Download presentation
Presentation is loading. Please wait.

1
Mr Robert Harris ENT Consultant
Referrals to ENT Mr Robert Harris ENT Consultant

2
Commonest referrals Adult Hearing Loss / tinnitus Sinusitis
Paediatric Glue Ear Ear Wax Paediatric snoring/OSA Globus / cough Adult snoring/OSA Throat pain Otitis externa Tonsillitis Otalgia (cause unknown) Dizziness Recurrent epistaxis Hoarseness Rhinitis
 Dizziness. Recurrent epistaxis. Hoarseness. Rhinitis.")
3
Triage options Secondary Care Secondary Care outside Croydon
Intermediate Care Back to Referrer Different Specialty Adult Audiology Paediatric Audiology

8
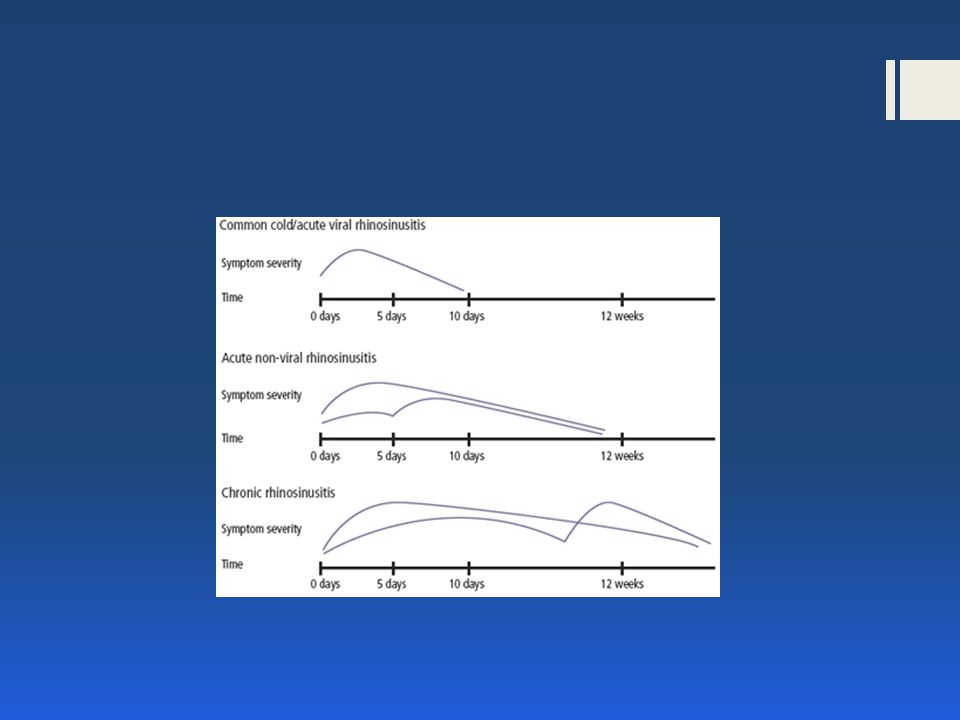
Symptoms in acute and chronic rhinosinusitis
ARS Nasal obstruction Anterior or postnasal discharge Progressive severe facial pain (affects teeth if maxillary) Reduced smell not volunteered Often pyrexia CRS Nasal obstruction Anterior or postnasal discharge (often discoloured yellow with eosinophils but green and infected uncommon) Facial pain uncommon unless acute exacerbation Hyposmia common Late onset asthma common
 Reduced smell not volunteered. Often pyrexia. CRS. Nasal obstruction. Anterior or postnasal discharge. (often discoloured yellow with eosinophils but green and infected uncommon) Facial pain uncommon unless acute exacerbation. Hyposmia common. Late onset asthma common.")
10
Case study – 1 week history of itchy ear
10

11
Case study – 1 week history of itchy, painful ear, decreased hearing
11

12
12

13
13

14
14

15
15

16
ENT UK evidence review and consensus document
The following be adopted as formal ENT-UK guidance: When treating a patient with a discharging ear, in whom there is a perforation or patent grommet: 1. If a topical aminoglycoside is used, this should only be in the presence of obvious infection 2. Topical aminoglycosides should be used for no longer than two weeks 3. The justification for using topical aminoglycosides should be explained to the patient 16

17
17

18
18

19
19

20
Case study 65 year old diabetic 3 week history of otalgia 20

22
Otitis Externa Prevention
Keep ears dry Dry thoroughly after wet EarCalm Early intervention with topical steroids / antiobiotics

23
Case study 45 year old IT manager
woke yesterday with muffled right hearing 23

24
Sudden hearing loss Tuning fork tests
Consider high dose steroids and urgent referral for intratympanic steroids 24

27
Paediatric OSA

28
Paediatric OSA Nasal symptoms Snoring Assessment of severity
History Video Clinical examination Anterior rhinoscopy Oropharynx Neck

30
Silent Laryngopharyngeal Reflux
Excessive throat clearing Persistent cough Hoarseness A "lump" in the throat that doesn't go away with repeated swallowing A sensation of post nasal drip Dry throat Sore throat Hallitosis Furry tongue

31
Silent Laryngopharyngeal Reflux
Sleep on an empty stomach Elevate head of bed Smoking cessation PPI double dose with evening meal for 1 month Manage associated anxiety

33
Thank you

34
Mr Robert Harris MSc FRCS
NHS CUH T: F: SGH T: F: AIRCALL: (SG933) Private Shirley Oaks Hospital North Downs Hospital Parkside Hospital T: F:
 Private. Shirley Oaks Hospital. North Downs Hospital. Parkside Hospital. T: F:")
35
Rationale for long-term macrolides for Chronic Rhinosinusitis

36
Acute RS vs Chronic RS bacteria
ARS Stretococcus pneumoniae Haemophilus influenza Moraxella catarrhalis Few anaerobes, streptococci, staphylococcus CRS Staph Aureus Coag neg staph Strep pneum anaerobes

37
Long-term antibiotics
Efficacy of long term treatment in diffuse panbronchiolitis Asian studies CRS over last decade Long-term low-dose macrolide 60-80% improvement in CRS refractory to surgery and steroids Slow onset, ongoing improvement at 4/12

38
Macrolides Increase mucociliary transport Reduce goblet cell secretion
Accelerated apoptosis of neutrophils Other anti-inflammatory effects Inhibit IL expression Reduce virulence and tissue damage caused by chronic bacterial colonisation Increase ciliary beat

39
Long-term macrolides Prospective RCT N=90 CRS =/- NP 3/12 erythromycin
ESS VAS, SNOT-22, SF36, NO, rhinometry, saccharine clearance, endoscopy No signif difference in outcome

42
Medical Regimen for Chronic Rhinosinusitis
Clarithromycin 250mg bd for 6-12 weeks Xylometazoline bd for 1 week Nasal douche for 6-12 weeks Topical nasal steroids for 6-12 weeks 42

43
Medical Regimen for nasal polyps
Maintenance dose of topical nasal steroid long-term 30mg prednisolone for 7 days as required, (but not more frequently than 3 monthly) 43
 43.")
Similar presentations