Download presentation
Presentation is loading. Please wait.

1
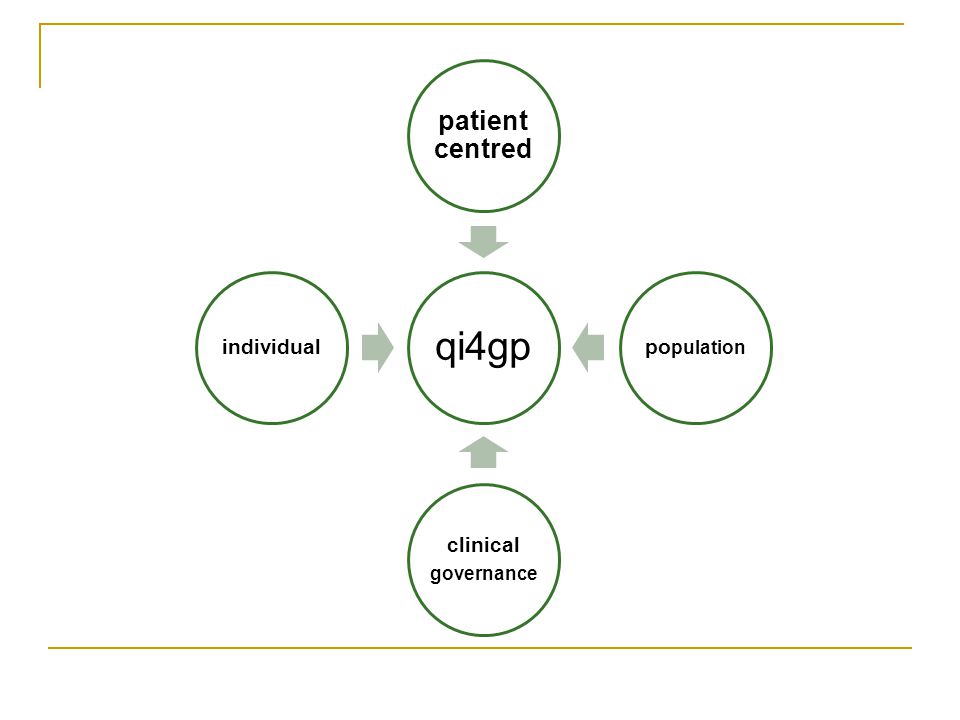
qi4gp & the quest for wisdom Harry Pert

2
The information/knowledge hierarchy

3
Origins of the knowledge hierarchy Where is the Life we have lost in living? Where is the wisdom we have lost in knowledge? Where is the knowledge we have lost in information? TS Eliot Choruses from the Rock. 1934

4
Russell Ackoff’s path to wisdom

5
What then is wisdom? Vision and design: creating a preferred future. Needs to be collaborative, but could include Patient Centred Professionalism. The best health outcomes, as safely as possible, with minimal waste, consistent with community values.

6
How can general practice help? 1. Our health service 2. Our IT platform 3. Clinical governance

7
The health service in New Zealand Every day 55,000 people visit a GP 1,350 people admitted to hospital Every year 3.38m people visit a GP (80% 1 yr, 90% 2 yrs) 15 -19m consultation 30 - 40m clinical decisions made Enrolment, NHI, HPI Increases accountability
 m consultation m clinical decisions made Enrolment, NHI, HPI Increases accountability")
9
Observations, questions & success factors “Why general practitioners use computers and hospital doctors do not” British Medical Journal 2002 Good software, and connectivity (PMS & Healthlink) Culture ‘early adopters’ Business model New support for general practice from the early 90s Clinical leadership Management support
 Culture ‘early adopters’ Business model New support for general practice from the early 90s Clinical leadership Management support")
10
New tier of support for general practice: a vehicle for clinical governance GP Local networks RHA, HFA DHB MoH Management Support Contracting Claims processing IM/IT Analysis and planning Practice support Quality Support Clinical leaders Clinical specialists Peer (cell) group Quality facilitators Pharmacy and lab Immunisation & child health Education organisers
 group Quality facilitators Pharmacy and lab Immunisation & child health Education organisers")
11
Our first IT installation 1989 Server $13k 2 terminals $2.5k Printer $2.8k Total $30.8k

15
Ranolf Medical Centre Date: 21 st November 2008 Prepared by: Michael Humphrey (Technical Director) Scott Whitwell (Sales Director) I.T. Strategy Discussion Paper

16
Observations, questions & success factors Our experience is consistent with international literature and evidence. Dennis Protti BJ Healthcare Computing and Information Management Dec 2003 “Over 150 factors… identified, but only two – top management support and clinician involvement… consistently associated with successful implementation” “Lack of clinician involvement has been a consistent theme in past failures”

17
Observations, questions & success factors Funding Largely self funded No pattern of state funding Expertise Infrastructure in place Many years of experience ‘the burden of prior innovation’

18
The major phases of qi4gp 52 Initial Stakeholder Engagement 8 Clarify & Develop the Vision An Initial Perspective Implement the Vision Apr 07 The Key Directions Project Stage 1 Business Case Agree Projects / Partnerships Broader Stakeholder Engagement 1 Draft Discussion Paper 4 Plan Next Steps 3 Final Discussion Paper Aug 07Dates TBC 7 Plan to Implement 6 Final Strategy Document Consultation Document Detailed Requirements / Solution Stage 2 Business Case High-level Requirements / Solution Current Phase Implementation 9 Track Progress

20
Information collected Demographic Name, Age, Gender, Ethnicities (affiliations) Address (standards, geocode) NHI Funding eligibility Clinical Prevention, screening Conditions
 Address (standards, geocode) NHI Funding eligibility Clinical Prevention, screening Conditions")
21
Long Term Conditions Proactive Structured Acute Conditions Reactive ‘Unstructured’ Relationship remains central Reactive care ok for acute conditions More structure needed for long term conditions Relationship remains central Reactive care ok for acute conditions More structure needed for long term conditions

22
National Regional DHB/NGO Network Practice Individual Population a group of individuals sharing a particular characteristic eg age, gender, ethnicity domicile, deprivation index health need

23
National Regional DHB/NGO Network Practice Individual Activities eg children needing immunisation flu vaccination women needing mammograms cardiovascular risk assessment new migrants & refugees patients & diabetes, copd

24
National Regional DHB/NGO Network Practice Individual opportunity we could measure & manage: any health problem access, utilisation & outcome inequalities improve the care of the individual and inform the sector

25
Increasing role of the patient at the centre of health care (cf the provider and organisations) For information to follow the patient through the health system Referrals, status, discharge, shared records, interconnectivity
 For information to follow the patient through the health system Referrals, status, discharge, shared records, interconnectivity")
26
Self care: trusted information Access to records, appointments, results etc Information about providers: services, facilities, performance.

27
Clinical governance is a system in which NHS organisations are accountable for continuously improving quality of their services and safeguarding high standards of care by creating an environment in which excellence in clinical care will flourish

29
Quality Improvement Local delivery through networks. Quality cycles Measure performance, feedback, peer review, intervention & review

30
Where to from here? 1. We must create “an environment in which excellence in clinical care will flourish” 2. All national GP organisations support this project 3. We want to share this development with you 4. Common ground, needs, unifying purpose

31
The patient safety agenda US: medical error in US hospitals 98,000 deaths per annum (Save 100k) > MVA, breast cancer and aids combined Australia: Inappropriate medicine use,80,000 hospital admissions, cost $350m >550,000 avoidable admissions a year, (9%) NZ: ?? adverse events in Auckland Hospitals 10% of admissions 1% permanent injury or death, 7 extra bed days.

Similar presentations












>")










: Magic or Maze? Norah Bostock Operations Manager: Governance.>")