Download presentation
Presentation is loading. Please wait.

1
http://sorrel.humboldt.edu/~jlg21/Zoo%20310/Lab%2017%20ADAM%20respiratory/resp%20system%20home.html “Interactive Physiology” A.D.A.M. – Benjamin Cummings Figuras extraídas de

2
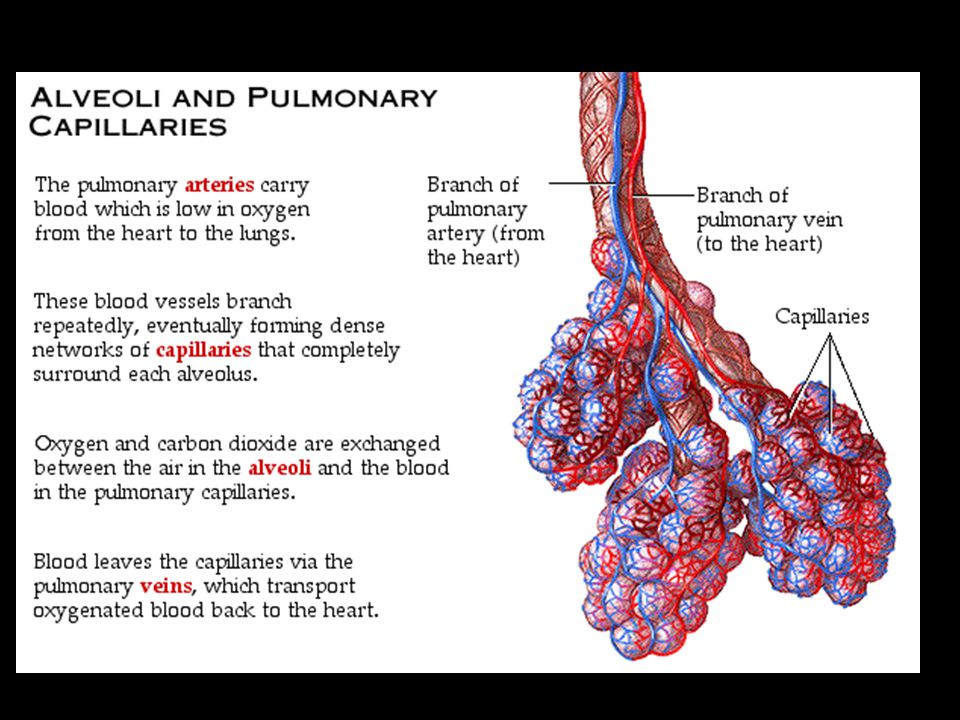
As they function, our cells use oxygen and produce carbon dioxide. The respiratory system brings the needed oxygen into and eliminates carbon dioxide from the body. The blood transports these gases, carrying oxygen to the tissues and carbon dioxide to the lungs.

3
Pleurae. The pleural cavity is a thin space between the parietal and vischeral pleurae, which contains a thin layer of pleural fluid. The pleural fluid assists in breathing by acting as a lubricant.

8
Alvéolo sem surfactante Alvéolo com surfactante Role of Surfactant Water in the alveolar fluid creates surface tension. Surface tension is due to the strong attraction between water molecules at the surface of a liquid, which draws the water molecules closer together. Surfactant is a mixture of phospholipids and lipoproteins which lowers the surface tension of the alveolar fluid. Without surfactant, alveoli would have to be completely reinflated between breaths.

9
Muscle activity causes changes in the volume of the thoracic cavity during breathing. Changing the thoracic cavity volume causes intrapulmonary and intrapleural pressure changes, which allow air to move from high pressure to low pressure regions. Airway resistance is normally low, but nervous stimulation and chemical factors can change the diameter of bronchioles, thereby altering resistance and airflow. Lung compliance is normally high de to the lungs abundant elastic tissue and surfactant's ability to lower the surface tension of the alveolar fluid.

10
Intrapleural pressure is the pressure within the pleural cavity. It is always negative, which acts as a suction to keep the lungs inflated. The negative intrapleural pressure is due to: Surface tension of alveolar fluid Elasticity of lungs Elasticity of thoracic wall

11
As the thoracic wall moves outward during inspiration, the intrapleural pressure becomes even more negative. As the thoracic wall recoils during expiration, the pressure returns to normal (756 mm Hg).
..")
12
Pneumothorax is the collapse of the lung due to a puncture into the pleural cavity of the chest wall or the lung. The collapse results from air entering the pleural cavity, as it moves from high pressure to low pressure. If one lung is punctured, the other lung is unaffected. This is because the lungs are completely separate from one another. Each is surrounded by its own pleural cavity and pleural membranes. Therefore, changes in the intrapleural pressure of one lung is independent of the other lung.

15
As air flows into the lungs, the gas molecules encounter resistance when they strike the walls of the airway. Therefore, the diameter of the airway affects resistance. When the diameter decreases, the resistance increases because more gas molecules encounter the airway wall. Airflow is inversely related to resistance. This relationship is shown by the equation:

16
Factors Affecting Resistance Parasympathetic neurons release the neurotransmitter acetylcholine, which constricts bronchioles. Therefore, as seen by equation, the increased airway resistance decreases airflow. Histamine, released during allergic reactions, constricts bronchioles. This increases airway resistance and decreases airflow, making it harder to breathe. Epinephrine, released by the adrenal medulla, dilates bronchioles, decreasing airway resistance. This greatly increases airflow, ensuring adequate gas exchange

19
Oxygen is transported in two ways: dissolved in plasma (1.5%) bound to hemoglobin as oxyhemoglobin (98.5%) Hemoglobin Hemoglobin can transport up to 4 O2's. When 4 O2's are bound to hemoglobin, it is 100% saturated. Oxygen binding occurs in response to the high PO2 in the lungs.

20
Factors Altering Hemoglobin Saturation: Low PO2's; Low pH; High temperature; High PCO2 and High BPG (2,3-bisphosphoglycerate) The last 4 conditions result from heavy exercise and decrease hemoglobin's affinity for oxygen, releasing more oxygen to the active muscle cells.
 The last 4 conditions result from heavy exercise and decrease hemoglobin s affinity for oxygen, releasing more oxygen to the active muscle cells.")
22
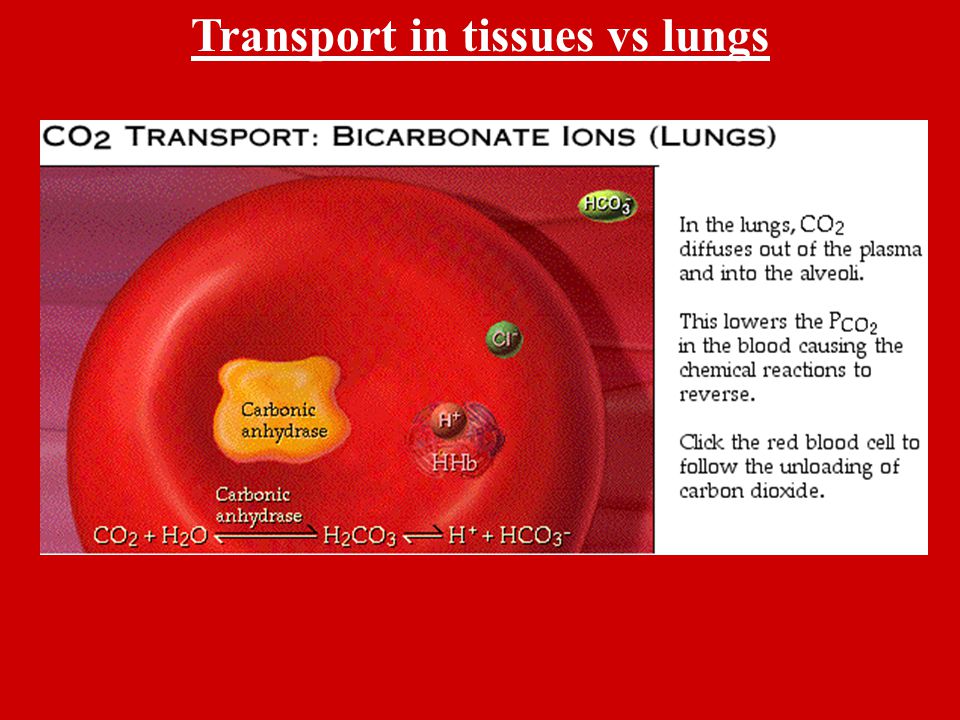
Transport in tissues vs lungs

24
O 2 loading facilitates CO 2 unloading from hemoglobin. This is known as the Haldane effect.

29
Carbon dioxide is very soluble in blood, allowing many molecules to diffuse along this small partial pressure gradient. Oxygen, on the other hand, is less soluble, requiring a larger concentration gradient. As you inhale, you replenish oxygen. As you exhale, you eliminate carbon dioxide. Oxygen Loading Carbon Dioxide unloading

31
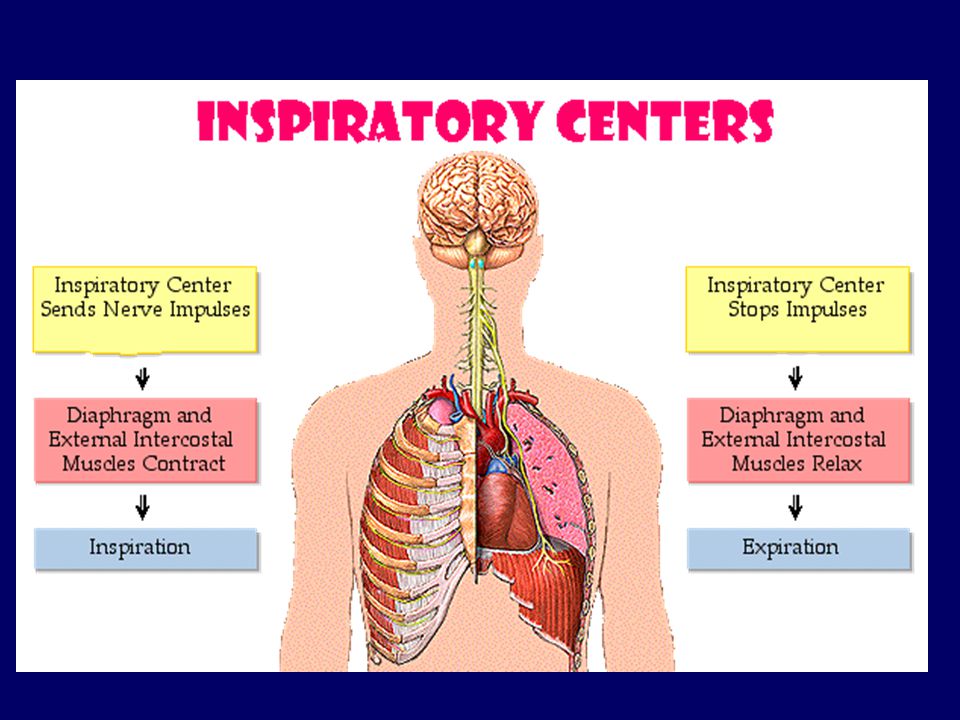
The control of respiration is tied to the principle of homeostasis (image right). The basic rhythm of breathing is set by the inspiratory center, located in the medulla. The inspiratory center sets the rhythm by automatically initiating inspiration (image below).
..")
33
Location of Chemoreceptors The basic rhythm of breathing is modified by input from the central and peripheral chemoreceptors. They respond to changes in the PCO2, pH, and PO2 of arterial blood. These are the most important factors that alter ventilation.

34
Changes in PCO 2, pH, and PO 2.

37
Hyperventilation

38
Hypoventilation

Similar presentations























 To improve gas absorption Increase surface.>")









