Download presentation
Presentation is loading. Please wait.

1
Mineralocorticoid Excess Hyperaldostronism

2
Epidemiology first description of a patient with an aldosterone-producing adrenal adenoma (Conn's syndrome) mineralocorticoid excess was thought to represent a rare cause of hypertension a much higher prevalence is now recognized, ranging from 5 to 12% The prevalence is higher when patients are preselected for hypokalemic hypertension
 mineralocorticoid excess was thought to represent a rare cause of hypertension a much higher prevalence is now recognized, ranging from 5 to 12% The prevalence is higher when patients are preselected for hypokalemic hypertension")
3
The most common cause of mineralocorticoid excess is primary hyperaldosteronism, reflecting excess production of aldosterone by the adrenal zona glomerulosa.

4
Causes of Mineralocorticoid Excess

5
Etiology Bilateral micronodular hyperplasia is more common than unilateral adrenal adenomas Bilateral adrenal hyperplasia is usually micronodular but can also contain larger nodules that might be mistaken for a unilateral adenoma. rare instances, caused by an adrenocortical carcinoma.

6
Causes of Mineralocorticoid Excess

7
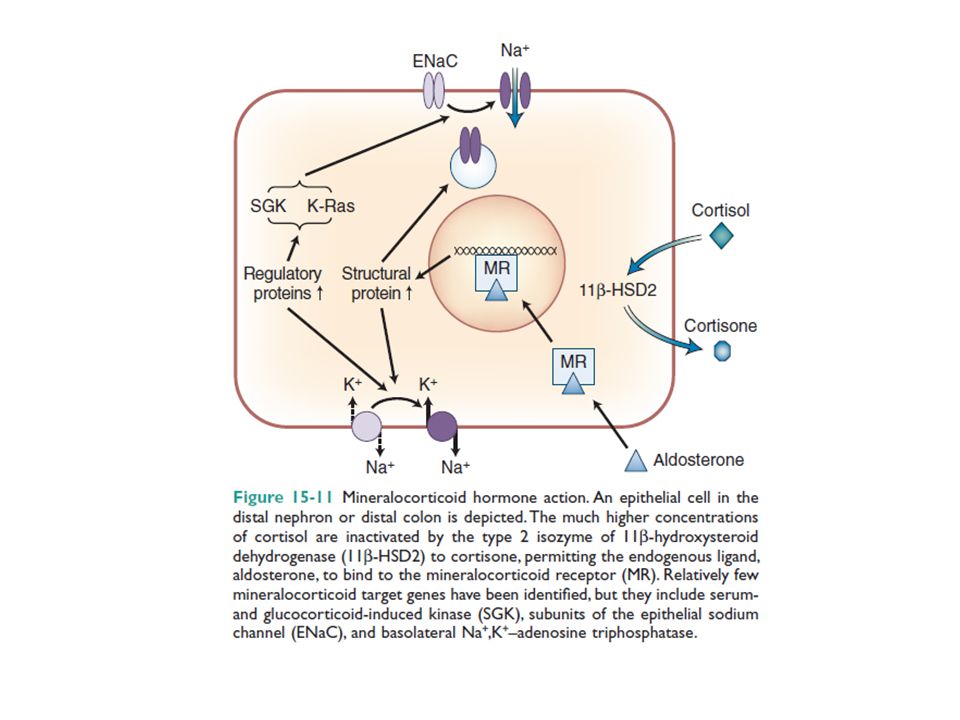
Clinical Manifestations Excess activation of the mineralocorticoid receptor leads to potassium depletion and increased sodium retention, with the latter causing an expansion of extracellular and plasma volume. Increased ENaC activity also results in hydrogen depletion that can cause metabolic alkalosis.

8
Aldosterone also has direct effects on the vascular system, where it increases cardiac remodeling and decreases compliance. Aldosterone excess may cause direct damage to the myocardium and the kidney glomeruli, in addition to secondary damage due to systemic hypertension.

11
The clinical hallmark of mineralocorticoid excess is hypokalemic hypertension serum sodium tends to be normal due to the concurrent fluid retention, which in some cases can lead to peripheral edema. Hypokalemia can be exacerbated by thiazide drug treatment, which leads to increased delivery of sodium to the distal renal tubule, thereby driving potassium excretion.

12
Severe hypokalemia can be associated with 1.muscle weakness 2.overt proximal myopathy 3.even hypokalemic paralysis Severe alkalosis contributes to muscle cramps and, in severe cases, can cause tetany

13
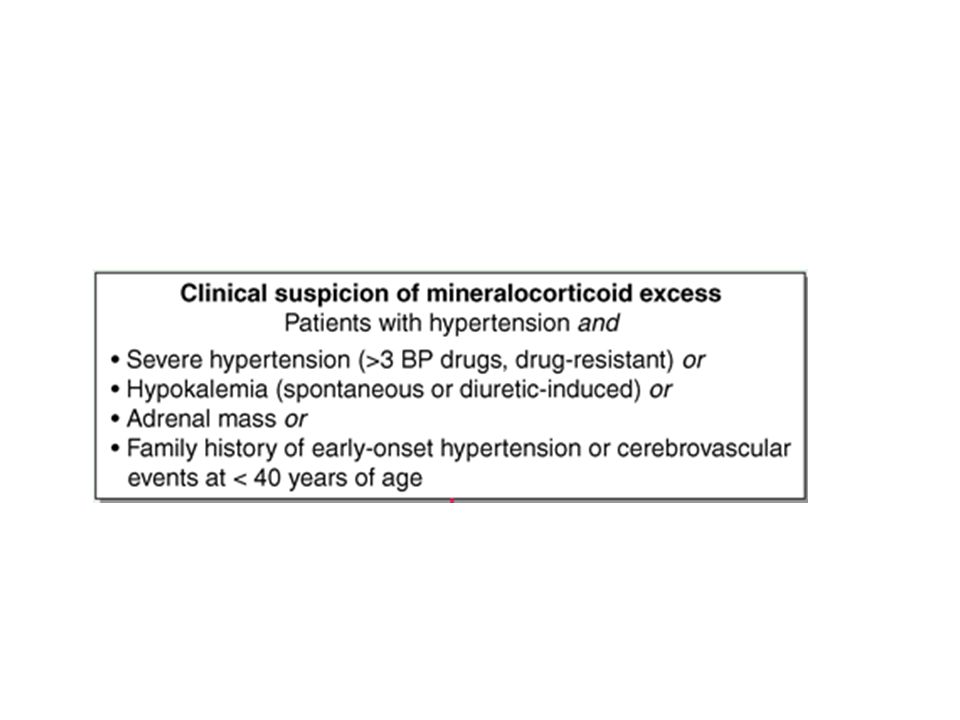
Diagnosis should be restricted to those who exhibit 1.hypertension associated with drug resistance 2.Hypokalemia 3.an adrenal mass 4.hypertension before the age of 40 years

16
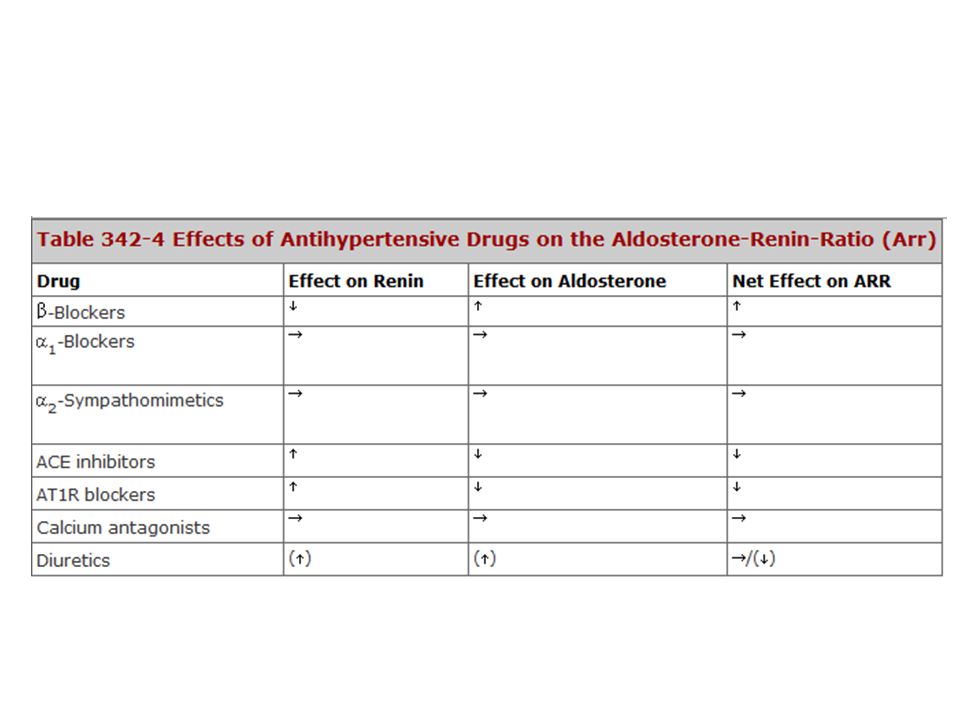
The accepted screening test is concurrent 1.measurement of plasma renin and aldosterone 2.calculation of the aldosterone-renin ratio (ARR) serum potassium needs to be normalized prior to testing.
 serum potassium needs to be normalized prior to testing.")
17
Screening

19
Confirmatory Tests

20
Intravenous Saline Infusion Test Two liters of 0.9% sodium chloride solution is infused intravenously with an infusion pump over 4 hours with the patient recumbent. Blood pressure and heart rate are monitored during the infusion. At the completion of the infusion, blood is drawn for measurement of PAC. 1.normal subjects :PAC levels decrease to less than 5 ng/dL, 2.primary aldosteronism : more than 10 ng/dL. 3.Indeterminate : PAC values between 5 and 10 ng/dL

21
Oral Sodium Loading Test hypertension and hypokalemia controlled high-sodium diet (supplemented with sodium chloride tablets if needed) for 3 days, with a goal sodium intake of 5000 mg (equivalent to 218 mEq of sodium or 12.8 g sodium chloride On the third day of the highsodium diet, a 24-hour urine specimen is collected for measurement of aldosterone, sodium, and creatinine. Urinary aldosterone excretion of more than 12 μg/24 hours is consistent with autonomous aldosterone secretion

22
Fludrocortisone Suppression Test fludrocortisone acetate is administered for 4 days (0.1 mg every 6 hours) in combination with sodium chloride tablets (2 g three times daily with food). Blood pressure and serum potassium levels must be monitored daily. In the setting of low PRA, failure to suppress the upright 10 a.m. PAC to less than 6 ng/dL on day 4 is diagnostic of primary aldosteronism

23
Localization

26
Adrenal Venous Sampling cortisol-corrected aldosterone lateralization ratios greater than 4.0: unilateral source of aldosterone like APA 95% sensitivity and 100% specificity zone of overlap :ratios greater than 3.0 but less than 4.0 represent bilateral aldosterone secretion : Ratios less than 3.0

27
Treatment Patients younger than 40 years with confirmed mineralocorticoid excess and a unilateral lesion can go straight to surgery Laparoscopic adrenalectomy is the preferred approach. Patients who are not surgical candidates, or with evidence of bilateral hyperplasia based on CT or AVS, should be treated medically

28
Medical treatment mineralocorticoid receptor antagonist Spironolactone: started at 12.5–50 mg bid and titrated up to a maximum of 400 mg/d to control blood pressure and normalize potassium. Side effects include 1.menstrual irregularity 2.decreased libido 3.gynecomastia eplerenone : more selective MR antagonist. Doses start at 25 mg bid and it can be titrated up to 200 mg/d.

29
Another useful drug is the sodium channel blocker amiloride (5–10 mg/bid).
.")
Similar presentations
















 of urine.>")





>")

 glucocorticoids (2)mineralocorticoids (3) adrenal androgens.>")