Download presentation
Presentation is loading. Please wait.

1
Latent Infection of Tuberculosis in China HUASHAN HOSPITAL, FUDAN UNIVERSITY, Shanghai, China Wenhong Zhang, M.D & PhD.

2
TB: A leading infectious killer - top 3 infectious killer TB kills about 2 million people each year 8 million people become sick with TB each year TB is the leading killer of HIV/AIDS patients 50 million people infected with drug-resistant TB

3
The New Tuberculosis HIV and Drug-resistant TB – A lethal combination and a major threat to TB control WHO declared TB a global emergency in 1993

4
TB Chemotherapy: THE Effective TB Control Pre-antibiotic era: before 1940s (e.g., cod liver oils, bed rest, fresh air) Drugs used to treat TB: Streptomycin first TB drug (1944), followed by PAS (1946), isoniazid (1952), pyrazinamide (1952), rifampin (1963) (a) Front-line Drugs: isoniazid (INH) rifampicin (RMP), pyrazinamide (PZA), streptomycin, ethambutol. (b) Second-line Drugs: PAS, kanamycin, cycloserine, ethionamide, thiacetazone, ciprofloxacin/ofloxacin, rifapentine, amikacin, viomycin, capreomycin.
 Second-line Drugs: PAS, kanamycin, cycloserine, ethionamide, thiacetazone, ciprofloxacin/ofloxacin, rifapentine, amikacin, viomycin, capreomycin..")
5
DOTS-The Best TB Therapy since 1991 DOTS: 6 month therapy - The best therapy against TB (78%-96% cure rate). Initial phase (daily, 2 months) with 4 drugs: INH, RMP, PZA, Ethambutol. Continuation phase (3 times a week, 4 months) with 2 drugs: INH and RMP.
 with 4 drugs: INH, RMP, PZA, Ethambutol. Continuation phase (3 times a week, 4 months) with 2 drugs: INH and RMP..")
6
DOTS-Plus DOTS + second-line TB drugs (PAS, ethionamide, cycloserine, kanamycin, amikacin etc.) Too expensive (TB case: $11 to $100, cost of treating an MDR-TB case: $150,000) MDR-TB requires extensive chemotherapy (also more toxic to patients- side effects) for up to two years DOTS-Plus works as a supplement to the DOTS, to address both drug-susceptible and MDR-TB in areas with significant MDR-TB.
 Too expensive (TB case: $11 to $100, cost of treating an MDR-TB case: $150,000) MDR-TB requires extensive chemotherapy (also more toxic to patients- side effects) for up to two years DOTS-Plus works as a supplement to the DOTS, to address both drug-susceptible and MDR-TB in areas with significant MDR-TB.")
7
Disease Burden of Tuberculosis in China, 2000 data Prevalence of active pulmonary diseases is 367 / 100,000 Prevalence of Sear positive pulmonary diseases is 122 / 100,000 130,000 patients die from tuberculosis every year No data of latent tuberculosis in China up to now China CDC 2006

8
Prevalence of Smear Positive Tuberculosis in China

9
Incidence of tuberculosis according to the report from China CDC But incidence do not decrease! 0 200000 400000 600000 800000 1000000 1200000 1400000 1600000 2003 200420052006 China CDC 2006

10
Factors contribute to tuberculosis reemerging in China MDR TB? HIV increasing? Latent infection? Diagnosis tools are more accurate to find more new cases?

11
HIV infected Tuberculosis Cases < 1/100,000 population in China

12
Latency TB bacilli can persist for long periods of time (decades) in the host before reactivating and causing active disease Host factors: immunocompromised conditions, viral infections (e.g. HIV and measles), steroids, anti-TNF antibody (REMICADE® infliximab) as part of the treatment of rheumatoid arthritis Bacterial factors: e.g. isocitrate lyase, alpha- crystallin, 48-gene dormancy regulon, etc.
, steroids, anti-TNF antibody (REMICADE® infliximab) as part of the treatment of rheumatoid arthritis Bacterial factors: e.g. isocitrate lyase, alpha- crystallin, 48-gene dormancy regulon, etc..")
13
Dormant or Persistent Bacilli Cornell model: Mice infected with TB bacilli are treated for 3 months with INH and PZA --> No bacilli found in infected organs (spleens/lungs) by plating --> stop treatment --> 3 months later, 1/3 mice relapse with TB (drug susceptible) and all mice relapse with TB if treated with immonosuppressing steroids --> suggest existence of dormant bacilli or persisters (phenotypic resistance).
 by plating --> stop treatment --> 3 months later, 1/3 mice relapse with TB (drug susceptible) and all mice relapse with TB if treated with immonosuppressing steroids --> suggest existence of dormant bacilli or persisters (phenotypic resistance).")
14
New TB cases are driven by the reservoir of latently infected people. If we want to stop active TB cases, we need to eliminate this reservoir of infection. This “hidden epidemic” of people infected with latent TB is enormous. The growth in latent TB is becoming a clinical time bomb. We need to defuse this bomb by increasing our efforts to identify and treat latently infected people. Latent tuberculosis is the reservoir of active tuberculosis Active TB – 8 million new cases a year - Unfortunately just the tip of the iceberg Latent TB - the “hidden epidemic” -2 billion people infected

15
Epidemiology of latent infection in the world Frothingham R, et al.International Journal of Infectious Diseases (2005) 9, 297—311
 9, 297—311")
16
45% 55% Infected No infection TST positive in China, 2000

17
Shortage of TST Poor specificity: antigenic cross-reactivity of PPD with BCG and environmental mycobacteria Poor sensitivity: 75-90% in active disease (lower in disseminated TB and HIV infection; unknown for latent infection)
")
18
Factors leading to False-Positive TST Reactions Nontuberculous mycobacteria –Reactions caused by nontuberculous mycobacteria are usually 10 mm of induration BCG vaccination –Reactivity in BCG vaccine recipients generally wanes over time; positive TST result is likely due to TB infection if risk factors are present

19
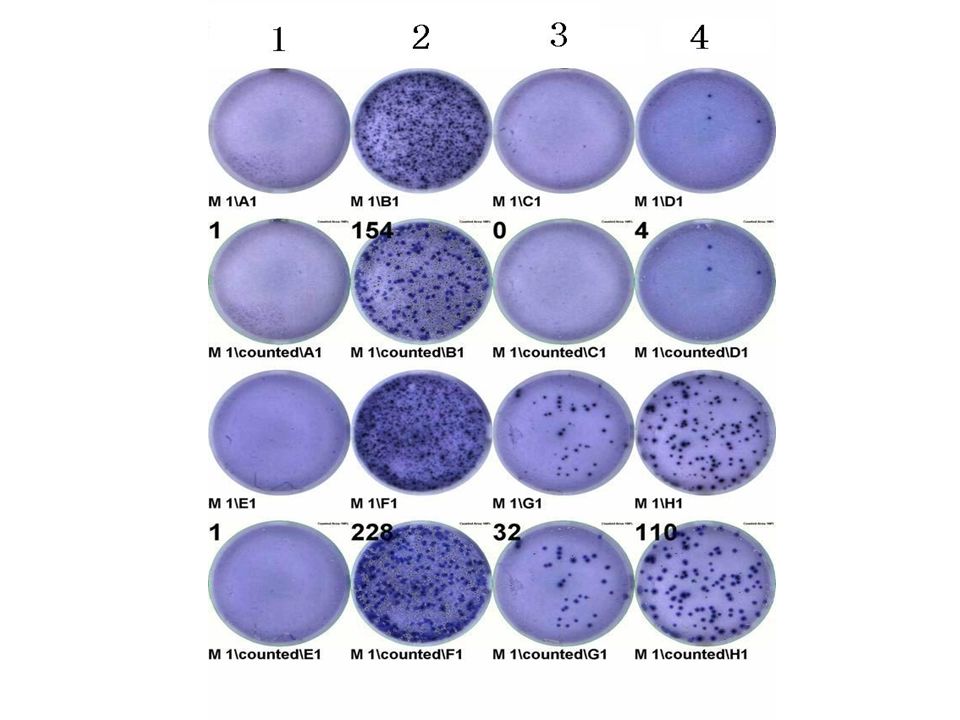
T SPOT TM detect INF-r released by specific T cells Collect white cells using BD CPT tube or Ficoll extraction.Add white cells and TB antigens to wells. T cells release interferon gamma. Interferon gamma captured by antibodies. Incubate, wash and add conjugated second antibody to interferon gamma. Add substrate and count spots by eye or use reader. Each spot is an individual T cell that has released interferon gamma.

20
How does T-spot Technology Work Patient Whole blood Sample PBMC ESAT-6 CFP10 T cell secreting INF Ab capture INF Blue spot

22
2 commercial Kit available for detecting latent or active tuberculosis T cell-based assay for interferon gamma, the enzyme-linked immunosorbent spot test (ELISPOT), has promise in the diagnosis of Mycobacterium tuberculosis infection after exposure to a known tuberculosis (TB) patient. Commercialisation of two T cellbased tests for the diagnosis of M. tuberculosis infection (T Spot TB by Oxford Immunotec and Quantiferon-TB Gold by Cellestis)
.")
23
T-cell based assay is recommended for detecting infection of M. Tb measures individual reacting T cells: –Even individual cells can be detected in a sample. –Therefore even those who are severely immunocompromised, if a single cell reacts then it can be detected. measures all types of T cells: –Both CD4 and CD8 type T cells are detected. –Therefore if one type of T cells is depleted in a patient (e.g. CD4 T cells in HIV infected patients) a response can still be detected from the CD8 T cells. This sensitivity is key to the test’s excellent performance in immunosuppressed populations
 a response can still be detected from the CD8 T cells. This sensitivity is key to the test’s excellent performance in immunosuppressed populations.")
25
The strategic for treating latent infection of tuberculosis in China?

26
Lifetime Risk of Reactivation Tuberculosis C. Robert Horsburgh. n engl j med 2004;350;20:2060-7

27
Latent infection of tuberculosis in China: Treat or not Treat? BCG strategic or “find and treat” strategic? Conditionally treatment focusing high-risk groups: close house contacts and immunocompromised cases Chemotherapy or Immunotherapy?

Similar presentations











 PHCL 442 Lab Discussion Jamilah Al-Saidan, M.Sc.>")
 Deputy Director.>")




 Randy Kim.>")


