Download presentation
Presentation is loading. Please wait.

1
Deep Vein Thrombosis and Pulmonary Embolism prophylaxis in Asian general surgical patients: is it necessary? AMY KOK Caritas Medical Centre

2
Introduction Importance Incidence Current practice and guidelines Review of prophylactic methods Applicable to our patients?

3
Introduction General surgical patients Fatal PE ~1% DVT ~24% 10% hospital deaths attributed to PE Venous thromboemobolism (VTE): A Major Source of Mortality and Morbidity
: A Major Source of Mortality and Morbidity")
4
Consequence of unprevented DVT Calf (46%)/thigh (67%)/pelvis(77%) PE 50% untreated DVT PE 50-80% untreated PE associated with DVT Clinicopathological pattern of PTE in Chinese autopsy patient:comparison with caucasian series Pathology 1997
/thigh (67%)/pelvis(77%) PE 50% untreated DVT PE 50-80% untreated PE associated with DVT Clinicopathological pattern of PTE in Chinese autopsy patient:comparison with caucasian series Pathology 1997")
5
Literature review –prophylaxis works! New England Journal of Medicine 1988 and 1999 Prophylaxis can reduce: PE by 50% DVT by 2/3 No increase in bleeding Long term mortality reduction VTE: The most common preventable cause of hospital death

6
Incidence in Caucasian USA 100 per 100,000 UK 48 per 100,000 DVT 23 per 100,000 PE (12% mortality) Australia 30,000 new cases 2,000 death per year 3 rd most common vascular disorder
 Australia 30,000 new cases 2,000 death per year 3 rd most common vascular disorder")
7
Incidence in Asia Study shows that incidence of 1 st time VTE of Asian 3-5x lower HOWEVER…

8
Incidence in Asia is increasing Hong Kong 16.6 per 100,000 population 3 per 10,000 hospital admissions 4.7% 1.8% (PE death) (91-97) Asia 17.1 per 100,000 DVT 3.9 per 100,000 PE Japan and Singapore: 2x increase in DVT (91 97) Epidemiology of VTE in a Chinese population Br J Surg 2004;91:424-8 Pulmonary thromboembolism and venous thrombosis in the Chinese Clin Ortho 1980;150:253-60
 (91-97) Asia 17.1 per 100,000 DVT 3.9 per 100,000 PE Japan and Singapore: 2x increase in DVT (91 97) Epidemiology of VTE in a Chinese population Br J Surg 2004;91:424-8 Pulmonary thromboembolism and venous thrombosis in the Chinese Clin Ortho 1980;150:253-60")
9
Guidelines for VTE Prophylaxis

10
Modalities of prophylaxis Mechanical Graduated compression stockings Intermittent pneumatic compression Venous foot pump Pharmacological Unfractionated heparin Low-molecular weight heparin Pentasaccharide Aspirin

11
Mechanical prophylaxis Graduated compression stockings (GCS) Intermittent pneumatic compression (IPC) devices Venous foot pump (VFP) Aim: Increase venous outflow Reduce stasis within leg veins
 Intermittent pneumatic compression (IPC) devices Venous foot pump (VFP) Aim: Increase venous outflow Reduce stasis within leg veins")
12
Mechanical prophylaxis Recommendation: High risk for bleeding (Grade 1A) Adjunct to anticoagulant prophylaxis (Grade 2A) Proper use of and optimal adherence (Grade 1A) Data from Geerts WH, Bergqvist, Pineo G, et al. Prevention of venous thromboembolism. Chest 2008; 133:381S-435S

13
Aspirin NO significant benefit Inferior results NOT recommended alone for VTE in any patient group (Group 1A)
")
14
Unfractionated heparin Effective: General and orthopedics surgery Reduce VTE by 50-70% Minor bleeding events: 6.3% vs 4.1% (statistically significant)
")
15
Low molecular weight heparin Examples: Enoxaparin Fraxiparin Effective: General and Orthopedic surgery

16
General surgery General recommendation: Avoid dehydration Early mobilization Leg elevation Stop Oral contraceptive pills or Hormone replacement therapy 4 weeks beforehand Consider regional anaesthesia

17
General surgery Low Risk (Grade 1A) Minor Surgery < 40 No additional risk factors (cancer, history of VTE) Recommendation No specific prophylaxis; early mobilization 8th ACCP GUIDELINE
 Minor Surgery < 40 No additional risk factors (cancer, history of VTE) Recommendation No specific prophylaxis; early mobilization 8th ACCP GUIDELINE")
18
General surgery Moderate Risk (Grade 1A) Minor Surgery: with additional risk factors Nonmajor surgery: 40-60 years with no risk factors Major surgery: < 40 with no risk factors Recommendation Heparin (5,000 units Q12H, start 1-2 hrs preop till discharge) Enoxaparin (40mg sc 1-12 hrs preop followed by 40mg sc Q24H 12hrs postop till discharge) 8th ACCP GUIDELINE
 Minor Surgery: with additional risk factors Nonmajor surgery: years with no risk factors Major surgery: < 40 with no risk factors Recommendation Heparin (5,000 units Q12H, start 1-2 hrs preop till discharge) Enoxaparin (40mg sc 1-12 hrs preop followed by 40mg sc Q24H 12hrs postop till discharge) 8th ACCP GUIDELINE")
19
General surgery High Risk (Grade 1A) Non-major surgery: > 60 yr or have additional risk factors Major Surgery: > 40 or have additional risk factors Recommendation Heparin (5,000 units Q8H, start 1-2 hrs preop till discharge) Enoxaparin (40mg sc 1-12 hrs preop followed by 40mg sc Q24H 12hrs postop till discharge ) 8th ACCP GUIDELINE
 Non-major surgery: > 60 yr or have additional risk factors Major Surgery: > 40 or have additional risk factors Recommendation Heparin (5,000 units Q8H, start 1-2 hrs preop till discharge) Enoxaparin (40mg sc 1-12 hrs preop followed by 40mg sc Q24H 12hrs postop till discharge ) 8th ACCP GUIDELINE")
20
General surgery Highest Risk (Grade 1C) Major surgery: >40 + prior VTE, cancer or hypercoagulable state Recommendation Heparin or LMWH + Intermittent pneumatic compression sleeves till discharge 8th ACCP GUIDELINE
 Major surgery: >40 + prior VTE, cancer or hypercoagulable state Recommendation Heparin or LMWH + Intermittent pneumatic compression sleeves till discharge 8th ACCP GUIDELINE")
21
Special consideration Extended VTE prophylaxis (selected high risks patients) Recommendation Extend prophylaxis for 28-30days (Grade 2A) Enoxaparin 40mg sc Q24H High bleeding risk Recommendation Optimal use of mechanical thromboprophylaxis (Grade 1A) Subsituted or added on pharmacological thromboprophylaxis when bleeding risks decreased (Grade IC) Prolonged prophylaxis in abdominal and pelvic cancer reduced DVT 12 to 5% Bergqvist NEJM 2002
 Recommendation Extend prophylaxis for 28-30days (Grade 2A) Enoxaparin 40mg sc Q24H High bleeding risk Recommendation Optimal use of mechanical thromboprophylaxis (Grade 1A) Subsituted or added on pharmacological thromboprophylaxis when bleeding risks decreased (Grade IC) Prolonged prophylaxis in abdominal and pelvic cancer reduced DVT 12 to 5% Bergqvist NEJM 2002")
22
General Surgery Laparoscopic surgery Longer general anasthesia Pneumoperitoneum and reverse Trendelenburg position reduces venous return

23
Laparoscopic surgery Rates of VTE is LOW

24
General Surgery Laparoscopic surgery Recommendation No risk factors – aggressive early mobilization (Grade1A) Risk factors – Heparin, LMWH, IPC or GCS (Grade 1C) 8th ACCP GUIDELINE
 Risk factors – Heparin, LMWH, IPC or GCS (Grade 1C) 8th ACCP GUIDELINE")
25
Bariatric Surgery Reported incidence: varied! Unknown: optimal regimen, dosage, timing and duration Recommendation Routine thromboprophylaxis with Heparin, LMWH or fondaparinux + IPC National Bariatric Surgery Registry

26
Guidelines for VTE Prophylaxis in Asia HK: Guideline for orthopedics and ICU patients Japan: Japanese guidelines for prevention of VTE 2004 Decrease in perioperative VTE Korea: Korean guidelines for the prevention of VTE Malaysia: Prophylaxis of VTE, clinical guideline

27
JAPAN

28
Korean guidelines for prevention of VTE 2010

29
Hong Kong NO unique guideline for general surgery Guidelines for ICU, neurosurgery and orthopedics patients

30
Hong Kong TMH/PMH ICU

31
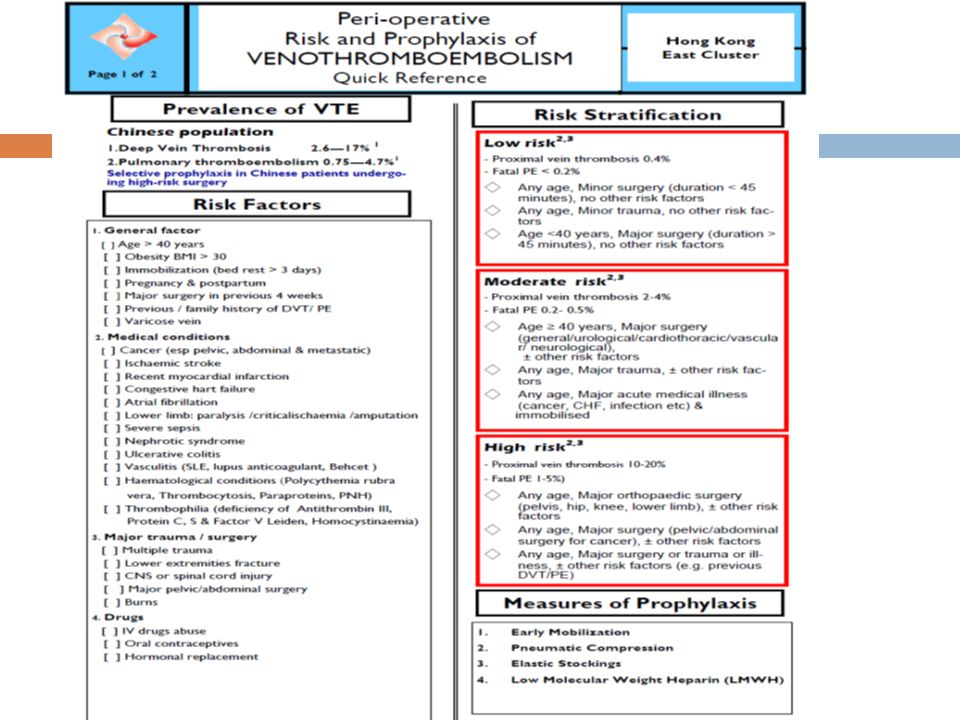
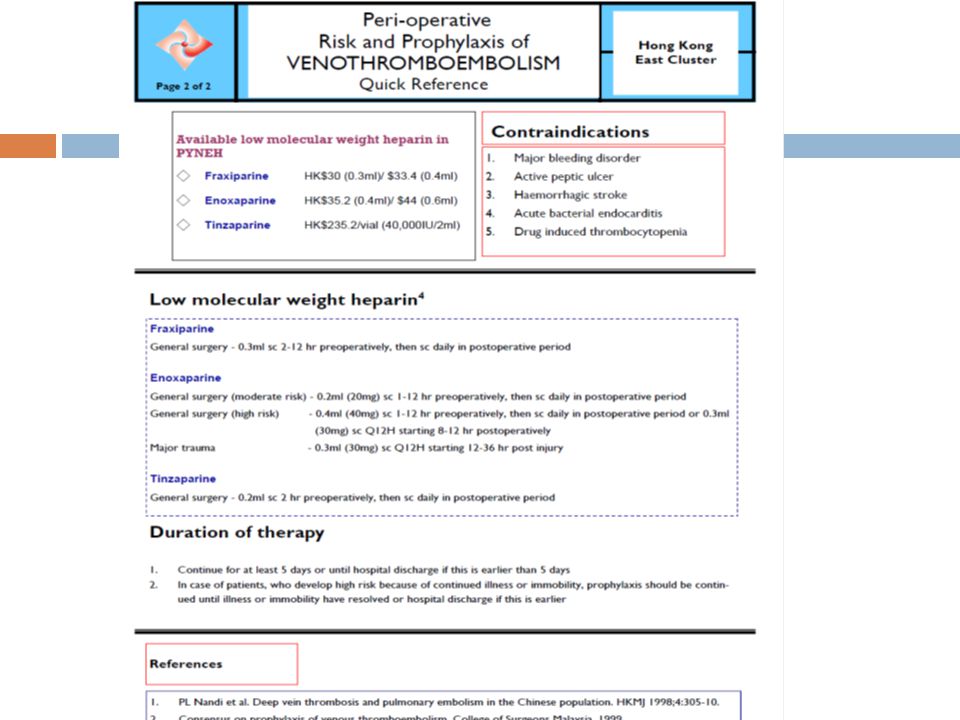
Guideline in Hong Kong Step 1: Identify high risk surgical procedures or injury Step 2: other VTE risk factors Step 3: Risk stratification Step 4: Assess bleeding risk or contraindication Step 5: Select appropriate thromboprophylaxis Step 6: Reassess

32
Bring home message Do not ignore venous thromboembolism (VTE) Incidence is rising in Asian population Prophylaxis and Guidelines with reference to other Asian countries should be considered Further RCT required
 Incidence is rising in Asian population Prophylaxis and Guidelines with reference to other Asian countries should be considered Further RCT required")
33
Thank you

37
Risk factors for DVT Stasis Surgery, trauma, immobility, paresis Increasing age Pregnancy and postpartum Heart or respiratory failure Obesity Vessel Injury Previous DVT Smoking Varicose veins Central venous catheterization Hypercoagulability Increasing age Malignancy Cancer therapy Estrogen therapy (OCP or HRT) Acute medical illness Inflammatory bowel disease Nephrotic syndrome Myeloproliferative disorders Paroxysmal nocturnal hemoglobinuria Inherited or acquired thrombophilia
 Acute medical illness Inflammatory bowel disease Nephrotic syndrome Myeloproliferative disorders Paroxysmal nocturnal hemoglobinuria Inherited or acquired thrombophilia")
38
Chinese population NOT UNCOMMON! Annual incidence of VTE in HK Chinese 16.6 events per 100,000 population 3 per 10,000 hospital admissions Autopsy study in adult HK Chinese population PE: 0.75% Postoperative incidence (120940 surgical operations) DVT: 0.13% PE: 0.04% Epidemiology of VTE in a Chinese population Br J Surg 2004;91:424-8 Pulmonary thromboembolism and venous thrombosis in the Chinese Clin Ortho 1980;150:253-60
 DVT: 0.13% PE: 0.04% Epidemiology of VTE in a Chinese population Br J Surg 2004;91:424-8 Pulmonary thromboembolism and venous thrombosis in the Chinese Clin Ortho 1980;150:")
39
Chinese population Incidence of DVT after colorectal surgery in a chinese population Open surgery 38.9% Laparoscopic surgery 50% Study showed 41.7% developed asymptomatic postop DVT in postop colorectal cancer patients in HK Noted increase prevalence in HK DVT 2.6-17% PE 0.75-4.5% INCIDENCE OF DEEP VEIN THROMBOSIS AFTER COLORECTAL SURGERY IN A CHINESE POPULATION ANZ J. Surg.(2001)71, 637–640
71, 637–640.")
40
Chinese population Prevalence of DVT in different surgery Orthopedic surgery 53.3% Neurosurgery 10% General surgery 8.5% Colorectal surgery 4%

41
Surgical patients: Anaesthetic time >90mins Anaesthetic time >60mins + operation involves pelvis or lower limb Acute surgical admission with inflammatory or intraabdominal condition Expected reduced mobility Any VTE risks factors

43
Mechanism of Heparin Unfractionated heparin inactivates both Factor IIa and Xa LMWH has increased affinity for Factor Xa Fondiparinux is only a pentasaccharide sequence

45
Bleeding risk Acute bleeding Acquired bleeding disorders eg acute liver failure Concurrent use of anticoagulant eg warfarin Acute stroke Thrombocytopenia (Plt <75) Untreated inherited bleeding disorders (eg hemophilia)
 Untreated inherited bleeding disorders (eg hemophilia)")
46
Major bleeding Death Decrease in Hb >/=2 Transfusion of at least 2 units Bleeding from retroperitoneal, intracranial or intraocular site

47
Contraindication for mechanical prophylaxis Suspected or proven peripheral arterial disease Peripheral arterial bypass grafting Peripheral neuropathy or other causes of sensory impairment Allergy Severe leg edema Major limb deformity Local skin condition eg dermatitis, gangrene etc

48
New oral anticoagulants Factor Xa inhibitors: apixaban and rivaroxaban Factor IIa inhibitors: dabigatran No need for routine coagulation monitoring No major food interactions Limited drug-drug interactions Trial on orthopedic surgery

Similar presentations





















 Prophylaxis Policy Mary-Anne Davies Patient Safety Specialist Accreditation Coordinator.>")

>")


 IPC/GCS or, UFH 5000 SQ q 12 hrs or, Enoxaparin 40mg SQ daily IPC/GCS or, UFH 5000.>")

