Download presentation
Presentation is loading. Please wait.

1
3 rd Lecture Biome II Dr. Manal Radwan Salim Lecturer of Physical Therapy Saturday 12-10-2013 for the two groups

2
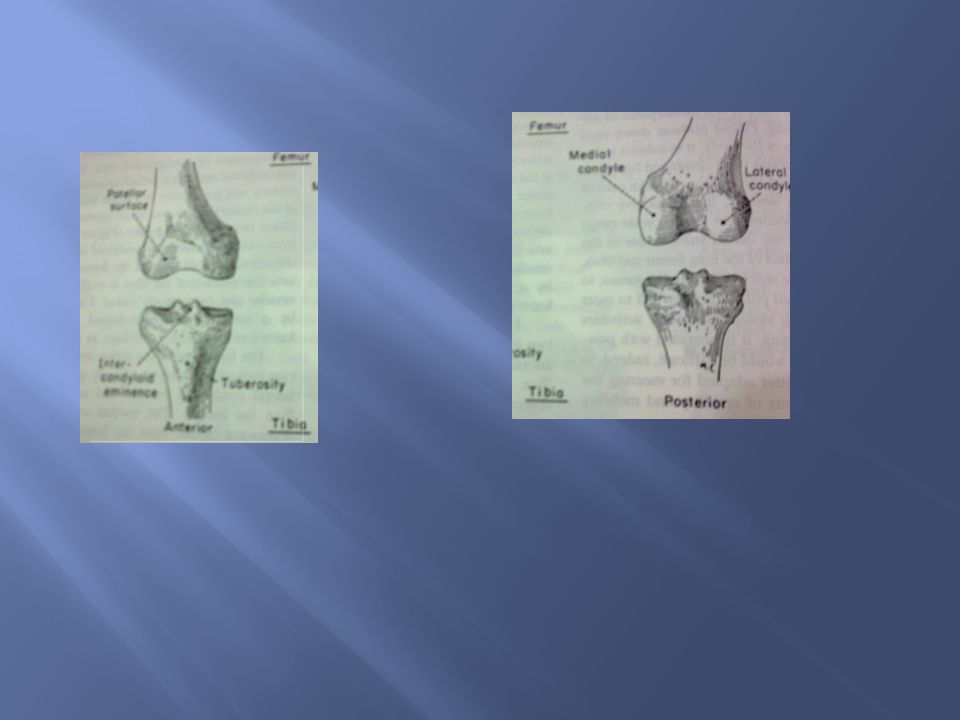
Arthrology and Movements a)Lateral and medial tibiofemoral: Consist of articulation between large convex femoral condyles, and nearly flat and smaller tibial condyles. b) Patellofemoral: Knee stability depends mainly on soft tissue constraints rather than bony configuration.
 Patellofemoral: Knee stability depends mainly on soft tissue constraints rather than bony configuration..")
4
Knee allows two degrees of freedom flx/ext, and int/ext rotations

5
Locking knee on full extension requires knee rotation about 10 degrees. Screw home rotation is different from axial rotation that occur at knee it is a conjunct rotation, linked mechanically to flexion and extension kinematics and cant be performed independently. In tibiofemoral extension: the tibia externally rotates about 10 degrees. In femorotibial extension(rising from squat): The femur internally rotates on fixed tibia. Regardless whether leg or femur is moving the knee is externally rotated 10 degrees when fully extended.
: The femur internally rotates on fixed tibia. Regardless whether leg or femur is moving the knee is externally rotated 10 degrees when fully extended..")
6
1- shape of medial femoral condyle: as it curves 30 degree laterally as it approaches the intercondylar grove. And as and extends further anteriorly than the lateral condyle. Thus tibia must follow this path during tibial on femoral extension. 2- passive tension in the anterior cruciate ligament 3- lateral pull of quadriceps tendon.

8
The popliteus is an internal rotator and flexor of the knee joint. As internal rotator, the popliteus is considered the key to the knee. As the extended and locked knee prepares to flex (e.g. when beginning to descend into a squat position), the popliteus provides an internal rotation torque that help mechanically to unlock the knee. In this position the femur is externally rotated on tibia, this action on femur is readily seen by this figure showing line of pull of popliteus
, the popliteus provides an internal rotation torque that help mechanically to unlock the knee. In this position the femur is externally rotated on tibia, this action on femur is readily seen by this figure showing line of pull of popliteus.")
9
Normal genu valgum: normal alignment is distal end of femur makes an angle of 170 -175 with the mechanical axis. 1- Changes Frontal plane knee joint alignment:

10
A) Excessive Genu valgum : The medial condyle is enlarged and the lateral condyle is diminished and flattened. Effects of genu valgum: -The weight bearing line is placed on the outer side of the knee effects -Strain on medial collateral ligament. -Osteoarthritis in later stages.

11
B) Genu varum: There is deflection in the axis of tibia in varus and inward in relation to the femur Effects of genu varum: -The subtalar joint goes into inversion to adapt the sole on the ground -Strain on the lateral collateral ligament -Osteoarthritis in later stages.
 Genu varum: There is deflection in the axis of tibia in varus and inward in relation to the femur Effects of genu varum: -The subtalar joint goes into inversion to adapt the sole on the ground -Strain on the lateral collateral ligament -Osteoarthritis in later stages.")
12
1- Surgery: a) “High Tibial (wedge) Osteotomy” Removal of a wedge of bone to correct a (varus) deformity. b) Knee transplantaion 2- Conservative: laterally wedged foot insoles decrease the varus torque on the knee and therby decrease the load on the medial compartement
 Knee transplantaion 2- Conservative: laterally wedged foot insoles decrease the varus torque on the knee and therby decrease the load on the medial compartement.")
13
Hyper extension beyond 10 degrees is called genu recarvatum. The primary cause is a chronic over powering knee extensor torque that eventually over stretches the posterior structures in the knee. This torque may be caused by poor postural control or from neuromuscul- -ar disease that causes spasticity in quadriceps and or paralysis of knee flexors, or spastic planter flexors.

Similar presentations

 by Susan J. Hall, Ph.D.>")






 articulating with 2 concave surfaces (tibia) Poor bony stability Stability increased.>")





 practical section>")
>")

>")


