Download presentation
Presentation is loading. Please wait.

1
Best Practices in Meeting NPSG 3E-Anticoagulation Requirements MaryAnne Cronin, PharmD Assistant Director of Pharmacy Glen Cove Hospital

2
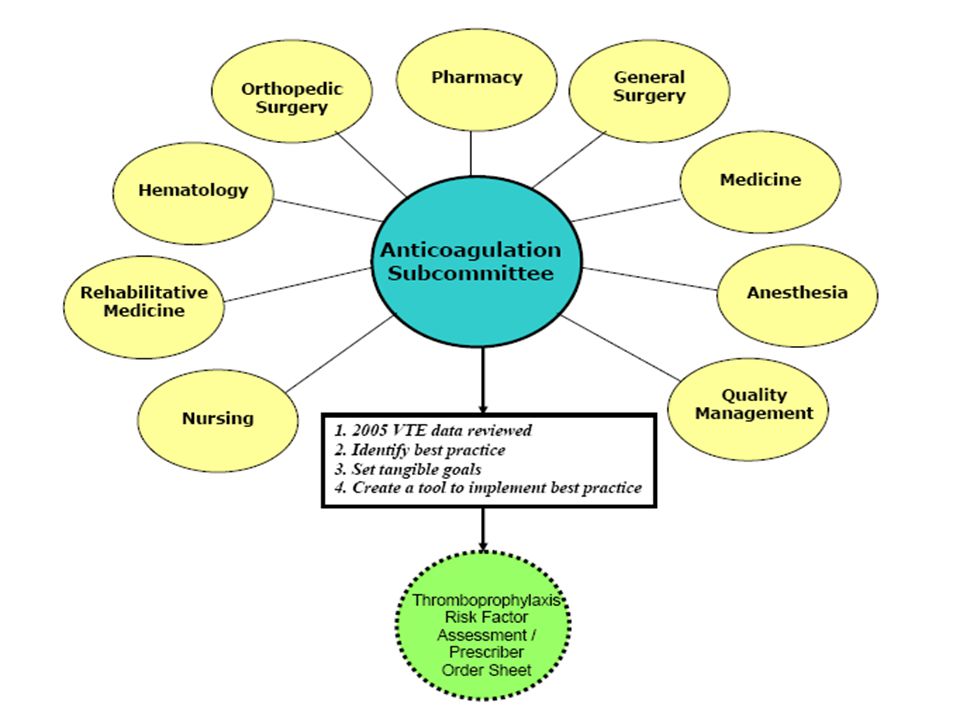
Clinical Pharmacy Presence Addition of Clinical Pharmacist to the orthopedic and rehabilitative medicine services in 2004 identified areas of potential improvement Review of all VTE in 2005 led to the formation of a multidisciplinary Anticoagulation Subcommittee

5
Orthopedic Service Order sheet approved by Anticoagulation Subcommittee in April 2005 Revised protocol applied immediately to orthopedic surgical population via patient care rounds and chart reviews –Minimize warfarin monotherapy –Begin LMWH POD#1 with non-epidural analgesia and 6 hours after catheter removal with epidural analgesia –Bridge warfarin with LMWH until INR > 2.0 x 2 consecutive days AND warfarin administered for at least 4 days.

6
What impact do you think the implementation of a Prescriber Order Sheet had on our rate of venous thromboembolism in the ORTHOPEDIC SURGERY PATIENT over one year? A.12% B.25% C.35% D.48%

7
Rate VTE Total Joint Replacement Program 2005: n = 44/953 48% reduction 2005 to 2006. 2006: n = 24/1003. 48% reduction 2005 to 2006. 43% reduction 2005 to 2007. 2007: n = 28/1054. 43% reduction 2005 to 2007.

8
Pulmonary Embolism Total Joint Replacement Program 2005: 9/953 2006: 4/1003 2007: 2/1054 2005: 9/953 2006: 4/1003 2007: 2/1054 57% reduction 2005 to 2006. 80% reduction 2005 to 2007.

9
WARFARIN MECHANISM OF ACTION Warfarin acts by inhibiting levels of anticoagulant factors II, VII, IX, and X and procoagulant proteins C and S. Protein C promotes fibrinolysis. Factor VII and protein C have short half-lives (6 hrs). Although depletion of Factor VII rise in INR, patient not protected from thrombosis until Factor X and Factor II levels fall substantially. The half-life of Factor X is ~40 hrs, and ~60-70 hrs for Factor II.
. Although depletion of Factor VII rise in INR, patient not protected from thrombosis until Factor X and Factor II levels fall substantially. The half-life of Factor X is ~40 hrs, and ~60-70 hrs for Factor II..")
10
WARFARIN MECHANISM OF ACTION Rapid reduction of Protein C leaves the patient hypercoagulable and places them at risk for thrombosis with warfarin monotherapy. If the patient is not bridged with LMWH or unfractionated heparin (UFH), warfarin alone induces a protein C deficiency prothrombotic state.
, warfarin alone induces a protein C deficiency prothrombotic state..")
12
Very High Risk TJR Patients History of VTE Clinically or genetically hypercoagulable Morbidly obese Monitored closely - Aggressive anticoagulation (LMWH on POD#1) - AntiFactor Xa levels for clinical efficacy in special populations - AntiFactor Xa levels for clinical efficacy in special populations
 - AntiFactor Xa levels for clinical efficacy in special populations - AntiFactor Xa levels for clinical efficacy in special populations")
13
Medical Service Form approved by all necessary committees and Medical Board in Sept 2006 Education provided to attendings, residents, NPs, PAs, RNs indicating that Thromboprophylaxis Order Sheet must be completed within 24 hours of patient admission Initiative up and running by end of 2006 Clinical interventions, phone calls, chart reviews completed by clinical pharmacy service Daily reports sent to pharmacy indicating patients requiring re-order to maintain prophylaxis throughout hospitalization

14
What impact do you think the implementation of a Prescriber Order Sheet had on our rate of venous thromboembolism in the MEDICAL PATIENT over one year? A.15% B.25% C.40% D.60%

15
Rate VTE Medical Service No Contraindication 2005: 28/5113 = 0.55% 2006: 30/5161 = 0.58% 2007: 11/4716 = 0.23% 60% reduction 2006 to 2007

16
Rehabilitative Medicine Mandatory use of Thromboprophylaxis Order Sheet improved rates of preventable VTE overall Patients admitted on warfarin monotherapy with subtherapeutic INRs bridged with LMWH until INR> 2.0 unless surgeon opposed therapy

17
Number Hospital-Acquired VTE Rehab 2005: 26/1791 = 1.5% 2006: 11/2284 = 0.48% 68% reduction 2005 to 2006 2007: 9/2179 = 0.41% 73% reduction 2005 to 2007

18
Rate Hospital-Acquired VTE Medical Service Heparin 5000 units SC q12hr Failure Lack of efficacy of Heparin 5000 units SC q12h for venous thromboprophylaxis supported by this 3-year data.

19
In addition to NPSG requirements, what other forces are impacting the prophylaxis and treatment of VTE?

20
PROPHYLAXIS OF VTE: American College of Chest Physicians (ACCP) 2008 Guidelines
 2008 Guidelines")
21
TREATMENT OF VTE: 2008 ACCP Guidelines

25
Patients Transferred Acute Patients Requiring Acute Care for Treatment of VTE YearRehab (# pts) Med-Surg (# pts) Total Acute Days Percent reduction 20059580 2006746617.5% 2007423350%
 Med-Surg (# pts) Total Acute Days Percent reduction % %")
26
Conclusion: Meeting NPSG 3E Requirements The Anticoagulation Subcommittee meets quarterly and is responsible for all issues concerning safe and efficacious administration of anticoagulation Hospital protocols and order sheets utilized for anticoagulation prophylaxis and treatment

27
Clinical Pharmacists round on each unit and monitor for anticoagulation safety and efficacy –INRs and PLTs –Morbid obesity (BMI>40) and low body weight ( 40) and low body weight (<45kg female, <57kg male) –Renal function –PMH (aggressive vs conservative) Patients and/or family members educated by nursing and/or pharmacy prior to discharge on warfarin and enoxaparin –Discharge kit for enoxaparin –Educational materials on safe administration of warfarin –“Coumadin Cookbook” Conclusion: Meeting NPSG 3E Requirements, cont.
 and low body weight ( 40) and low body weight (<45kg female, <57kg male) –Renal function –PMH (aggressive vs conservative) Patients and/or family members educated by nursing and/or pharmacy prior to discharge on warfarin and enoxaparin –Discharge kit for enoxaparin –Educational materials on safe administration of warfarin – Coumadin Cookbook Conclusion: Meeting NPSG 3E Requirements, cont.")
Similar presentations
















 Prophylaxis Policy Mary-Anne Davies Patient Safety Specialist Accreditation Coordinator.>")
 Anticoagulation Inpatient Management (AIM) Team 2009.>")


 is 19%-25% (Buckner, et al., 2013). Post surgical orthopedic patients.>")

 recommended cardiac surgery patients, with.>")

