Download presentation
Presentation is loading. Please wait.

1
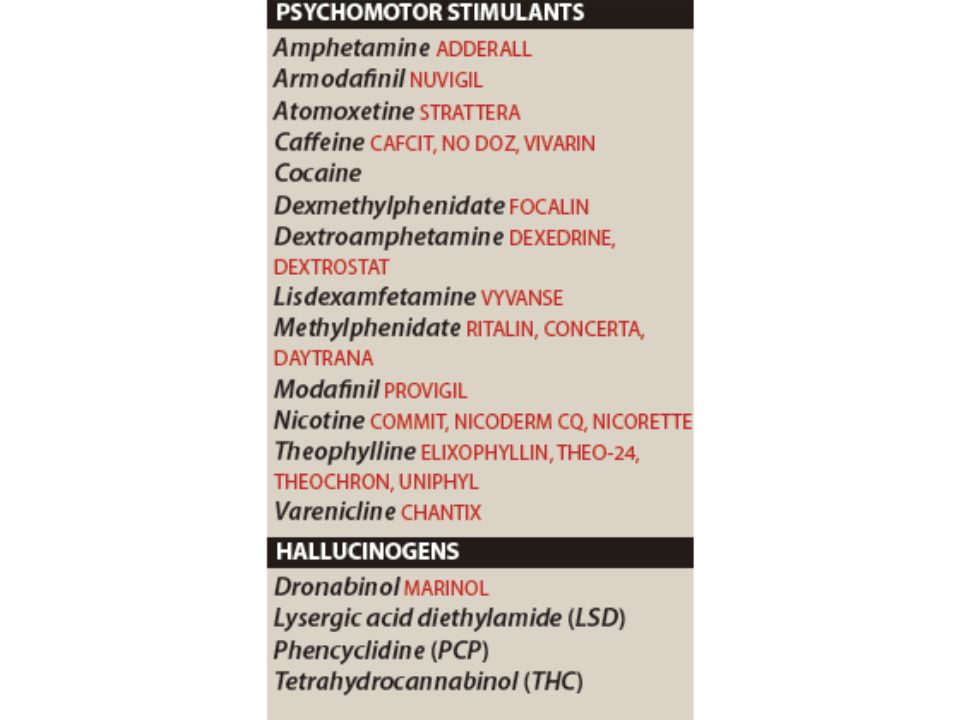
CNS stimulants

2
Schedule for Controlled Drugs Class I –No medical use, high addiction potential Class II –Medical use, high addiction potential Class III –Medical use, moderate potential for dependance Class IV –Medical use low abuse potential Class V

3
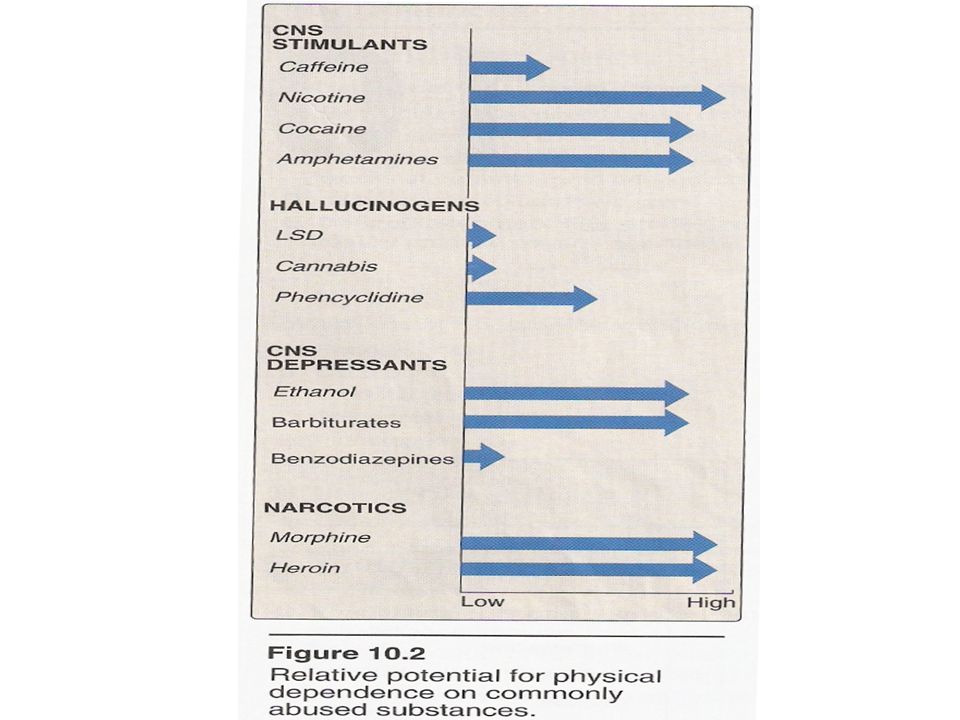
CNS stimulants Little therapeutic application Drug abuse Psychomotor stimulants –Excitement and euphoria, decrease feeling of fatigue and increased motor activity Hallucinogens –Profound change in thought pattern and mood

6
Methylxamine Theophylline –Tea Theobromine –Found in coca Caffeine –Most widely consumed stimulant in the world –Highest con in coffee, –Tea, cola drink, chocolate candy and coca

7
Caffeine Coffee, 8oz drip 104-192 mg Tea, 8oz brewed 20-90 Iced Tea, 8 oz 9-50 Soft Drinks, 8 oz 20-40 Cocoa Beverage, 8oz 3-32 Milk Chocolate, 1 oz 1-15 Dark Chocolate, 1 oz 5-35

8
7oz coffee Drip 115-175 Brewed 80-135 Instant 65-100 Decaf, brewed 3-4 Decaf, instant 2-3

10
Actions Caffeine found in two cups of coffee (100-200 mg) cause –Decrease in fatigue and increase mental alertness 1.5 g of caffeine (12-15 cups) produce tremor and anxiety –Tolerance developed rapidly to the stimulant effect of caffeine Withdrawal effect: –routine consumption of 600 mg (6 cups of coffe) –lethargy, irritability and headache
 cause –Decrease in fatigue and increase mental alertness 1.5 g of caffeine (12-15 cups) produce tremor and anxiety –Tolerance developed rapidly to the stimulant effect of caffeine Withdrawal effect: –routine consumption of 600 mg (6 cups of coffe) –lethargy, irritability and headache")
11
Caffeine Positive inotropic and chronotropic effects –Angina pectoris Mild diuretic action All methylxanthines increase gastric acid secretion –Patient with peptic ulcer Therapeutic uses –Theophyline as bronchodilator

12
Side effects Moderate dose of caffeine –Insomnia, agitation and anxiety A high dose is required for toxicity –Emesis and convulsion Lethal dose 10 gm (100 cup) –Cardiac arrhythmia
 –Cardiac arrhythmia")
14
Nicotine Active ingredient in tobacco There are around 3000 chemicals in cigarettes Nicotine, carbon monoxide and tars

15
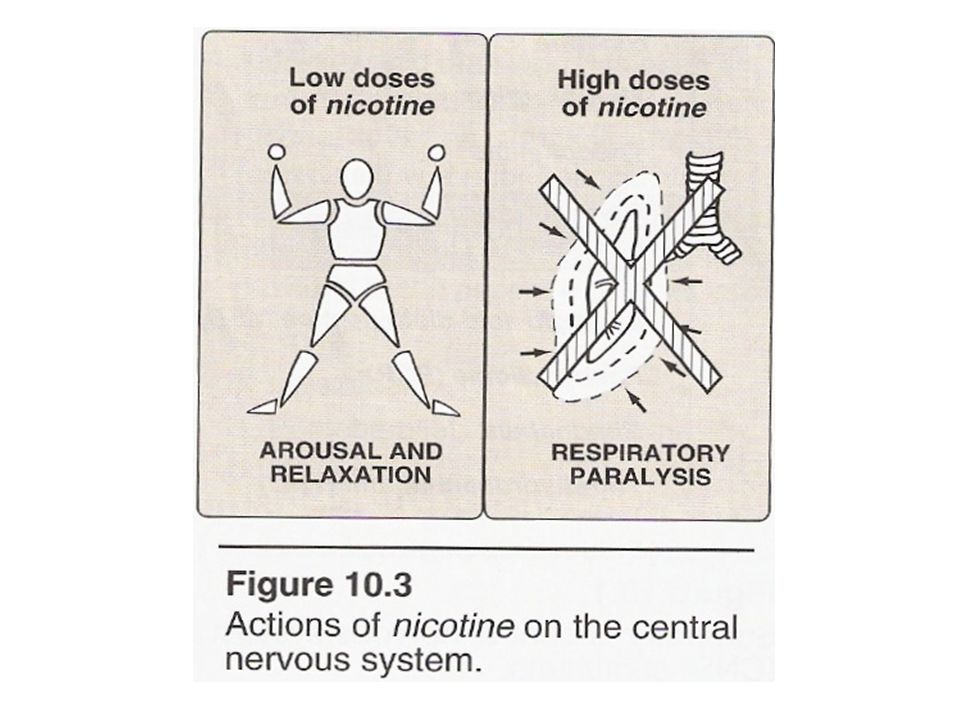
Actions At low dose ganglionic stimulation At high dose ganglionic suppression It is highly lipid soluble 6-8 mg in one cigarette Acute lethal dose 60 mg Placenta and lactating women

17
Actions Some degree of euphoria, arousal and relaxation Improve attention and learning problem High dose central respiratory paralysis and hypotension

18
Peripheral effects Stimulation of sympathetic ganglia and adrenal medulla –Vasoconstriction –Increased heart rate –Increased blood pressure Peripheral vascular diseases At high dose decrease in blood pressure

20
Withdrawal syndrome Physical dependence develops rapidly and is severe Irritability, anxiety, restlessness, difficulty concentrating, headache and insomnia Decrease appetite and abdominal pain

21
Withdrawal syndrome Pharmacological and behaviorial therapy Nicotine patches and nicotine gum Bupropion antidepressant can reduce craving for nicotine

25
Cocaine Inexpensive (USA) Widely available Highly addictive
 Widely available Highly addictive")
28
Cocaine IV, smoking, sniffing Lipophilic Short half life (1 hour)
")
29
COCAINE –Rapid onset of action 10-20 mins –Short duration of action 1-2 hrs –Euphoria followed by depression –Abuser prefer amphetamines due to its longer duration of action (4-6 hrs) Local anesthesia –Eye, nose and throat surgery Vasoconstriction –Nasal septum perforation
 Local anesthesia –Eye, nose and throat surgery Vasoconstriction –Nasal septum perforation")
31
Cocaine MI at any dose at any time with warning and prediction Hyperthermia Cocaine intoxication –Mydriasis –Benzodiazepine

32
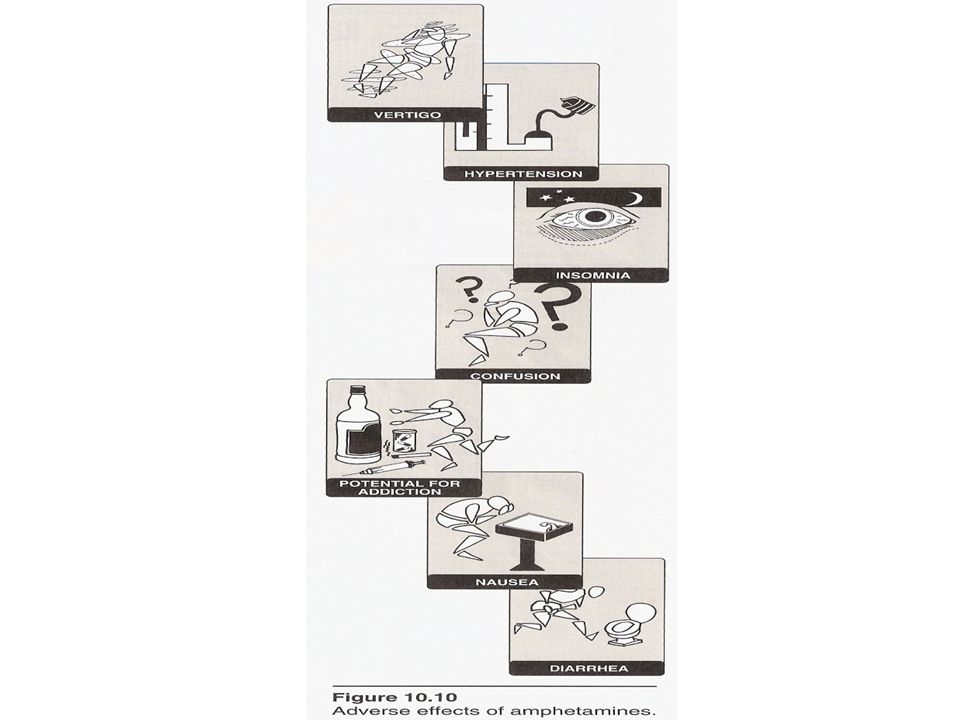
Amphetamines Group of drugs –Amphetamine, dextramphetamines, metaamphetamines Drug abuse Little therapeutic uses (disencourage)
")
35
Attention deficit hyperactivity disorder (ADHD) –Increase rewarding neurotransmitters –Methylpehenidate –Atomoxetine Narcolepsy –Modanifil –Less psychoactive and europhria effect
 –Increase rewarding neurotransmitters –Methylpehenidate –Atomoxetine Narcolepsy –Modanifil –Less psychoactive and europhria effect")
36
Amphetamines Performance enhancement –Alertness –Decrease fatigue –Depressed appetite –Insomnia Followed by depression

38
Methylphenidate 4-6 million children daily in USA –Less addiction potentials than amphetamine –Still controlled substances Dopamine transport inhibitor ADHS GIT disturbance

39
Hallucinogens Lysergic acid diethylamide (LSD) Tetrahydrocannaboidol Penyclidine (PCP) –Anesthesia (angel dust)
 Tetrahydrocannaboidol Penyclidine (PCP) –Anesthesia (angel dust)")
40
Marijuana (cannabis) The main psychoactive component of marjuana –Tetrahydrocannabinol THC Dronabilol the available synthetic compound Cannabinoid receptors Oral or smoking route
 The main psychoactive component of marjuana –Tetrahydrocannabinol THC Dronabilol the available synthetic compound Cannabinoid receptors Oral or smoking route")
43
Marijuana High Euphoria Uncontrolled laughter Time disorientation Depersonalization

44
Marijuana Relaxation Dream like state Thinking or concentration impairment Impotence ? Same side effects as smoking

46
Dronabinol Oral administration Long effect 24 hrs Appetite stimulator for HIV patients Antiemetics

47
LSD Lysergic acid diethylamine –Hallucination with color –Dream like state –Serotonin agonists –Increase BP, increase body heat –Pupillary dilation

48
LSD Psychotic changes Hyperreflexia Muscle weakness Haloperidol

Similar presentations






















![Pharmacology – II [PHL 322] CNS Stimulants Dr. Mohd Nazam Ansari.](/14/4333837/big_thumb.jpg "Pharmacology – II [PHL 322] CNS Stimulants Dr. Mohd Nazam Ansari.>")





.>")


