Download presentation
Presentation is loading. Please wait.

1
Case Base Cardiology 4.17.2014 kyavar md facc

2
No 1

3
A 75 year old woman with Recent orthopnea Chronic dyspnea Fatigue Recent orthopnea palpitation Pedal edema

6
LA LV AO Diastole

7
Mitral Stenosis: Physical Exam First heart sound (S1) is loud and snapping Opening snap (OS) Low pitch diastolic rumble at the apex Pre-systolic accentuation (esp. if in sinus rhythm) S1 S2 OS S!
 S1 S2 OS S!.")
8
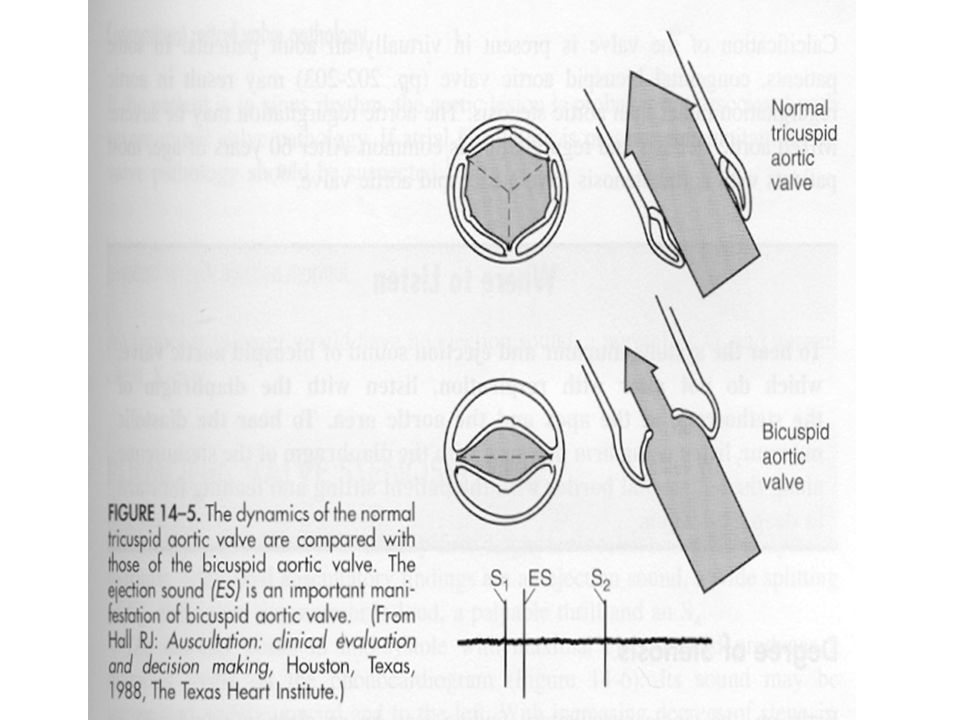
MS MR/TR/VSD AS with ES PS with ES AR MS with OS PDA S1S2

9
Mitral Stenosis: Investigations CXR ECG Echo

13
Mitral Stenosis Etiology Natural history Symptoms Physical Exam Severity Timing of Surgery

14
Mitral Stenosis: Etiology Primarily a result of rheumatic fever (~ 99% of MV’s @ surgery show rheumatic damage ) Scarring & fusion of valve apparatus Rarely congenital Pure or predominant MS occurs in approximately 40% of all patients with rheumatic heart disease Two-thirds of all patients with MS are female.
 Scarring & fusion of valve apparatus Rarely congenital Pure or predominant MS occurs in approximately 40% of all patients with rheumatic heart disease Two-thirds of all patients with MS are female.")
15
Mitral Stenosis: Natural History Progressive, lifelong disease, Usually slow & stable in the early years. Progressive acceleration in the later years 20-40 year latency from rheumatic fever to symptom onset. Additional 10 years before disabling symptoms

16
Mitral Stenosis: Pathophysiology Right Heart Failure: Hepatic Congestion JVD Tricuspid Regurgitation RA Enlargement Pulmonary HTN Pulmonary Congestion Atrial Fib LA Thrombi LA Enlargement LA Pressure RV Pressure Overload RVH RV FailureLV Filling

17
Jugular Veins Add 5 cm

18
Mitral Stenosis: Symptoms Breathlessness Fatigue Oedema, ascites Palpitation Haemoptysis Cough Chest pain mitral facies or malar flush Symptoms of thromboembolic complications (e.g. stroke, ischaemic limb) Worsened by conditions that cardiac output. ◦ Exertion,fever, anemia, tachycardia,, pregnancy, thyrotoxicosis
 Worsened by conditions that cardiac output. ◦ Exertion,fever, anemia, tachycardia,, pregnancy, thyrotoxicosis.")
19
Signs of Mitral Stenosis Palpation: Small volume pulse Tapping apex-palpable S1 Palpable S2 Atrial fibrillation Signs of raised pulmonary capillary pressure – Crepitations, pulmonary oedema, effusions Signs of pulmonary hypertension – RV heave, loud P 2 Auscultation: Loud S1 S2 to OS interval inversely proportional to severity Diastolic rumble: length proportional to severity In severe MS with low flow- S1, OS & rumble may be inaudible

20
What if you hear something? When does it occur? Is it systolic, diastolic, or both? – What is the pattern? Where is it loudest? Where does it radiate? Who goes with it?Are there other associated findings? – S2 splitting normal, loud P2, gallop sound? How does it respond? Maneuvers

21
A 75 year old woman with loud first heart sound and mid-diastolic murmer

23
No 2

24
70 years old man with PND Syncope Chest pain

26
LA LV AO Systole RV

28
Valve Stenoses Two Catheter Technique

30
Ejection Murmur Mixed frequencies and is moderate-to-marked crescendo-decrescendo Caused by forward flow across the left or right outflow Aortic stenosis & pulmonic stenosis

33
No 3

34
Patient with Purplish lips, hands and feet History: 6 week old male with 2 days of clear, nasal congestion, no fever Gets bluish after feeding or crying Previously well, full-term baby The family history was negative

35
Tetralogy of Fallot- Clinical Findings squatting “Tet spells” – due to pulmonary outflow tract spasm Severe cases ---at birth---severe PS Mild cases ---- much later---mild PS Cyanosis usually ECG reveals right ventricular hypertrophy

37
Physical Examination Central Cyanosis vs. Peripheral cyanosis Vital signs Lung and CNS examination to rule these out Cardiac Examination Heaves, thrills, abnormal or increased precordial activity Absent or diminished femoral pulses Abnormal first or second heart sound (abnormal splitting) Extra heart sounds (gallop, ejection click, opening snap) Murmurs that are loud, harsh, blowing
 Extra heart sounds (gallop, ejection click, opening snap) Murmurs that are loud, harsh, blowing.")
38
Case Presentation cont’d Purplish lips, hands and feet Grade III/VI systolic murmur loudest at lower left sternal border Liver was 1.5 cm below right costal margin and a normal spleen Peripheral pulses equal in upper/lower extremities, 1.5 sec cap refill

40
Lab/Imaging Studies CBC/Sepsis evaluation Chest x-ray Oxygen Saturation (Arterial blood gas, pulse oximetry) Hyperoxia test Electrocardiogram Echocardiography
 Hyperoxia test Electrocardiogram Echocardiography")
42
Hyperoxia test- Cardiac or Pulmonary? 50-150mm Hg Truncus Arteriosus ( No restricted pulmonary blood flow) <50 mm Hg Tetralogy of Fallot, Tricuspid Atresia ( Reduced pulmonary flow) <150 mm HgCardiac disease or PPHN (SHUNT) >150mm HgPulmonary disease (V/Q mismatch) On 100% oxygenpaO2
 <50 mm Hg Tetralogy of Fallot, Tricuspid Atresia ( Reduced pulmonary flow) <150 mm HgCardiac disease or PPHN (SHUNT) >150mm HgPulmonary disease (V/Q mismatch) On 100% oxygenpaO2.")
43
TOF - ECG

44
Brickner, M. E. et al. N Engl J Med 2000;342:334-342 Tetralogy of Fallot 5/10k births Ventricular septal defect Narrowing of the pulmonary outflow tract Over riding aorta right ventricular hypertrophy

45
Hypoxemia Differential Right-to-Left Shunt INTRACARDIAC, Great Vessels, pulmonary AV malformation V/Q Mismatch Pneumonia, atelectasis, aspiration, pulmonary hypoplasia Hypoventilation CNS depression, Neuromuscular disease, Airway obstruction Diffusion Impairment Pulmonary edema, pulmonary fibrosis Hemoglobinopathy

46
No4

47
A 41-year-old man was initially evaluated 6 years previously by his family physician, found to be hypertensive, and managed with pharmacologic agents. Over the next several years, control of his BP became increasingly difficult, requiring multiple agents. He was referred to a cardiologist for further evaluation. Throughout the entire period, he has remained asymptomatic.

48
Physical examination disclosed a BP of 160/94 mm Hg and a heart rate of 75 beats/min. Precordial pulsations were normal. Auscultation disclosed a late- peaking systolic murmur heard well at the apex; however, it was also heard over the entire thoracic cage and upper back (Fig 1 ). No diastolic murmurs were audible. Simultaneous palpation of the radial and femoral pulses disclosed a significant delay of the latter. The systolic pressure in the lower extremities was 130 mm Hg, determined with a Doppler probe over the pedal vessels, yielding an ankle/brachial index of 0.85. The remainder of the examination was normal.Fig 1
. No diastolic murmurs were audible. Simultaneous palpation of the radial and femoral pulses disclosed a significant delay of the latter. The systolic pressure in the lower extremities was 130 mm Hg, determined with a Doppler probe over the pedal vessels, yielding an ankle/brachial index of The remainder of the examination was normal.Fig 1.")
49
Graphic recording of murmurs as heard at two locations over the chest. Varma C et al. Chest 2003;123:1749-1752 ©2003 by American College of Chest Physicians

50
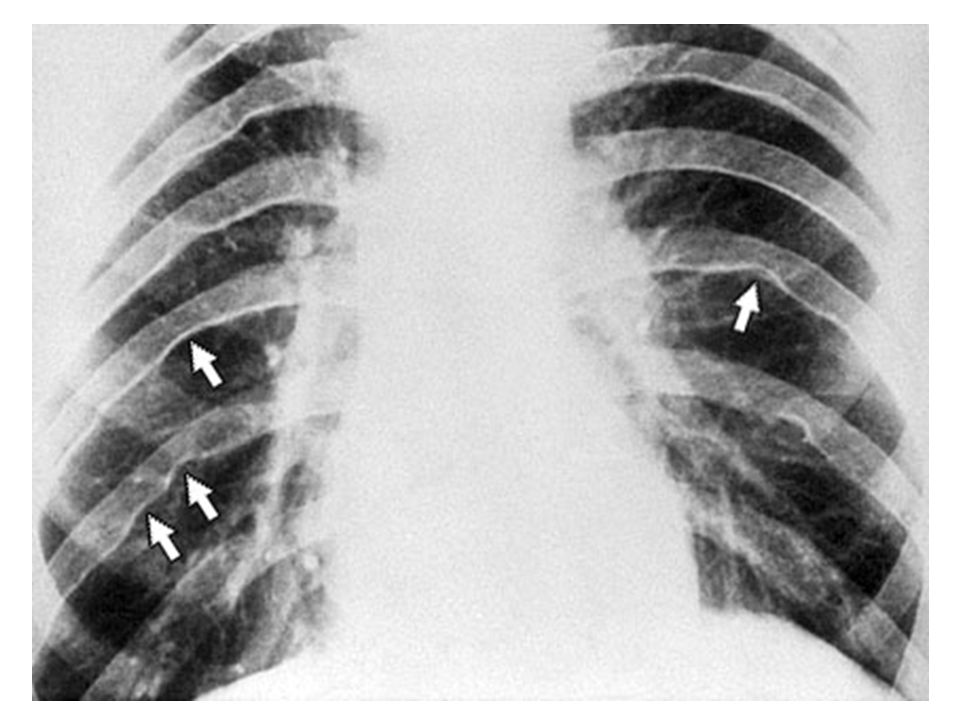
Rib notching

52
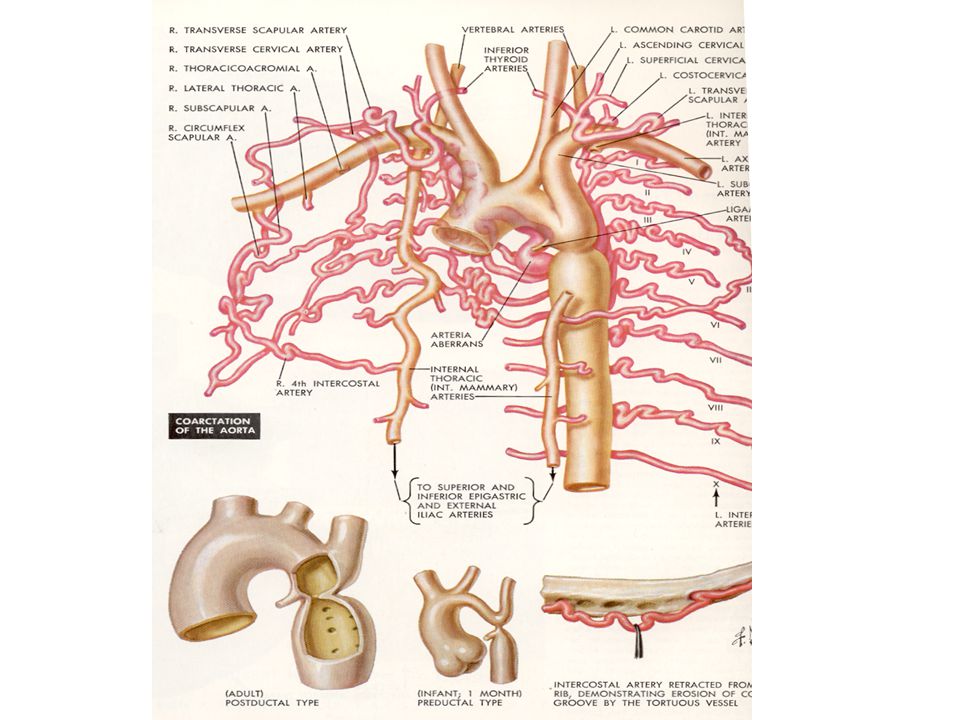
Coarctation of the Aorta Grade II or III murmur Heard posteriorly & over base of the heart Hypertension in the arms, but not in the legs Decreased or absent femoral arterial pulsation

54
Coarctation of Aorta Narrowing in proximal descending aorta May be long/tubular but most commonly discrete ridge Natural hx: poor prognosis if unrepaired – Aortic Aneurysm/dissection – CHF – Premature CADz

56
Coarctation Repair Edmunds’ Cardiac Surgery in the Adult, Ch 47 Surgical correction 1) Patch aortoplasty with removal of segment and end to end anastomosis or subclavian flap repair 2) bypass tube grafting around segment
 Patch aortoplasty with removal of segment and end to end anastomosis or subclavian flap repair 2) bypass tube grafting around segment")
57
Coarctation of Aorta Residual or recoarctation may be seen in 3% to 41% of patients and can occur with any surgical technique or after angioplasty (seen in 8% to 11% of patients undergoing angioplasty for native coarctation)
")
58
No5

59
Dyspnea & Chest Pain The patient was a 33 year old housewife who had acute cardiac failure on the sixteenth day after the onset of the disease

60
Physical examination revealed a pale thin female with tachycardia (107 beats/minute), tachypnea (22 breaths/minute), hypotension (blood pressure 86/50 mmHg), jugular venous distension with rapid “×” descent, and distant heart sounds. While the patient was being evaluated in the emergency room, she suddenly had a cardiopulmonary arrest

61
Myocarditis Myocarditis is an inflammation of the myocardium, the thick muscular layer making up the major portion of your heart. Often follows URI May present with chest pain (either pleuritic or non-specific) or signs of heart failure ECG may show sinus tachycardia, nonspecific repolarization abnormalities, and intraventricular conduction abnormalities Echocardiography documents cardiomegaly & contractile dysfunction Myocardial biopsy, although not sensitive, may reveal characteristic inflammatory pattern (ex. Giant Cell)
 or signs of heart failure ECG may show sinus tachycardia, nonspecific repolarization abnormalities, and intraventricular conduction abnormalities Echocardiography documents cardiomegaly & contractile dysfunction Myocardial biopsy, although not sensitive, may reveal characteristic inflammatory pattern (ex. Giant Cell).")
63
Myocarditis basics Wide spectrum of clinical consequences – Mild & self-limited with few symptoms or severe with progression to CHF & dilated CM – Very localized or diffuse – Clinical involvement can be limited to the heart or be part of widespread systemic disorder

64
Electrocardiogram showing PQ-segment depression and diffusely elevated ST-T-segments at presentation (A) and evolution after 1 day (B).
 and evolution after 1 day (B).")
65
ECG & CXR ECG - nonspecific ST-T changes and conduction delays are common – Ventricular ectopy may be only clinical finding CXR - cardiomegaly is frequent, may have evidence for pulmonary venous hypertension & pulmonary edema

66
Diagnostics Wbc’s often elevated ESR increased Troponins elevated in 1/3 CK-MB elevated in 10% Echocardiogram helps evaluate cardiac function & exclude other causes Cardiac MRI improving in ability to see abnormalities in myocardium

67
Endomyocardial Bx Pathologic exam may reveal lymphocytic inflammatory response with necrosis, but this is not sensitive b/c of the patchy areas of distribution. “Dallas” criteria for histopathologic dx May see “Giant cells”

69
No6

70
65 years man with sever chest pain History DM Hyperlipidemia smoking

Similar presentations



































 tricuspid valve 2. Hypoplastic right ventricle 3. Ventricular septal defect 4. Atrial.>")







