Download presentation
Presentation is loading. Please wait.

1
Gastric and duodenal ulcer disease

2
Ulcer disease ulcer is a defect of gastric or duodenal mucosa which interfere over lamina muscularis mucosae, submucosa or penetrates across whole gastric or duodenal wall rise of ulcer is conditioned by presence of acid gastric content frequent disease, men are afected 3-4x more than women

3
Pathogenesis: multifactorial
dysbalance between protective and aggressive factors Protective f.: saliva, food, alcalic duodenal fluid, mucus - mucine, fast regeneration of gastric epithelial cells, well perfused gastric mucosa Aggressive f.: HCl, pepsin, bile acids (reflux), helicobacter pylori, drugs (analgetics, aspirin, korticoids), nicotine, alcohol
, helicobacter pylori, drugs (analgetics, aspirin, korticoids), nicotine, alcohol.")
4
Classification: Acute ulcer (ulcus acutum)
smooth non-elevated borders and smooth base major bleeding into upper GIT Chronic ulcer (ulcus chronicum) rushed and elevated boders, inflammation with hypertrophic and fibrotic proliferation is present the most frequent form of ulcer disease Ulcus chronicum mediogastricum Ulcus chronicum ventriculi et duodeni Ulcus chronicum praepyloricum Ulcus chronicum duodeni
 rushed and elevated boders, inflammation with hypertrophic and fibrotic proliferation is present. the most frequent form of ulcer disease. Ulcus chronicum mediogastricum. Ulcus chronicum ventriculi et duodeni. Ulcus chronicum praepyloricum. Ulcus chronicum duodeni.")
5
Symptoms of gastric ulcer disease:
epigastric pain after meal or during meal upper dyspeptic syndrome – loss of appetite, nauzea, vomiting, flatulence vomiting brings relief reduced nutrition loss of weight

6
Symptoms of duodenal ulcer disease:
epigastric pain 2 hours after meal or on a empty stomach or during night pyrosis good nutrition obstipation seasonal dependence (spring, autumn)
")
7
Complications: Bleeding - chronic (minor, cause anaemia)
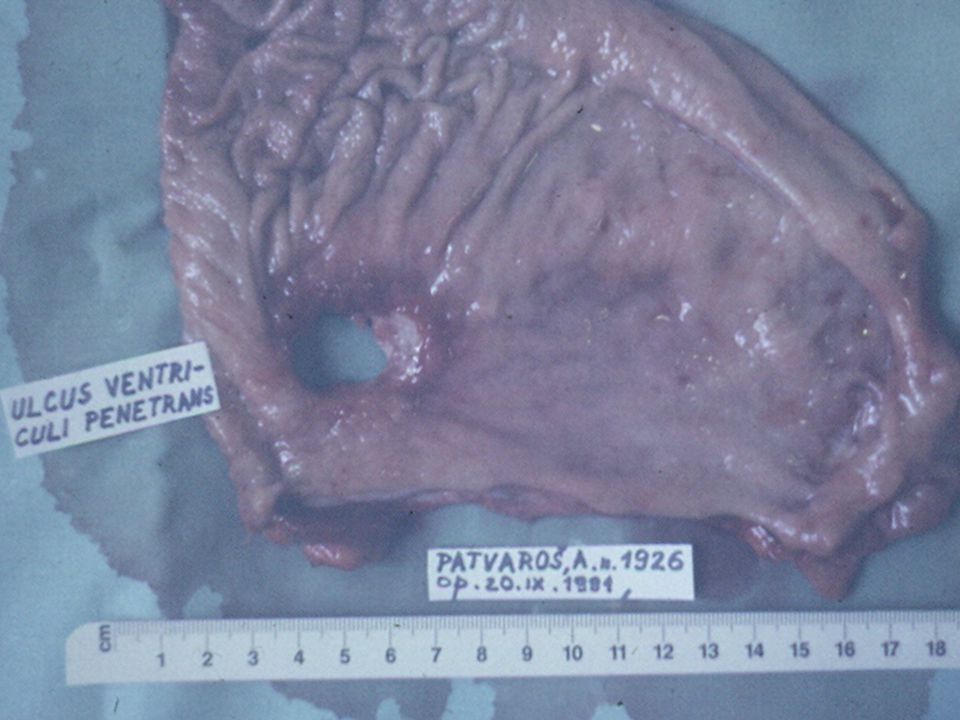
- acute (major, form affected vessel) Perforation - mostly bulbus duodeni, anterior gastric wall - acute violent pain - bleeding can be present Penetration - of the ulcer deeply through whole wall into neighbor organ (pancreas, liver) Stenosis - narrow of the lumen caused by scar, oedema or inflammatory infiltration after healing of the ulcer - rise only at pyloric localization - vomiting of huge volume of gastric content
 Perforation - mostly bulbus duodeni, anterior gastric wall. - acute violent pain. - bleeding can be present. Penetration - of the ulcer deeply through whole wall into. neighbor organ (pancreas, liver) Stenosis - narrow of the lumen caused by scar, oedema or. inflammatory infiltration after healing of the ulcer. - rise only at pyloric localization. - vomiting of huge volume of gastric content.")
8
A – penetration B – perforation C – bleeding D - stenosis
Zeman, M. et al., Speciální chirurgie, ISBN , 2004 A – penetration B – perforation C – bleeding D - stenosis

9
Therapy: Conservative Surgical regular lifestyle
prohibition of the smoking and alcohol diet (proteins, milk and milky products) pharmacology (antagonists of H2 receptors, antacids, anticholinergics Surgical BI, BII resection proximal selective vagotomy vagotomy with pyloroplastic suture of perforated or haemorrhagic ulcer
 pharmacology (antagonists of H2 receptors, antacids, anticholinergics. Surgical. BI, BII resection. proximal selective vagotomy. vagotomy with pyloroplastic. suture of perforated or haemorrhagic ulcer.")
10
Stomach resections: Billroth I (BI) – gastro-duodenoanastomosis end-to-end Billroth II (BII) – gastro-jejunoanastomosis end-to-side with blind closure of duodenum Proximal selective vagotomy – denervation of parietal gastric cells
 – gastro-jejunoanastomosis end-to-side with blind closure of duodenum. Proximal selective vagotomy – denervation of parietal gastric cells.")
11
Zeman, M. et al., Speciální chirurgie, ISBN 80-7262-260-9, 2004
Billroth I

12
Zeman, M. et al., Speciální chirurgie, ISBN 80-7262-260-9, 2004
Billroth II

13
Gastro-enteroanastomosis on Roux Y crankle
Zeman, M. et al., Speciální chirurgie, ISBN , 2004 Gastro-enteroanastomosis on Roux Y crankle

14
Zeman, M. et al., Speciální chirurgie, ISBN 80-7262-260-9, 2004
Vagotomy

15
Complications after stomach resection:
Early – dehiscence, stenosis of anastomosis, bleeding, pancreatitis, obstructive icterus, affection of neighbour tissues Late - days, weeks - early dumping syndrome - late dumping syndrome - incoming crankle syndrome - outcoming crankle syndrome - ulcer in anastomosis or in outcoming crankle

16
Early dumping syndrome:
group of symptoms approved shortly after meal appears after BII resection vasomotoric sy. - face redness, fall of blood pressure, dizziness GI sy. - vomiting, diarrhoea Th.: diet, no sugar, low quantities of food, change BII to BI resection

17
Late dumping syndrome:
hypoglycaemia (sugar is not enough digested) appears after BII resection weakness, perspiration, dizziness, tremor cca 3h after meal Th.: no sugar, change BII to BI resection
 appears after BII resection. weakness, perspiration, dizziness, tremor cca 3h after meal. Th.: no sugar, change BII to BI resection.")
18
Incoming crankle syndrome:
stasis of the content at incoming crankle increase intraluminal pressure appears after BII resection Th.: diet, change BII to BI resection

19
Outcoming crankle syndrome:
chronic or acute closure of outcoming crankle appears after BII resection vomiting after meal, convulsive pain Th.: change BII to BI resection

25
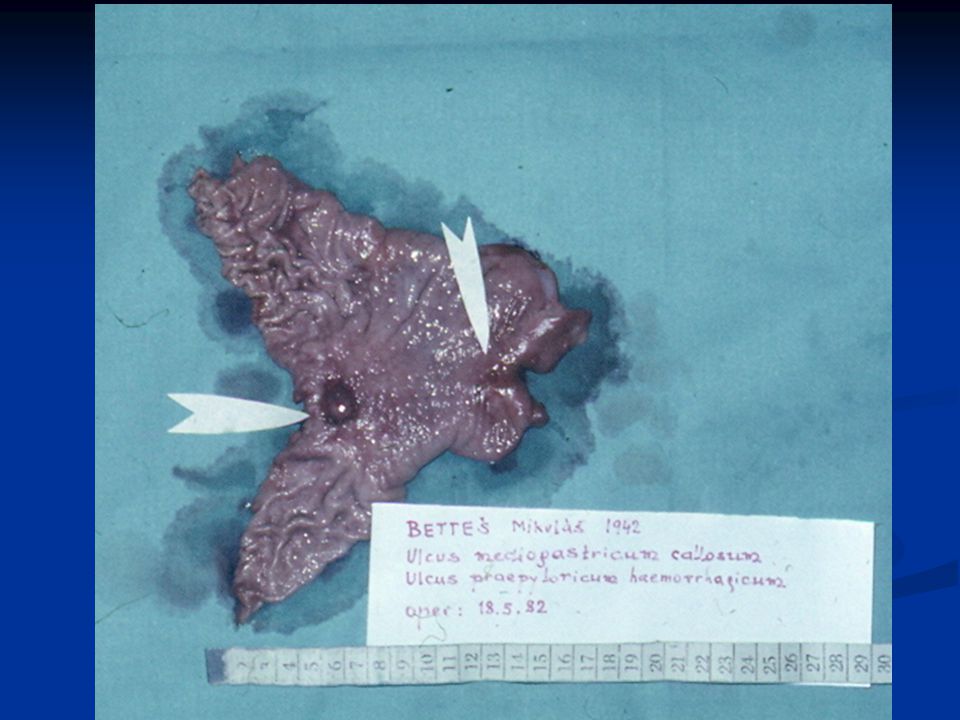
Haemorrhagic mediogastric ulcer

27
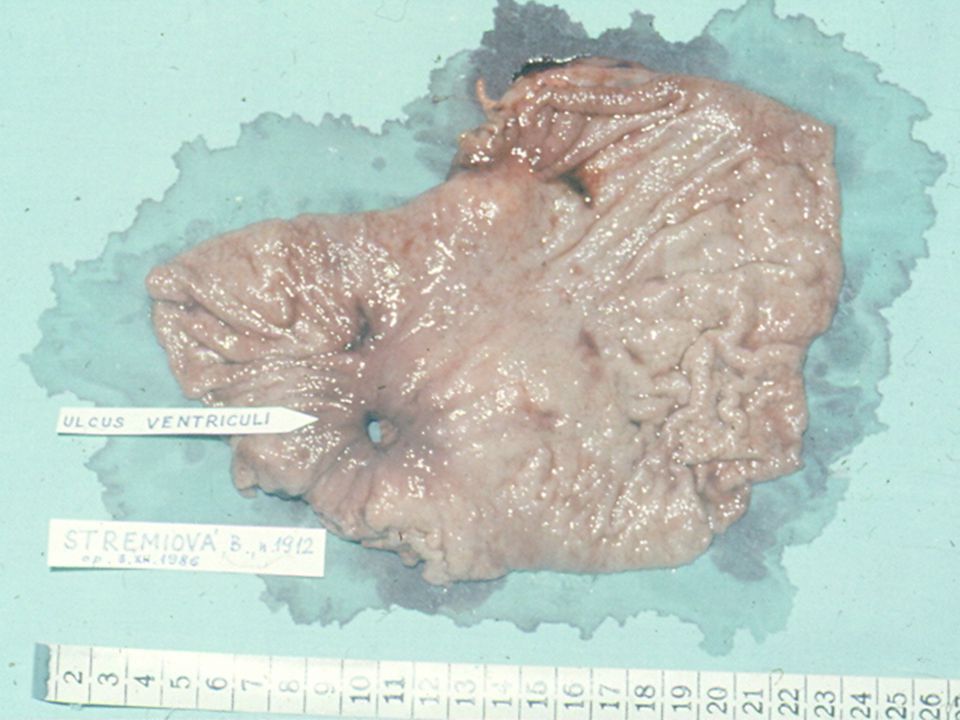
Chronic gastric ulcer

34
Pylorostenosis and gastrectasia

35
Duodenal ulcer

36
Stress ulcers

38
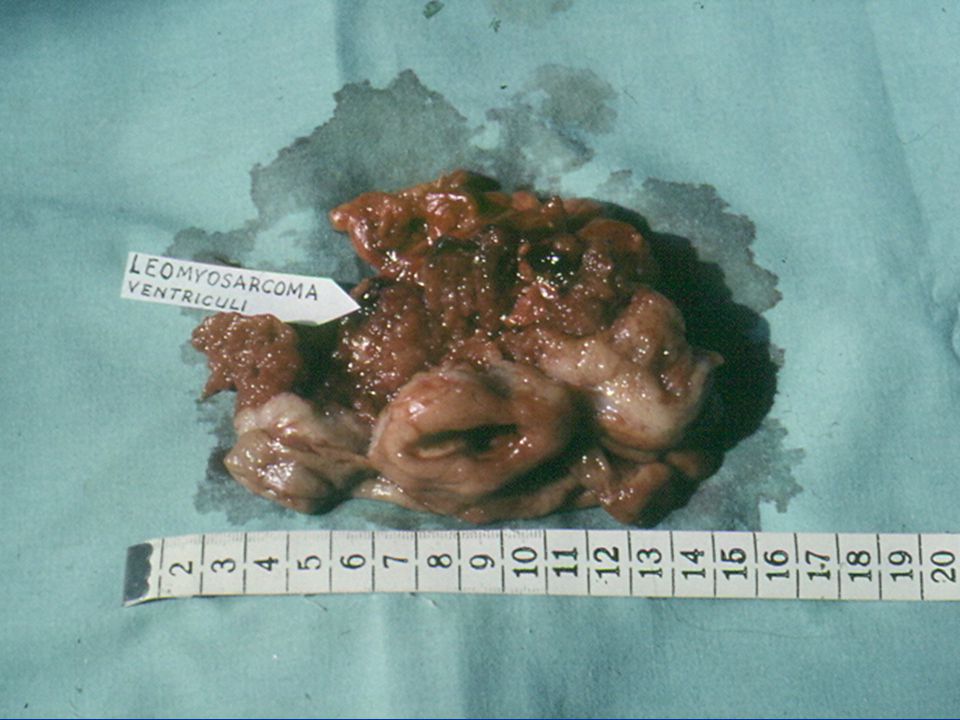
Benign stomach tumors rise from all layers of stomach wall
often asymptomatic Polypus, Leiomyoma, Lipoma, Fibroma, Neurofibroma, Neurinoma, Hemangioma, Karcinoids, Lymfoma Diagnostic: endoscopy, X – ray Therapy: local excision, stomach resection

39
Stomach cancer Symptoms: Diagnosis: long-time asymptomatic
feeling of full stomach, odour from mouth, tiredness, anaemia, occasional vomiting, loss of appetite, loss of weight Diagnosis: gastrofibroscopy – biopsy - histology X-ray, USG, CT - metastasis Wirchow´s nodule – enlargement of left supraclavicular nodule

40
Stomach cancer Etiopathogenesis: Division:
Praecancerosis: adenomatous polypus, chronic atrofic gastritis, foveolar hyperplasia (Ménétrier disease), stub of the stomach after BII resection Division: Macroscopic: exofytic polypoid form, diskyform ulcerous form, diffused infiltrating form Histopathologic: adenocarcinoma, papilar, tubular, gelatinous cancer, round cell cancer, flagstone cell cancer, etc.
, stub of the stomach after BII resection. Division: Macroscopic: exofytic polypoid form, diskyform ulcerous form, diffused infiltrating form. Histopathologic: adenocarcinoma, papilar, tubular, gelatinous cancer, round cell cancer, flagstone cell cancer, etc.")
41
Stomach cancer Therapy:
Zeman, M. et al., Speciální chirurgie, ISBN , 2004 Therapy: Currative – total gastrectomy, sub-total gastrectomy Paliative – gastrostomy, jejunostomy

49
Gastric cancer

50
Gastric stub cancer after B II resection

52
Schwanoma fundi vetriculi

56
Than you for your attention!!!

Similar presentations


























>")
![Peptic Ulcer Disease Dr Maha Arafah. Objectives Upon completion of this lecture the students will : A] Understand the Pathophysiology of acute and chronic.](/13/3809458/big_thumb.jpg "Peptic Ulcer Disease Dr Maha Arafah. Objectives Upon completion of this lecture the students will : A] Understand the Pathophysiology of acute and chronic.>")



>")
 Dr. Gehan Mohamed Dr. Abdelaty Shawky.>")






