Download presentation
Presentation is loading. Please wait.

1
Dr. Mirzaei

2
One of the most common surgical emergencies Highest incidence in the second and third decades

3
Location: three taeniae coli converge at the base (fix) Length: 30cm (average 6-9) Tip: retrocecal, pelvic, subcecal, preileal, right pericolic
 Length: 30cm (average 6-9) Tip: retrocecal, pelvic, subcecal, preileal, right pericolic")
4
Secretion of immunoglobulin A Appendectomy and U.C protection ? As a reservoir to recolonize the colon with healthy bacteria

5
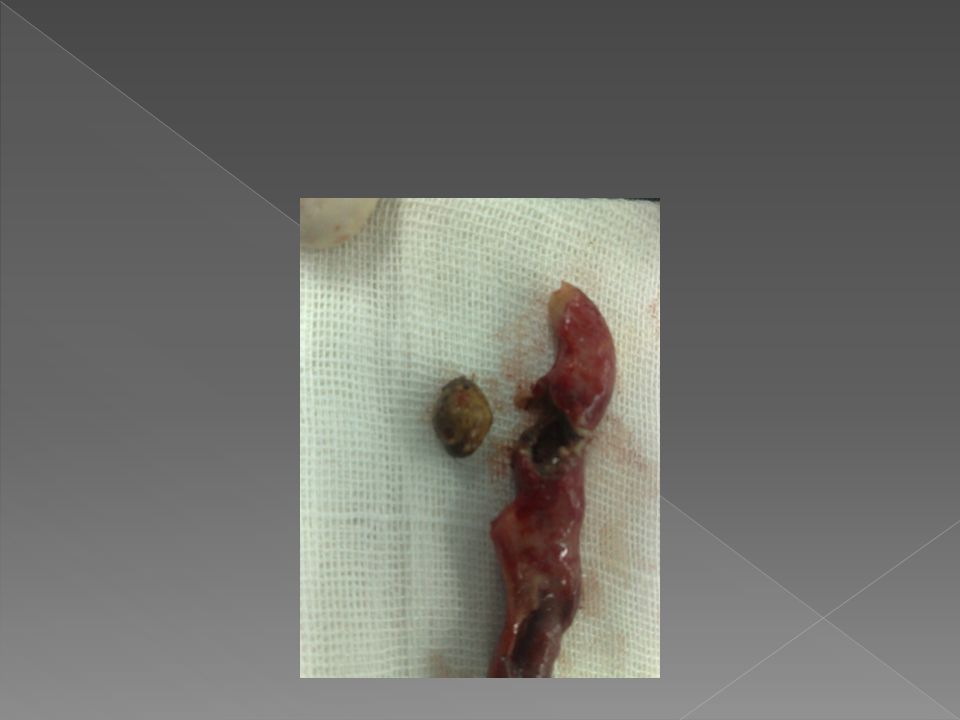
Obstruction - Fecalith - Hypertrophy of lymphoid - Inspissated barium - Tumors - Vegetable and fruit - Intestinal parasites

6
Normal luminal capacity 0.1 ml Proximal obstruction => closed-loop obstrucation Normal secretion of mucosa => distention 0.5 ml secretion => intraluminal pressure 60cm H2O

7
Secretion + rapid multiplication of bacteria => venous pressure increased => occlusion of capillaries Arteriolar inflow continue => vascular congestion

8
Impairment of blood supply => mucosal integrity compromised => bacterial invasion Infarction in antimesentric border => perforation

9
Overall Rate: 25.8% Children < 5 years: 45% Patients > 65: 51%

10
Walling-off process -> Phlegmon: Adherence of bowel loops to the inflamed appendix or a periappendiceal abscess. Mass in exam:2-6% Duration: At least 5-7 days

14
Distention => visceral nerve endings stimulation => vague, dull, diffuse pain in the mid abdomen or lower epigastrium Distention => reflex nausea &vomiting Inflammation of serosa & parietal peritoneum => shift in pain to the right lower quadrant

15
Abdominal pain - Moderately severe - steady, sometimes intermittent cramp - 1-12 h (4-6h) pain => R.L.Q
 pain => R.L.Q")
16
Pain variation - Begins in the R.L.Q - Shift to the L.L.Q (tip in the L.L.Q) - Retrocecal => flank or back pain - Pelvic => suprapubic - Retroileal => testicular pain (irritation of the spermatic artery & ureter)
 - Retrocecal => flank or back pain - Pelvic => suprapubic - Retroileal => testicular pain (irritation of the spermatic artery & ureter)")
17
Intenstinal malrotation -Visceral: normal location - Somatic: where the cecum has been arrested

18
Anorexia (nearly always) - loss of anorexia: diagnosis should be questioned
 - loss of anorexia: diagnosis should be questioned")
19
Vomiting - 75% of patients - neither prominent nor prolonged - only once or twice

20
95% anorexia – pain - vomiting Vomiting – pain: diagnosis should be questioned

21
Temperature : rarely > 1ºC PR: normal or slightly elevated More change: complication ?

22
Lie supine Right thigh drawn up Any motion increases pain Move slowly with caution

23
McBurney point tenderness

24
Local tenderness rebound tenderness Voluntary guarding True reflex (involuntary) rigidity (irritation progress)
 rigidity (irritation progress)")
25
Flank tenderness Local tenderness in rectal exam (pelvic) psoas sign Obturator sign Rovsings sign
 psoas sign Obturator sign Rovsings sign")
26
W.B.C 10,000 – 18,000 Moderate P.M.N predominance W.B.C > 18,000 => possibility of complication CRP U/A: several W.B.C or R.B.C (ureteral or bladder irritation) Bacteriuria generally not seen
 Bacteriuria generally not seen")
27
Plain film (rarely helpful) - abnormal bowel gas pattern - fecalith (highly suggestive) C.X.R (R/O right lower lobe pneumonia)
 - abnormal bowel gas pattern - fecalith (highly suggestive) C.X.R (R/O right lower lobe pneumonia)")
29
Sonography (inexpensive, rapid, no contrast medium, even in pregnancy Noncompressible appendix > 6mm Appendicolith Thickening of appendiceal wall & periappendiceal fluid Remainder of abdominal cavity

30
Exclude Gyn pathology Effective in children & pregnancy

31
Limitations - user dependent - false – positive: dilated fallopian tube, inspissated stool can mimic appendicolith, obesity, - false – negative: appendicitis in tip, retrocecal, markedly enlarged, perforation

32
Dilated appendix>5mm + wall thickening thickened mesoappendix Phlegmon Periappendiceal fat stranding Free fluid Other inflammatory processes

33
Expensive, exposes to radiation, cannot be used during pregnancy, allergy to contrast, intolerance of oral contast

34
Most useful in females (30 – 40% normal appendix) Differentiating acute Gyn pathology
 Differentiating acute Gyn pathology")
35
highest rate: child-bearing women,very young,very old Accuracy of preoperative diagnosis should be: 85% Accuracy>90%: Missed some patients Depends on: anatomic location of the appendix, simple or ruptured, age, sex

37
7-10 high likelihood 4-6 consider further imaging 1-3 low likelihood

38
Differential diagnosis

39
Most in Children Upper respiratory tract infection is present or has recently subsided. Pain is diffuse Tenderness is not sharply localized Guarding sometimes present

40
True rigidity is rare Generalized lymphadenopathy (may) Relative lymphocytosis suggestive Self limited May need immediate exploration
 Relative lymphocytosis suggestive Self limited May need immediate exploration")
41
Pelvic Inflammatory Disease - Usually bilateral - Nausea & Vomiting: 50% - Tenderness Usually lower - Motion of cervix is painful - Diplococci on smear of purulent vaginal discharge - Higher during early phase of cycle

42
Ruptured Graafian Follicle - Spillage of follicular fluid - Pain and tenderness diffuse - Leukocytosis & fever: minimal - Midcycle: Mittelschmerz

43
Twisted Ovarian Cyst - Sudden pain - CT & Sono (transvaginal) - Need emergent operation - Leakage of ovarian cyst: Treated nonoperatively
 - Need emergent operation - Leakage of ovarian cyst: Treated nonoperatively")
45
Ectopic pregnancy Abnormal menses Missing one or two periods or only slight vaginal bleeding Elevated level of human chorionic gonadotropin(B-HCG) Hct level falls Vaginal exam:cervical motion tenderness culdocentesis
 Hct level falls Vaginal exam:cervical motion tenderness culdocentesis")
46
Diarrhea, nausea, vomiting Abdominal Cramps Soft Abdomen between cramps No localizing sign Vomiting - Pain

47
Cecum or sigmoid Diverticulitis Meckel’s Diverticulitis Perforating Carcinoma of the cecum Epiploic appendagitis Pleuritis of the right lower chest Acute Cholecystitis Acute Pancreatitis Hematoma of the abdominal wall Epididymitis, Testicular torsion, U. T. I, Ureteral Stone

Similar presentations