Download presentation
Presentation is loading. Please wait.

1
Senior Academic Half Day: Malignant Haematology
Beth Harrison Department of Haematology University Hospitals Coventry and Warwickshire NHS Trust

2
Normal haematopoiesis
Investigations in malignant haematology Approach to a patient with pancytopenia Diagnosis and management

3
Case 1 Hb 8.6 WCC 1.2 Platelets 12 35 year old male
6 weeks recurrent throat infections 2 weeks easy bruising Hb 8.6 WCC 1.2 Platelets 12 Pancytopenia – he will need a bone marrow examination

4
Bone Marrow Examination

5
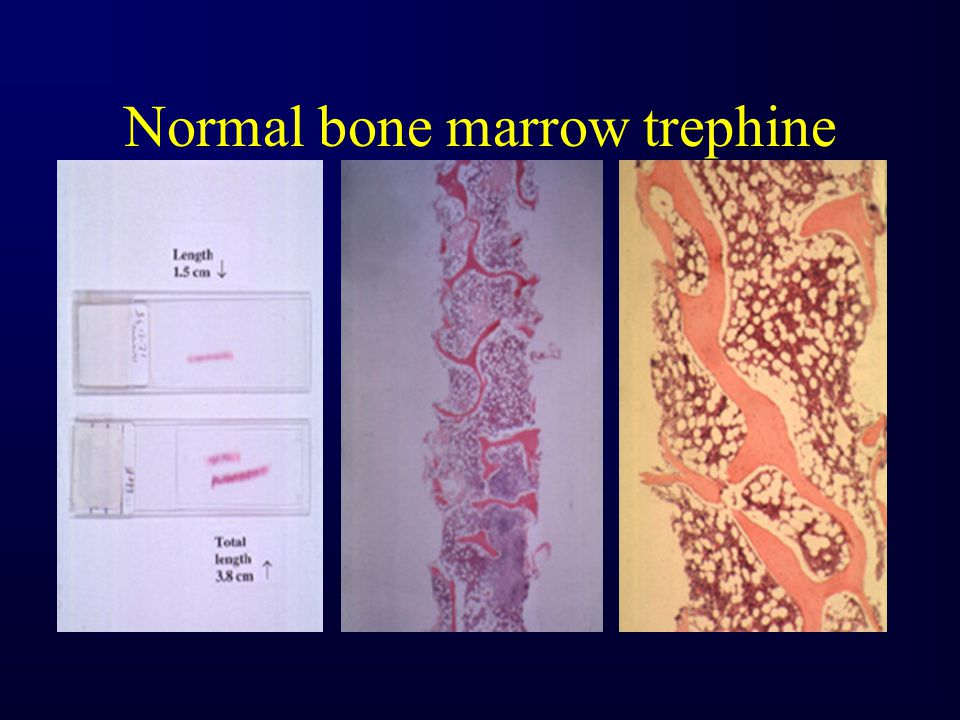
Normal Bone Marrow Aspirate

6
Normal bone marrow trephine
7
Case 1 Hb 8.6 WCC 1.2 Platelets 12 35 year old male
6 weeks recurrent throat infections 2 weeks easy bruising Hb 8.6 WCC 1.2 Platelets 12

8
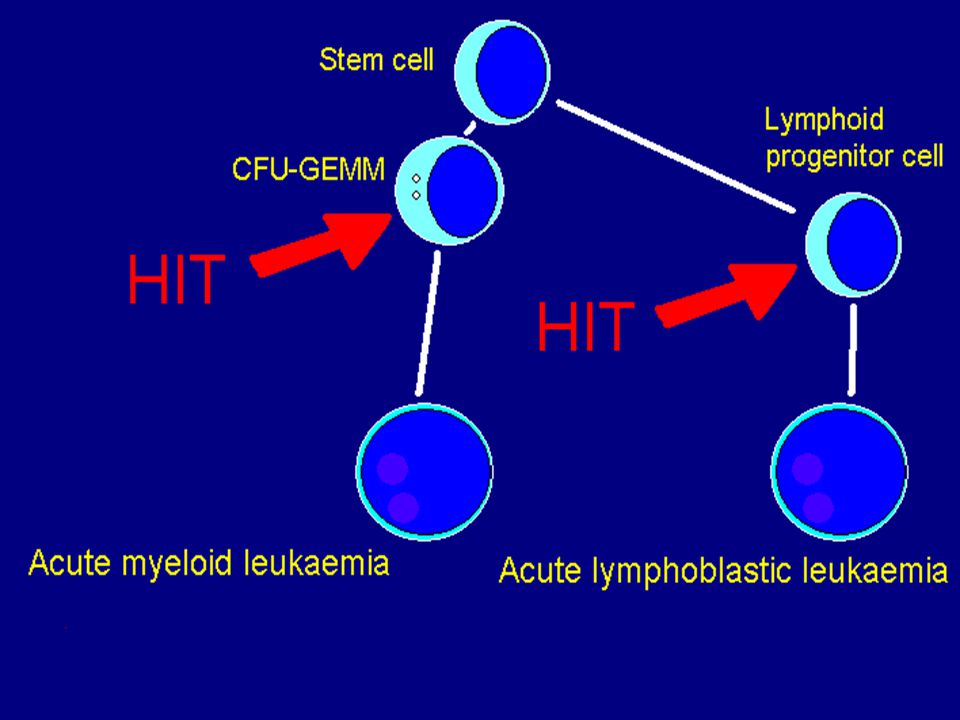
Hb 8.6 WCC Platelets 12 = Acute Leukaemia

9
What is acute leukaemia?
What is a “blast”?

11
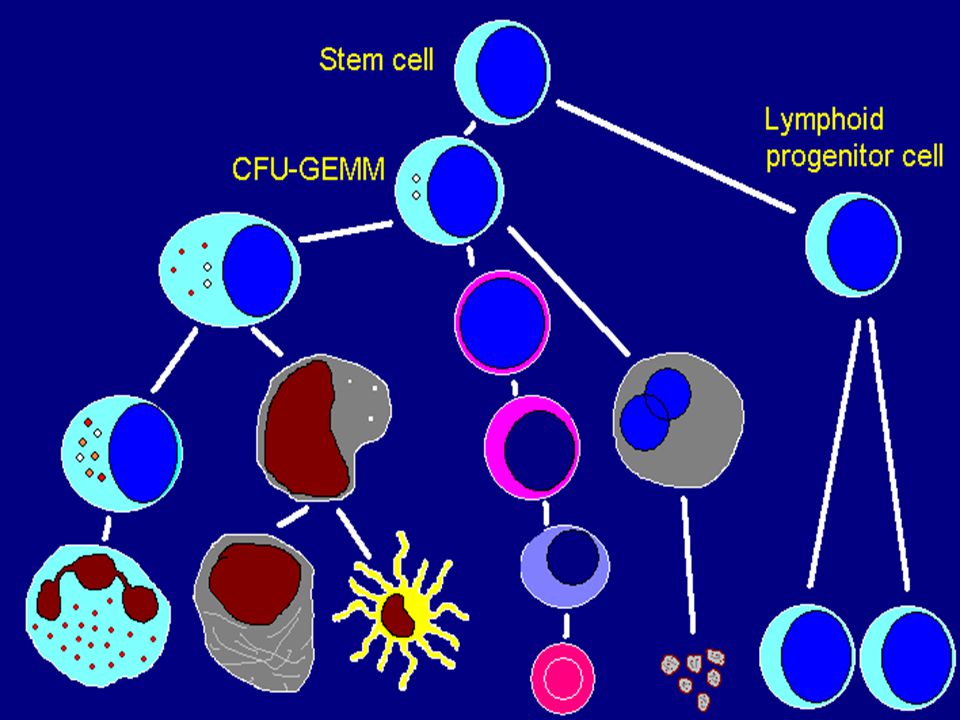
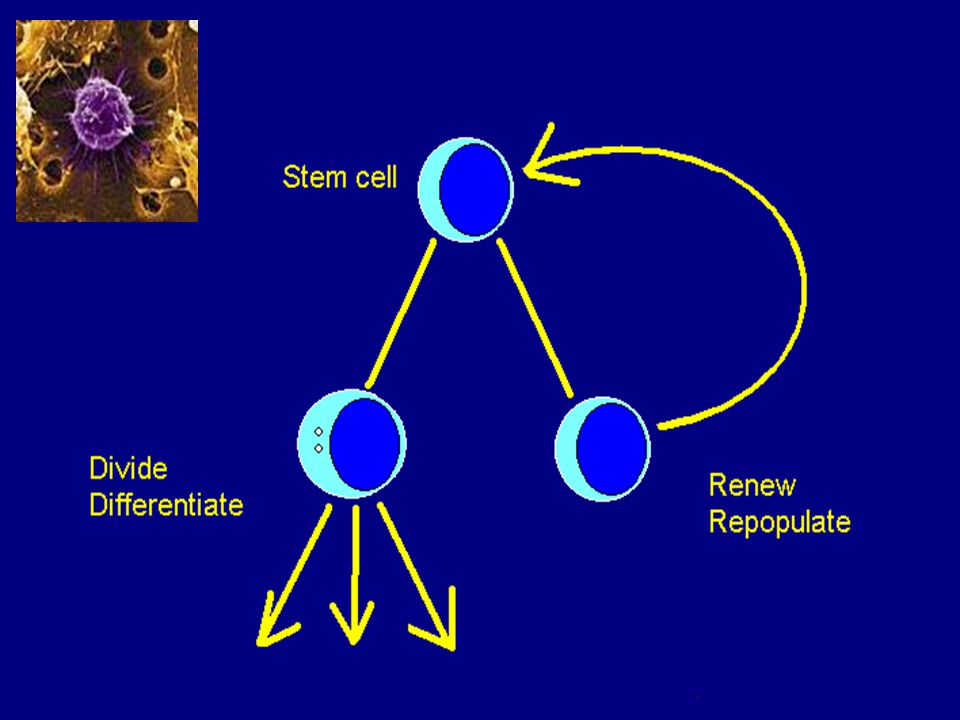
What is a stem cell?

15
Blasts in bone marrow (+blood) Molecular diagnostics
Case 1 + Diagnosis = Acute myeloid leukaemia Bone marrow failure Blasts in bone marrow (+blood) Molecular diagnostics
 Molecular diagnostics.")
16
Case 1 The Patient receives some chemotherapy Presents to A&E Pyrexial
Shivery, vomiting, diarrhoea

17
Neutropenic Sepsis

18
Neutropenic Sepsis Treat as neutropenic without waiting for FBC result
Blood cultures Broad spectrum antibiotics within 30 minutes of presentation IV fluid resuscitation Get help

19
Fungal Pneumonia – Probably Aspergillus

20
Management of acute leukaemia
Chemotherapy BUT: Filtered air No plants or flowers No unnecessary visitors Washed food – no salad or grapes or black pepper Antifungal prophylaxis Mouthcare

21
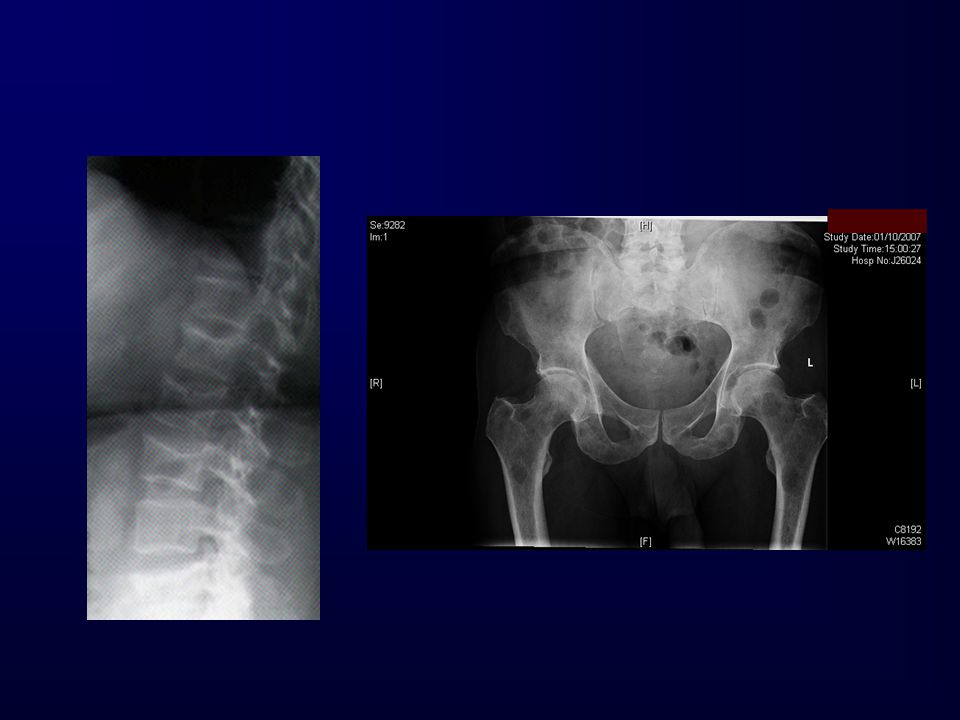
Indications for bone marrow
Diagnostic Abnormal FBC Investigation of paraproteinaemia Bone lesions in pelvis accessible by this route Pyrexia of unknown origin ? TB in HIV+ ? foreign travel / splenomegaly Isolated splenomegaly with diagnosis unclear from PB Staging Hodgkin Lymphoma / Non Hodgkin Lymphoma Treatment response Leukaemia, Myeloma, Lymphoma etc

23
Case 2 56 year old man back pain, vomiting and constipation
Na Calcium K Total protein Urea 46 Albumin Creat 565 Hb 8.7

25
Investigations: Protein electrophoresis – of what?
Bone marrow examination – for what? Skeletal survey – is what?

26
Investigations: Serum / urine electrophoresis Bone marrow examination
Skeletal survey

27
What is the diagnosis? Multiple myeloma First management issues?
Correct calcium Give fluids

28
Renal Failure in Myeloma
Light chain deposition in kidney Hypercalcaemia Hyperuricaemia Dehydration Non-steroidal anti-inflammatories Plasma cell infiltration of kidney

29
Urine free light chains: An old story
Previous polyclonal antisera against light chains could not distinguish light chains bound into whole immunoglobulin molecules from free light chains

31
Case 3 35 year old woman with 2 years of lethargy and intermittent LUQ pain now complaining of dizziness Visible white cells

32
Case 3 On examination: Massive splenomegaly Fundal haemorrhages
Diagnosis Chronic myeloid leukaemia with hyperviscosity resulting from WCC Immediate management Get the white cell count down!!

33
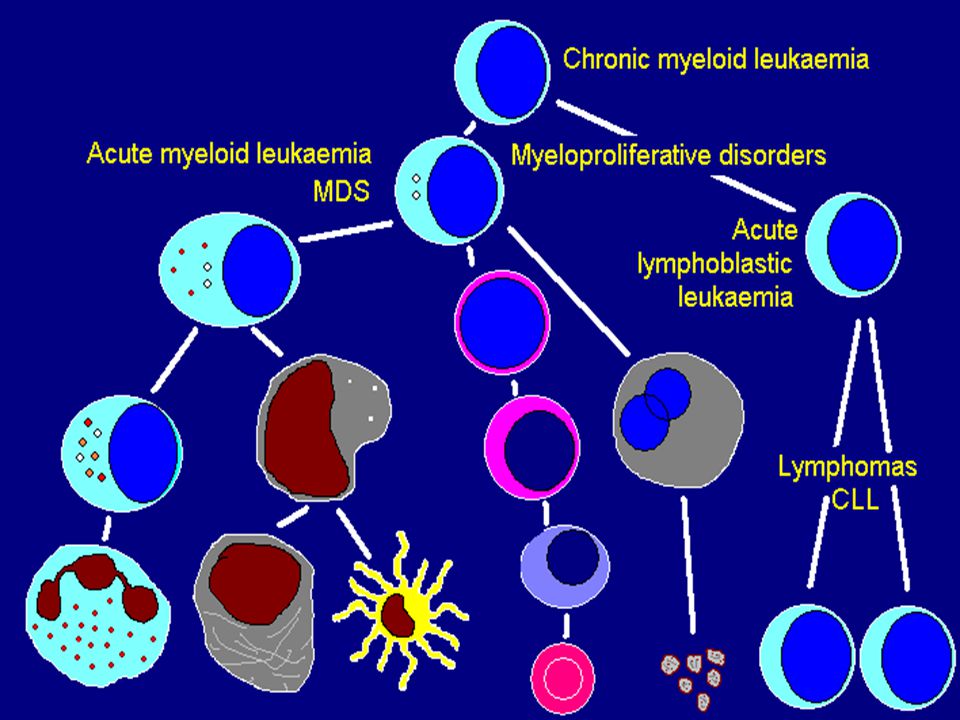
Myeloproliferative Disorders
Clonal, pre-leukaemic Uncontrolled proliferation of one or more bone marrow lineages: Red cells – primary polycythaemia Platelets – essential thrombocythaemia White cells (myeloid) – chronic myeloid leukaemia Fibroblasts - myelofibrosis
 – chronic myeloid leukaemia. Fibroblasts - myelofibrosis.")
34
Myeloproliferative Disorders
Primary Polycythaemia and Essential Thrombocythaemia: Increased vascular events Treatment is aimed at reducing these Hb>19? Plts>700? Ask!

35
Causes of hyperviscosity
Paraprotein (IgM > IgA > IgG) High WCC (CML / AML > CLL) High red cell mass (polycythaemia) Raised platelet count (>1,000, myeloproliferative rather than reactive)
 High WCC (CML / AML > CLL) High red cell mass (polycythaemia) Raised platelet count. (>1,000, myeloproliferative rather than reactive)")
36
Causes of splenomegaly
Haematological Chronic myeloid leukaemia, Myelofibrosis Chronic lymphatic leukaemia Acute lymphoblastic leukaemia Lymphoma (various) Infective EBV Chronic malaria Visceral Leishmaniasis Liver Other HCV / HBV with portal hypertension Any cause cirrhosis with portal hypertension
 Infective. EBV. Chronic malaria. Visceral Leishmaniasis. Liver Other. HCV / HBV with portal hypertension. Any cause cirrhosis with portal hypertension.")
38
Case 4

40
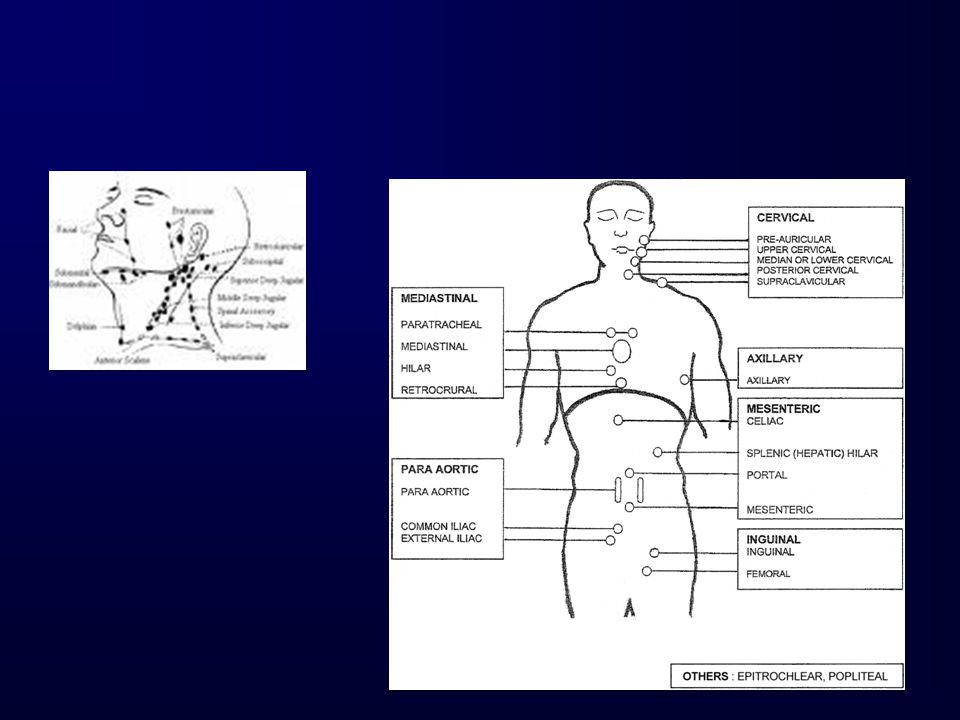
Indications for lymph node biopsy
Generalised lymphadenopathy, FBC unhelpful. (Also palpable cervical LN with mediastinal LN on CXR) Isolated lymphadenopathy – no obvious pathology in the anatomical region drained (ENT: nasendoscopy NAD, FNA unhelpful) Regional lymphadenopathy with obvious primary pathology inaccessible to biopsy
 Isolated lymphadenopathy – no obvious pathology in the anatomical region drained. (ENT: nasendoscopy NAD, FNA unhelpful) Regional lymphadenopathy with obvious primary pathology inaccessible to biopsy.")
41
Findings on lymph node biopsy?
Reactive Necrotic Granulomatous – TB, Sarcoid? HIV? Metastatic Carcinoma Metastatic Melanoma Lymphoma

42
Non-Hodgkin’s Lymphoma: T cell
Hodgkin Lymphoma Non-Hodgkin’s Lymphoma: B cell

43
Case 4 Nodular Sclerosing Hodgkin Lymphoma

44
Case 4 Treatment: Chemotherapy Radiotherapy Risks of treatment:
Breast cancer Thyroid cancer Secondary leukaemia / myelodysplasia Infertility Other endocrine failure - early menopause Bones Cardiac damage (chemo + radiotherapy) Risks of treatment?
 Risks of treatment")
46
Intraabdominal lymphoma

47
PET-CT in staging lymphoma

48
PET-CT in staging lymphoma

49
Indolent Non-Hodgkin Lymphoma: localised to one site

50
Aggressive Non-Hodgkin Lymphoma

51
Thank you

Similar presentations






1 CHILDHOOD LEUKAEMIA. TA OGUNLESI (FWACP)2 LEUKAEMIA Heterogenous group of malignant disorders Characterised by uncontrolled clonal.>")

 Idiopathic Associated with other diseases (autoimmune, infectious, non-heme.>")
 CHEMOTHERAPY Adult Medical-Surgical Nursing.>")








:>")




