Download presentation
Presentation is loading. Please wait.

1
Sniffing out the problem Jonathan Hern

2
Commissioning Guide for Chronic Rhinosinusitis ENTUK and RCS Based on European position paper on sinusitis Guidance for primary and secondary care treatment of sinusitis

3
Introduction Acute sinusitis Duration < 12 weeks Aetiology usually infective Chronic sinusitis Duration > 12 weeks Aetiology multifactorial including inflammatory, infective and obstructive (sinus ventilation and drainage) 10% prevalence in UK
 10% prevalence in UK")
4
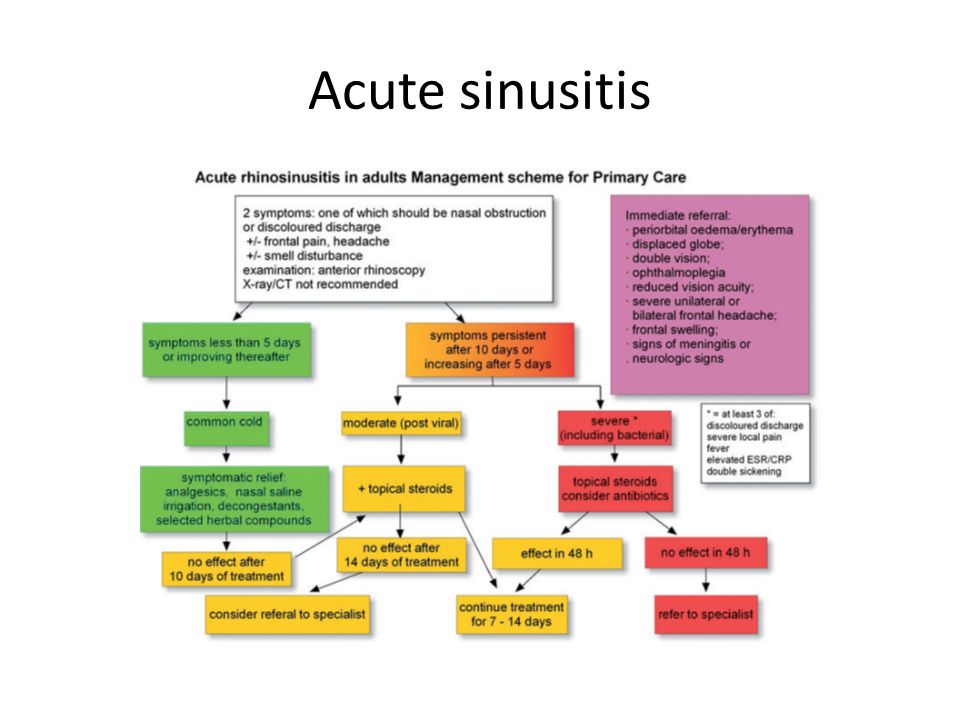
Acute sinusitis History Presence of 2 or more symptoms for < 12 weeks Either nasal obstruction and/or discharge Facial pain/pressure Reduced sense of smell

5
Acute sinusitis

7
Paediatric acute sinusitis

8
Chronic Sinusitis in primary care History Presence of 2 or more symptoms for > 12 weeks Either nasal obstruction and/or discharge Facial pain/pressure Reduced sense of smell Subcategorised by presence or absence of nasal polyps CRSwNP or CRSsNP Unilateral symptoms raise suspicion of neoplasia

9
Primary care Examination Anterior rhinoscopy Otoscope or endoscope Discharge Inflammation Nasal polyps Turbinate hypertrophy

10
Assessment of severity 10cm Visual analogue scale Mild (VAS 0 -3) Moderate/severe (VAS>3)
 Moderate/severe (VAS>3)")
11
Allergic rhinitis Nasal itching Sneezing Rhinorrhoea Epiphora Asthma (assess control)
")
12
Red flags Unilateral symptoms Cacosmia Epistaxis/crusting Diplopia Reduced visual acuity Globe displacement Periorbital oedema Severe frontal headache Neurological signs

13
Primary care Treatment Nasal douching Intranasal corticosteroids (mometasone or fluticasone) Bilateral nasal polyps visible on AR Prednisolone EC 30mg OD 7 days with topical steroid drops (fluticasone or betamethasone)
 Bilateral nasal polyps visible on AR Prednisolone EC 30mg OD 7 days with topical steroid drops (fluticasone or betamethasone)")
14
Options not advised in primary care in Chronic Sinusitis Plain x-rays Oral antibiotics

15
Reassess symptom control after 3 months Mild symptoms (VAS 0 -3) continue with medical treatment Moderate/severe (VAS >3) assess treatment compliance and technique and refer to secondary care if not improving
 continue with medical treatment Moderate/severe (VAS >3) assess treatment compliance and technique and refer to secondary care if not improving")
16
Treatment of chronic sinusitis in primary care

17
Secondary care History Reassess history and consider diagnosis and treatment of co-morbidity Allergy ASA triad Systemic condition (vasculitides, Churg- Strauss, sarcoidosis) Ciliary dyskinesia
 Ciliary dyskinesia")
18
Secondary care Examination Nasal endoscopy Purulent middle meatal discharge (swab) Polyps Middle meatal oedema
 Polyps Middle meatal oedema")
19
SNOT 22 Disease specific patient related outcome measure

20
Secondary care CT scanning Uncertainty from nasal endoscopy (2 out of 3 rule) Neoplasia suspected Complications of CRS (orbital/neurological) Allergy testing SPT or RAST and IgE
 Neoplasia suspected Complications of CRS (orbital/neurological) Allergy testing SPT or RAST and IgE")
21
Secondary care Continue nasal saline irrigation CRSwNP Prednisolone, steroid drops/spray, consider Doxycycline 100mg OD 3 weeks CRSsNP Steroid spray, consider 4-6 weeks of macrolide antibiotic (most likely effective if IgE levels not elevated; avoid clarithromycin with statins in patients with IHD)
")
22
Treatment of CRSsNP

23
Treatment of CRSwNP

24
Surgery Endoscopic sinus surgery Balloon sinuplasty Ethmoid or frontal stratus CT mandatory before surgery. CT score <4 alternative diagnosis should be considered Many patients likely to require long term maintenance therapy with saline irrigation and topical steroids

25
Variation in treatment

26
Conclusion Primary and Secondary Care Pathways Consider earlier referral Early surgery Long term medical maintenance therapy

Similar presentations