do they work? ( what is a nephrologist?) How does SLE involve the kidneys? How do you know if you have kidney involvement? Are there different patterns of Kidney disease with SLE? What happened with SLE Kidney disease ( lupus nephritis )in the past ? Can we treat kidney disease due to LN today? How successful are we? Will there be new ways to treat it tomorrow.
 How does SLE involve the kidneys. How do you know if you have kidney involvement. Are there different patterns of Kidney disease with SLE. What happened with SLE Kidney disease ( lupus nephritis )in the past . Can we treat kidney disease due to LN today. How successful are we. Will there be new ways to treat it tomorrow..")
Similar presentations






 51 year old Caucasian female Presented with nephrotic syndrome and hypertension in 2000.>")

 a synthetic Toleragen molecule consisting of four double-stranded oligodeoxyribonucleotides attached to nonimmunogenic polyethylene.>")












