Download presentation
Presentation is loading. Please wait.

1
TORCH infections and HIV/AIDS in newborn - diagnostic, treatment and prophylaxis.
Prof. Pavlyshyn H.A.

2
TORCH Infections Index of Suspicion T=toxoplasmosis O=other (syphilis)
R=rubella C=cytomegalovirus (CMV) H=herpes simplex (HSV) When do you think of TORCH infections? IUGR infants HSM Thrombocytopenia Unusual rash Concerning maternal history “Classic” findings of any specific infection Index of Suspicion
 H=herpes simplex (HSV) When do you think of TORCH infections IUGR infants. HSM. Thrombocytopenia. Unusual rash. Concerning maternal. history. Classic findings of any specific infection. Index of Suspicion.")
4
Toxoplasmosis Caused by protozoan – Toxoplasma gondii
Domestic cat is the definitive host with infections via: Ingestion of cysts (meats, garden products) Contact with oocysts in feces Much higher prevalence of infection in European countries (ie France, Greece) Acute infection usually asymptomatic 1/3 risk of fetal infection with primary maternal infection in pregnancy Infection rate higher with infxn in 3rd trimester Fetal death higher with infxn in 1st trimester
 Contact with oocysts in feces. Much higher prevalence of infection in European countries (ie France, Greece) Acute infection usually asymptomatic. 1/3 risk of fetal infection with primary maternal infection in pregnancy. Infection rate higher with infxn in 3rd trimester. Fetal death higher with infxn in 1st trimester.")
6
Clinical Manifestations
Most (70-90%) are asymptomatic at birth Classic triad of symptoms: Chorioretinitis Hydrocephalus Intracranial calcifications Other symptoms include fever, rash, HSM, microcephaly, seizures, jaundice, thrombocytopenia, lymphadenopathy Initially asymptomatic infants are still at high risk of developing abnormalities, especially chorioretinitis
 are asymptomatic at birth. Classic triad of symptoms: Chorioretinitis. Hydrocephalus. Intracranial calcifications. Other symptoms include fever, rash, HSM, microcephaly, seizures, jaundice, thrombocytopenia, lymphadenopathy. Initially asymptomatic infants are still at high risk of developing abnormalities, especially chorioretinitis.")
9
Treatment Symptomatic infants Asymptomatic infants
Pyrimethamine (with leucovorin rescue) and sulfadiazine Treatment for 12 months total Asymptomatic infants Course of same medications Improved neurologic and developmental outcomes demonstrated (compared to untreated pts or those treated for only one month)
 and sulfadiazine. Treatment for 12 months total. Asymptomatic infants. Course of same medications. Improved neurologic and developmental outcomes demonstrated (compared to untreated pts or those treated for only one month)")
10
Syphilis Clinical Manifestations
Early congenital (typically 1st 5 weeks): Cutaneous lesions (palms/soles) HSM Jaundice Anemia Snuffles Periostitis and metaphysial dystrophy Funisitis (umbilical cord vasculitis) Late congenital: Frontal bossing Short maxilla High palatal arch Hutchinson teeth 8th nerve deafness Saddle nose Perioral fissures Can be prevented with appropriate treatment
: Cutaneous lesions (palms/soles) HSM. Jaundice. Anemia. Snuffles. Periostitis and metaphysial dystrophy. Funisitis (umbilical cord vasculitis) Late congenital: Frontal bossing. Short maxilla. High palatal arch. Hutchinson teeth. 8th nerve deafness. Saddle nose. Perioral fissures. Can be prevented with appropriate treatment.")
12
Treatment Penicillin G is THE drug of choice for ALL syphilis infections Maternal treatment during pregnancy very effective (overall 98% success) Treat newborn if: They meet CDC diagnostic criteria Mom was treated <4wks before delivery Mom treated with non-PCN med Maternal titers do not show adequate response (less than 4-fold decline)
")
13
Rubella Clinical Manifestations
Sensorineural hearing loss (50-75%) Cataracts and glaucoma (20-50%) Cardiac malformations (20-50%) Neurologic (10-20%) Others to include growth retardation, bone disease, HSM, thrombocytopenia, “blueberry muffin” lesions
 Cataracts and glaucoma (20-50%) Cardiac malformations (20-50%) Neurologic (10-20%) Others to include growth retardation, bone disease, HSM, thrombocytopenia, blueberry muffin lesions.")
14
“Blueberry muffin” spots representing extramedullary hematopoesis

16
Treatment Diagnosis Prevention…immunize, immunize, immunize!
Maternal IgG may represent immunization or past infection - Useless! Can isolate virus from nasal secretions Less frequently from throat, blood, urine, CSF Serologic testing IgM = recent postnatal or congenital infection Rising monthly IgG titers suggest congenital infection Diagnosis after 1 year of age difficult to establish Treatment Prevention…immunize, immunize, immunize! Supportive care only with parent education

17
Cytomegalovirus (CMV)
90% are asymptomatic at birth! Up to 15% develop symptoms later, notably sensorineural hearing loss Symptomatic infection SGA, HSM, petechiae, jaundice, chorioretinitis, periventricular calcifications, neurological deficits >80% develop long term complications Hearing loss, vision impairment, developmental delay

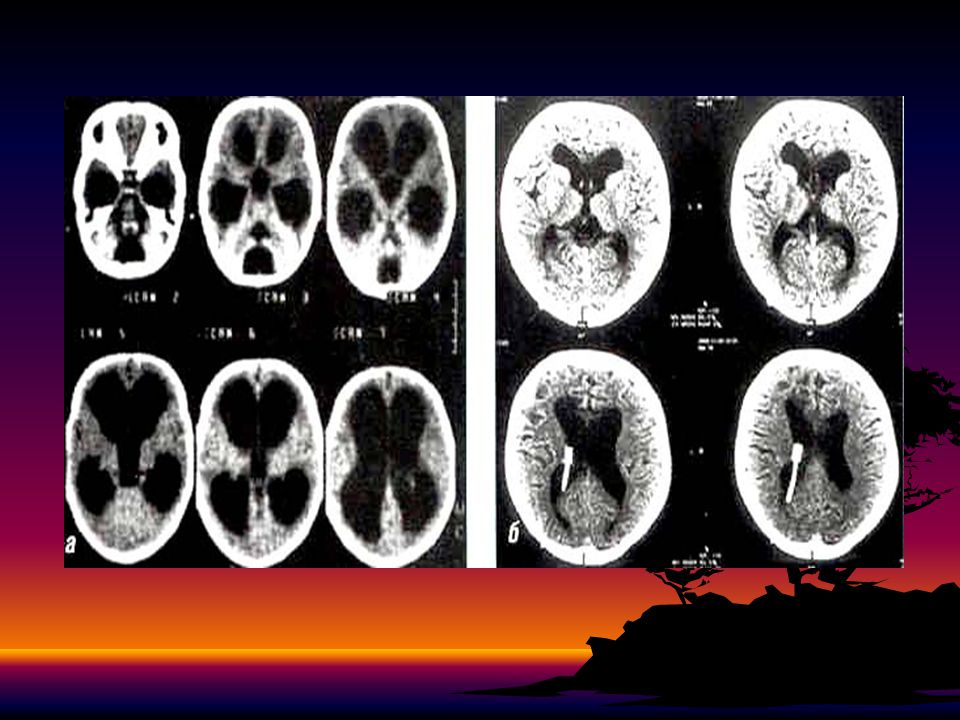
19
Ventriculomegaly and calcifications of congenital CMV

21
Diagnosis Maternal IgG shows only past infection
Infection common – this is useless Viral isolation from urine or saliva in 1st 3weeks of life Afterwards may represent post-natal infection Viral load and DNA copies can be assessed by PCR Less useful for diagnosis, but helps in following viral activity in patient Serologies not helpful given high antibody in population

22
PCR diagnostic

23
PCR diagnostic

24
Treatment Ganciclovir x6wks in symptomatic infants
Studies show improvement or no progression of hearing loss at 6mos No other outcomes evaluated (development, etc.) Neutropenia often leads to cessation of therapy Treatment currently not recommended in asymptomatic infants due to side effects Area of active research to include use of valgancyclovir, treating asx patients, etc.
 Neutropenia often leads to cessation of therapy. Treatment currently not recommended in asymptomatic infants due to side effects. Area of active research to include use of valgancyclovir, treating asx patients, etc.")
25
Clinical Manifestations
Herpes Simplex (HSV) Clinical Manifestations Most are asymptomatic at birth 3 patterns of ~ equal frequency with symptoms between birth and 4wks: Skin, eyes, mouth (SEM) CNS disease Disseminated disease (present earliest) Initial manifestations very nonspecific with skin lesions NOT necessarily present
 Clinical Manifestations. Most are asymptomatic at birth. 3 patterns of ~ equal frequency with symptoms between birth and 4wks: Skin, eyes, mouth (SEM) CNS disease. Disseminated disease (present earliest) Initial manifestations very nonspecific with. skin lesions NOT necessarily present.")
27
Diagnosis Treatment High dose acyclovir 60mg/kg/day divided q8hrs
Culture of maternal lesions if present at delivery Cultures in infant: Skin lesions, oro/nasopharynx, eyes, urine, blood, rectum/stool, CSF CSF PCR Serologies again not helpful given high prevalence of HSV antibodies in population Treatment High dose acyclovir 60mg/kg/day divided q8hrs X21days for disseminated, CNS disease X14days for SEM Ocular involvement requires topical therapy as well

29
What is HIV? Human immunodeficiency virus is the virus that causes AIDS. The human immunodeficiency virus (HIV) infects cells of the immune system - (CD4+) T cells, destroying or impairing their function. Infection with the virus results in the progressive deterioration of the immune system, leading to "immune deficiency." Infections associated with severe immunodeficiency are known as "opportunistic infections", because they take advantage of a weakened immune system. 29
 infects cells of the immune system - (CD4+) T cells, destroying or impairing their function. Infection with the virus results in the progressive deterioration of the immune system, leading to immune deficiency. Infections associated with severe immunodeficiency are known as opportunistic infections , because they take advantage of a weakened immune system. 29.")
30
Symptoms of HIV/AIDS in Children
CNS – microcephaly - progressive neurological deterioration or spastic encephalopathy - developmental delay/regression - predisposition to CNS infections Respiratory System - Recurrent infections (pneumonia, sinusitis, otitis media) - Tuberculosis - Pneumocystis carinii pneumonia (PCP) or lymphoid interstitial pneumonitis (LIP)
 - Tuberculosis. - Pneumocystis carinii pneumonia (PCP) or lymphoid interstitial pneumonitis (LIP)")
31
Clinical Features CVS – cardiomyopathy with congestive cardiac failure
GIT- AIDS enteropathy (malabsorption, infections with various pathogens) leads to chronic diarrhoea resulting in failure to thrive - Abdominal pains, dysphagia, chronic hepatitis, pancreatitis Renal – AIDS nephropathy: the most common presentation being nephrotic syndrome Skin – Eczema, seborrheic dermatitis, candida infections, molluscum contagiosum, anogenital warts
 leads to chronic diarrhoea resulting in failure to thrive. - Abdominal pains, dysphagia, chronic hepatitis, pancreatitis. Renal – AIDS nephropathy: the most common presentation being nephrotic syndrome. Skin – Eczema, seborrheic dermatitis, candida infections, molluscum contagiosum, anogenital warts.")
Similar presentations










 Infection>")




>")










 – presence of severe birth defects in babies born to mothers who drink alcohol during pregnancy. Includes damage.>")
>")
