Download presentation
Presentation is loading. Please wait.

1
Urinalysis Belinda Jim, MD July 17, 2009

2
Urinalysis Major noninvasive tool Provide information about disease severity, though not always a direct relationship Specimen should be examined about 30-60 minutes of voiding Sample centrifuged at 3000 rpm for 3-5 minutes, supernatant be tested by dipstick

3
Color Normal color is clear and light yellow White- pyuria or phosphate crystals Green- administration of methylene blue, amitriptyline, propofol Red or Brown- due to blood

4
Turbidity Normal urine should be clear Turbidity indicates: cellular material bacteria protein lipids crystals salt precipitation

5
Odor Normal odor is urinoid Ammonia- related to UTI, prolonged urinary retention Sweetish- diabetic ketoacidosis due to acetone Sulfuric- cysteine decomposition Drugs/Foods- e.g. antibiotics, asparagus

6
Test Reagent Strip

7
Protein Detects primarily albumin Highly specific, but not sensitive Positive only when protein excretion > 300- 500 mg/day Not good to detect microalbuminuria or immunoglobulin light chains

8
Sulfosalicylic acid test (SSA) SSA detects all proteins in the urine Especially useful if suspects multiple myeloma in which immunogloblin light chains form casts that obstruct the tubules A positive SSA test in conjunction with a negative dipstick indicates presence of non-albumin proteins in urine Mix 1 part urine supernatant with 3 parts SSA (3%), grade its turbidity
 SSA detects all proteins in the urine Especially useful if suspects multiple myeloma in which immunogloblin light chains form casts that obstruct the tubules A positive SSA test in conjunction with a negative dipstick indicates presence of non-albumin proteins in urine Mix 1 part urine supernatant with 3 parts SSA (3%), grade its turbidity")
9
pH Reflects degree of acidification of urine Urine pH ranges from 4.5 to 8.0 Major clinical use for patient with metabolic acidosis Appropriate response to increase urinary acid excretion, with urine pH falling below 5.3 A higher value indicate presence of RTA or infection

10
Ketones Detects acetone and acetoacetate using nitroprusside reaction Does not detect -hydroxybutyrate Presence in the urine indicates diabetic ketoacidosis, starvation ketosis, low carb diet

11
Bilirubin/Urobilinogen Normal bilirubin not detected in urine If increased conjugated bilirubin in urine, indicates liver dysfunction Bilirubin metabolized by bacteria in the intestines to form urobilins Small % absorbed in intestine and appears in urine

12
Osmolality and specific gravity Osmolality- number of solute particles per unit volume Specific gravity- weight of solution compared with weight of water –Generally varies with osmolality, though presence of large molecules in urine, such as glucose or radiocontrast media can produce large changes in specific gravity with little changes in osmolality

13
Glucose Presence of glucose indicates inability to reabsorb filtered glucose in the proximal tubule despite normal plasma levels OR urinary spillage due to abnormally high plasma concentrations Generally glucosuria does not occur until plasma glucose exceeds 180 mg/dL

14
Hematuria and Pyuria Dipsticks very sensitive in detecting rbc’s, as few as 1 to 2 rbc’s per high power field Detect leukocyte esterase (pyuria) and nitrite (enterobacteriaceae converts nitrate to nitrite) Sterile pyuria: interstitial nephritis, renal tuberculosis, and nephrolithiasis
 and nitrite (enterobacteriaceae converts nitrate to nitrite) Sterile pyuria: interstitial nephritis, renal tuberculosis, and nephrolithiasis")
15
Urine sediment Crystals Bacteria Red blood cells (0-2 rbc’s in normal) White blood cells (0-4 wbc’s) Casts Artifact
 White blood cells (0-4 wbc’s) Casts Artifact")
16
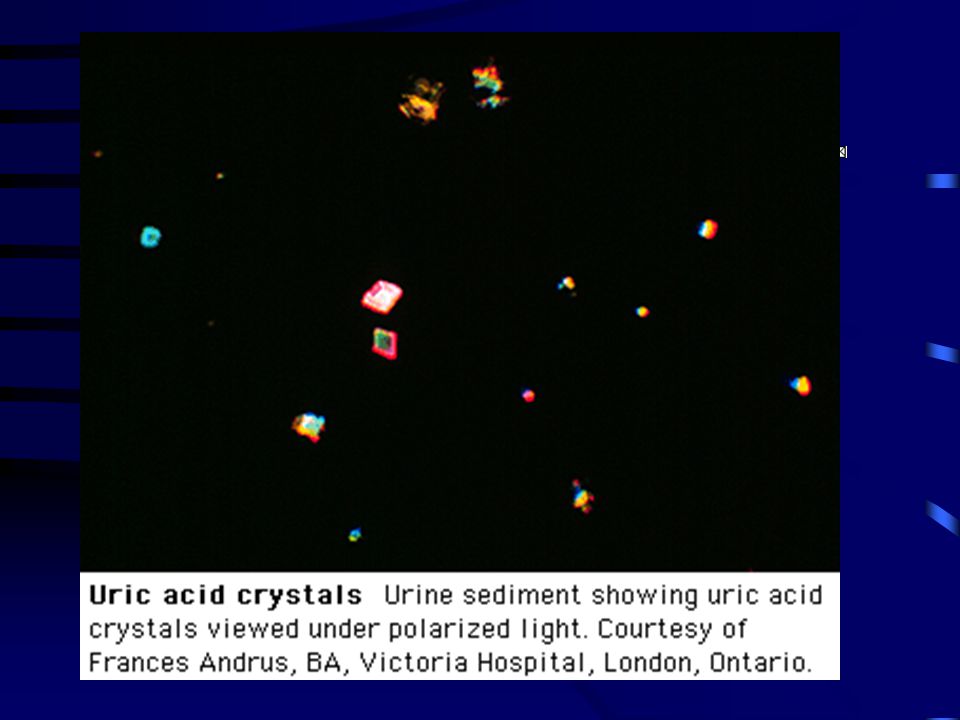
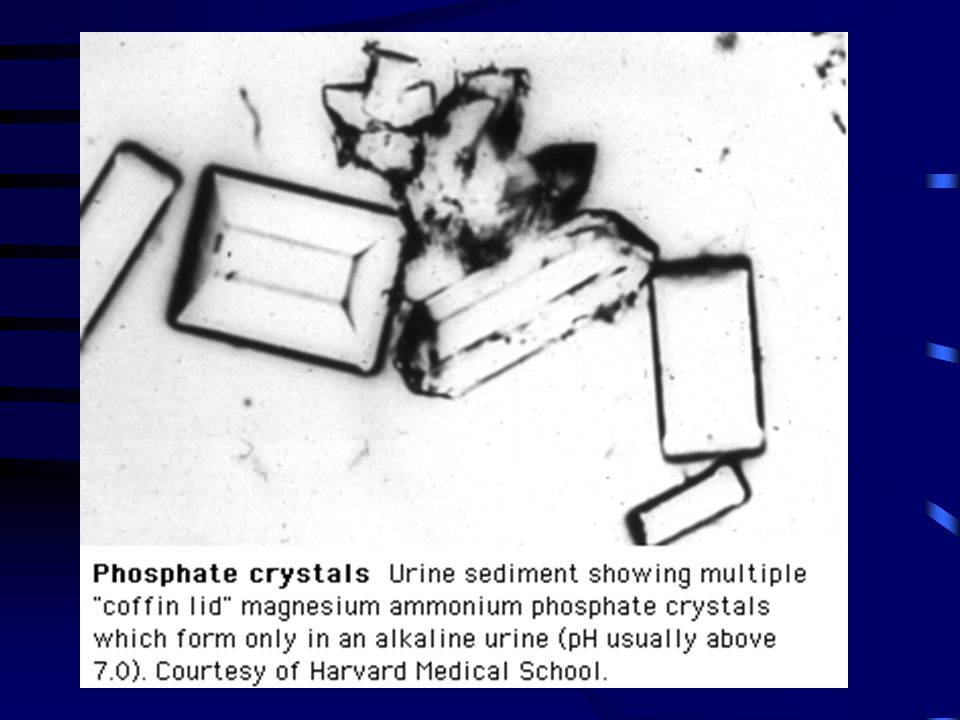
Crystals Calcium phosphate or calcium oxalate crystals Uric acid crystals Magnesium ammonium phosphate crystals Cystine crystals

23
Bacteria Significance depends on quality of collection More significant in presence of wbc’s and other elements Urine in the bladder should be sterile, but becomes contaminated as it passes through bladder

25
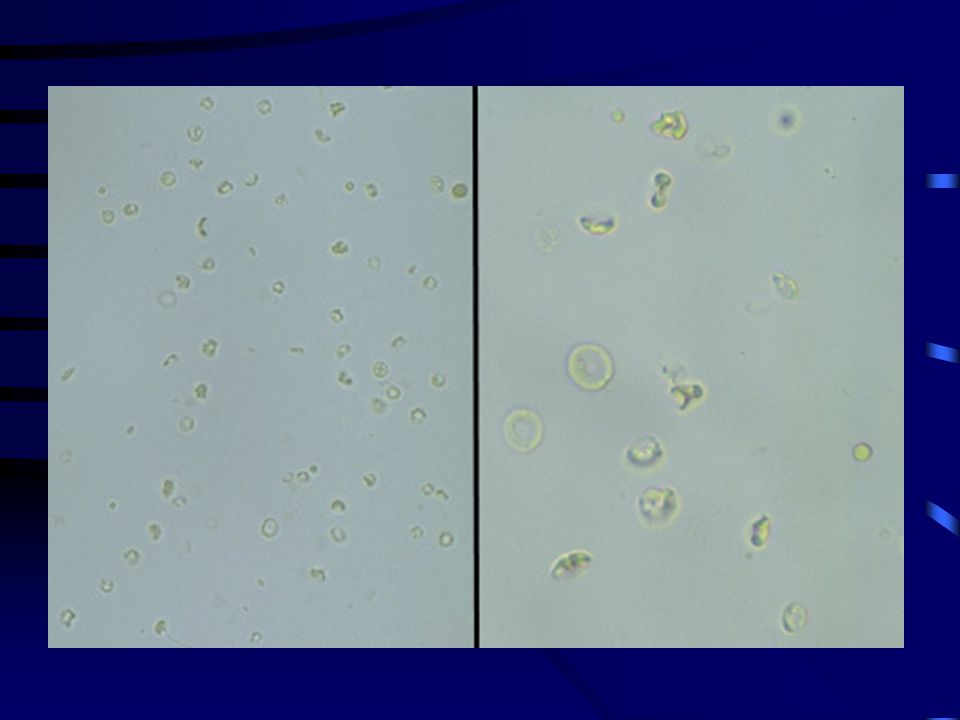
Hematuria Transient hematuria - relatively common in young subjects, not indicative of disease Persistant hematuria- gross or microscopic –Morphology is important, usually uniform and round with extrarenal bleeding –Dysmorphic appearance with renal lesions, I.e. blebs, budding, segmental loss of membrane

29
Pyuria White cells are larger than red cells, granular cytoplasm and multilobed nuclei Pyuria alone usually indicated infection Less diagnostic value when seen with other elements such as cellular casts, and/or proteinuria Eosinophils may indicate allergic interstitial nephritis, cholesterol emboli disease Lymphocytes seen in disorders associated with infiltration of kidney by lymphocytes, such as chronic tubulointerstitial disease

31
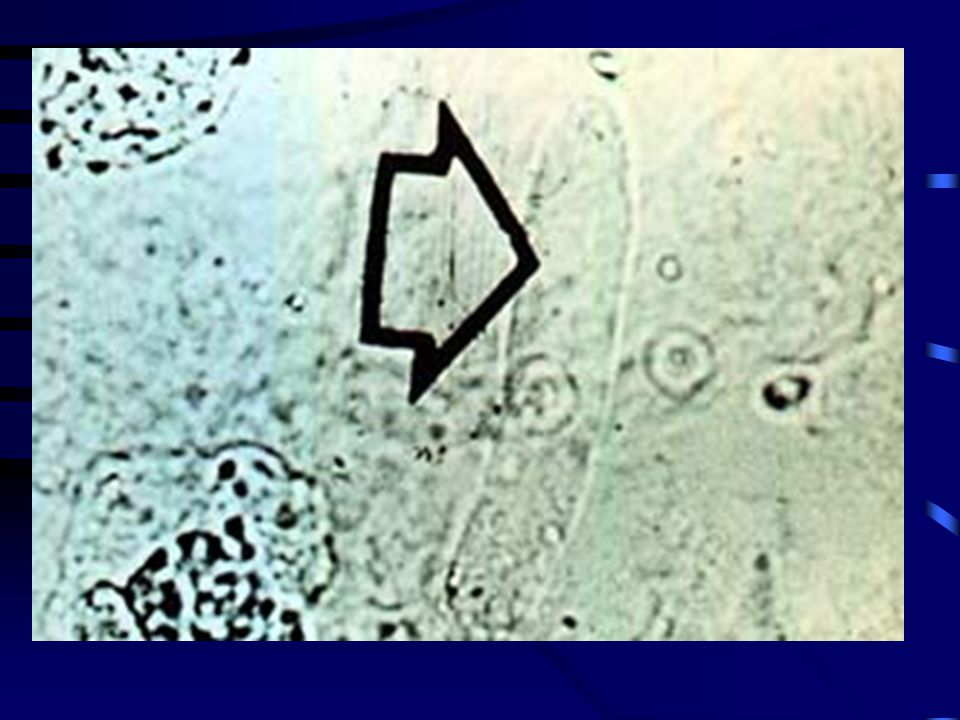
Epithelial Cells May be shed anywhere within the GU tract Only renal tubular cells are significant Generally 1.5 to 3 times larger than white cells, contain a round, large nucleus May be normal or indicative of ATN, pyelonephritis, nephrotic syndrome

34
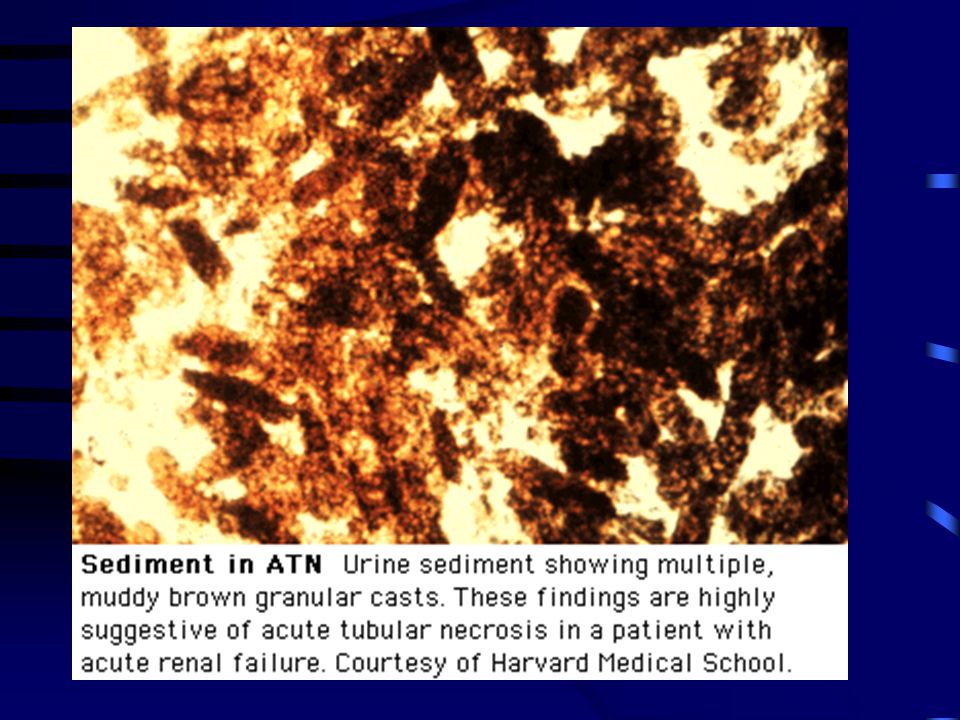
Casts Conform to the shape of the renal tubule in which they form Organic matrix composed mostly of Tamm- Horsfall mucoprotein Types of casts: hyaline, red cell, white cell, epithelial, granular, waxy, broad

35
Theory of Casts Genesis Key: A = Cellular casts B = Coarsely granular cast C = Finely granular cast D = Waxy cast

38
RBC cast

41
©2005 UpToDate ® e-mail this to a colleaguemail this to a colleague

45
Miscellaneous Findings

46
Trichomonas Vaginalis

47
Sperm

48
Talc

49
Fiber

50
Case 1 A 46 y.o. man with HTN presents with acute right flank pain that moves around. He is slightly febrile to 100.4 C. Exam unremarkable. UA shows hematuria.

52
Case 2 A 22 y.o. woman with no significant past medical history presents with dysuria, ammonia-smelling urine and increased urinary frequency for 3 days. What will her UA show? What do you expect on the urine sediment?

55
Case 3 A 57 y.o. woman with h/o poorly controlled HTN and DM, diabetic retinopathy presents with creatinine of 1.8 and lower extremity edema. What would you expect your UA to show? What would you do next?

56
Case 4 A 3-year old boy brought to pediatrician for increasing facial and peripheral edema of eight days duration. Urine- 4.2 grams protein/24 hours, cholesterol 450 mg/dl, albumin 3.0 g/dl

58
Case 5 A 45-year old man hospitalized for peripheral edema and proteinuria. Urine-6 g protein/24 hours, albumin 1.6 g/dl. Cholesterol 380 mg/dl. Creatinine 1.6. Review of medical records showed he had 1+ proteinuria four years previously.

60
Case 6 A 52-year old woman with sudden onset of edema, “dark urine”, headaches, malaise. BP: 150/105, urine 900 cc/24 hr, 1.7g protein/24 hours, creatinine 4.5 mg/dl, BUN 68 mg/dl. Review of records show that she had normal renal function 1 month ago.

Similar presentations

























; Small mwt proteins (such as peptide hormones,Insulin glucagon, growth hormone) can appear.>")






 The sample must be tested within 1hr.>")


 –Urea (from amino acids) –Creatinine (from muscle creatine.>")




