Download presentation
Presentation is loading. Please wait.

1
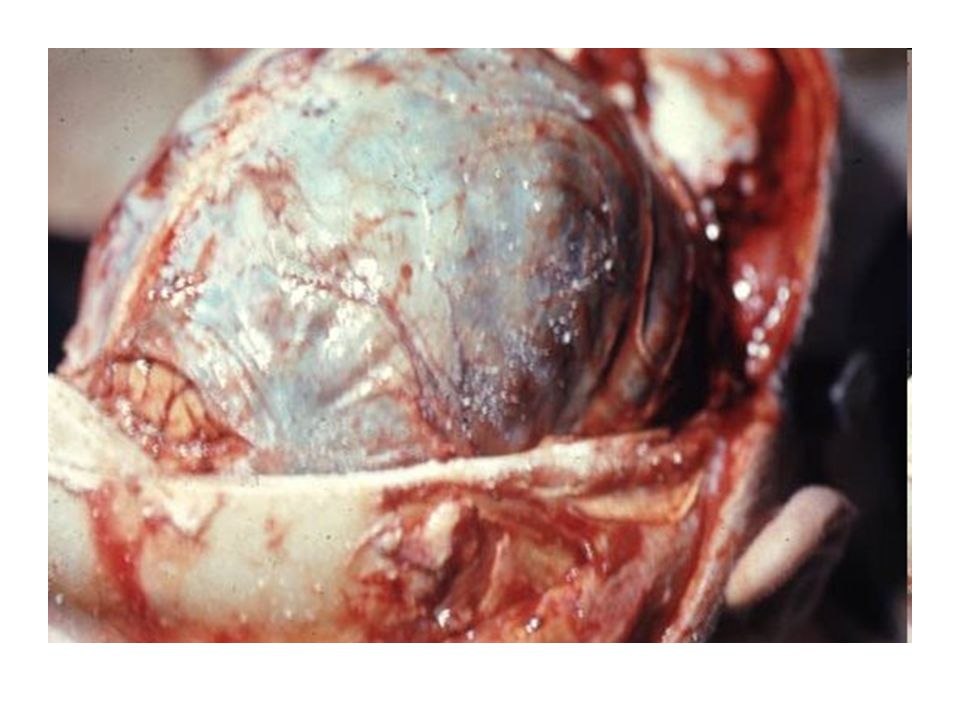
SEVERE TRAUMATIC BRAIN INJURY A CASE REVIEW

7
PRIMARY SURVEY Intubated-not initiating RR Severe dysoxygenation-PaO2 mid 80’s on 100% FIO2 PEEP 14 Extremities cold pale/flaccid; peripheral pulses weak- Temp 32.3 HR 134ST BP 93/66 Pupils 6mm fixed, dilated, non reactive Without corneal reflex

8
SECONDARY SURVEY No other obvious trauma Unknown PMH/PSH/Allergies/Medications Social Hx: Yale graduate student-english speaking; mother and father live in Japan and speak Mandarin Non smoker

12
Recovery From SDH The mortality rate for patients with an acute SDH ranges from 50 percent to 90 percent. A significant percentage of these deaths result from the underlying brain injury and pressure on the brain that develops in the days after injury. Approximately 20 percent to 30 percent of patients will recover full or partial brain function. Postoperative seizures are relatively common in these patients. Favorable outcomes are most common in patients who receive rapid treatment, younger adults, patients with a GCS score above 6 or 7 and reactive pupils, and those without multiple cerebral contusions or unmanageable pressure on the brain.

13
LAB DATA WBC 5.2Hgb 14.0Plt 269 INR 1.2PTT37 Na 140K2.5Cl 109 Cr 0.6BUN 12Glu 238 ABG: ph 7.15 pCO2 56 PaO245 Bicarb 18.8BE (-) 10.1
 10.1")
16
ARRIVAL To ICU Active Issues Severe TBI/s/p Craniectomy Diabetes Insipidus SIRS/Distributive Shock Neurogenic pulmonary edema vs aspiration pneumonia Severe hypoxia Pulmonary Edema Anemia Thrombocytopenia Coagulopathy Metabolic Acidosis Hypokalemia/Hypernatremia/Hypocalcemia/Hyperglycemia

17
ICU CLINICAL EXAM T 30.2 HR132ST BP 94/42 SPO2 67-70% Pupils 1.5mm B; minimally reactive Intubated/Sedated on neuromuscular blockade Lungs rhonchorous Refractory hypoxia; High PEEP Mean airway pressures 60’s Abdomen distended Extremities Cold

18
DIAGNOSTIC DATA WBC 2.2Hgb 7.7Plt 80K INR 2.2PTT69 Fibrin 91 Na 144K3.5Cl 118 Osm 339Ca (i) 0.9Lactate 5.2 Echo-akinesis of base (stunned myocardium) EF 30% PA cath
 0.9Lactate 5.2 Echo-akinesis of base (stunned myocardium) EF 30% PA cath")
19
Understanding Basic’s of Resuscitation Normal Vital signs DO NOT indicate adequate resuscitation Low BP associated with worse outcome in TBI Need to measure Hgb, ABG, Lactate

20
Understanding Basic’s of Resuscitation Traumatic blood loss occurs in 5 compartments: chest, abdomen, extremities, retroperitoneum, and outside Crystalloid and retained intravascular volume is 5:1 FFP: PRBC ratio- 1:2 Avoid hemodilution Measure Ca (i) frequently Fluid resuscitation strategy evolving science
 frequently Fluid resuscitation strategy evolving science")
21
THE DEADLY TRIAD ACIDOSIS HYPOTHERMIA COAGULOPATHY

22
MANAGEMENT/DECISION MAKING Sedated; neuromuscular blockade Refractory hypoxia; High PEEP; Nitric oxide Multiple pressors-chronotrophy dependent for cardiac output Correcting lytes Bicarb gtt for persistent acidosis Started on hydrocortisone gtt Receiving warmed multiple blood products Warming blanket

23
Prognosis VERY POOR Unable to place ICP monitor d/t emergent closure

24
24 Hrs POST INJURY ICU DAY 2 Hemodynamics improving-off pressors and inotropic agents Swan dc’d Remains in Pressure Control ventilation With sedation and paralytic on board ICP bolt inserted for monitoring

25
72 Hrs POST INJURY ICU DAY 3 Hemodynamically stable Remains off pressors and paralytics Remains on vent support ICP within target range Pupils bilaterally reactive + left corneal reflex No cough or gag No response to noxious stimuli

26
72 Hrs POST INJURY ICU DAY 3 MRI-suggestive of bilateral anterior communicating artery and significant diffuse patchy damage throughout cortex and deep brain structures C-spine MRI-without injury

27
7 Days Post Injury Family Meeting Held

28
10 Days Post Injury Trach and Peg placed Now with cough reflex Opened one eye ICP Bolt dc’d Withdraws extremities to noxious stimuli On antibiotics for hospital acquired Pneumonia

29
22 Days Post Injury Neuro unchanged Still with trach/peg Weaned from Vent Placed on amantadine and aricept for neurostimulation Transferred to NSCU

30
37 Days Post Injury Transferred to Yale New Haven Hospital Neuro unchanged

Similar presentations