Download presentation
Presentation is loading. Please wait.

1
Stem Cell Transplantation H. Atilla Özkan, MD.

2
The Nobel Prize, 1990 E. Donnall Thomas first succsessful HSCT in treatment of acute leukemias Thomas ED, Lochte HL, Lu WC, Ferrebee JW. Intravenous infusion of bone marrow in patients receiving radiation and chemotherapy. N. Engl. J. Med. 1957; 257: 491.

3
08.05.2015 3

4
Definition Infusion of hematopoietic stem cells from oneself or another person Usually follows high dose chemotherapy and/or irradiation

6
CD34+ CD38- CD38+ 6

7
Hematopoietic Stem Cell Transplantation 1. Hematologic Malignancies Acute and Chronic Myeloid Leukemia Acute and Chronic lymphocytic leukemia Myeloddysplastic Syndrome Lymphomas – Hadgkins and Non Hodgkins Multiple Myelomas 2. Non Malignant Disorders Severe Aplastic Anemias (SAA) Hurler’s Syndrome Wiskott – Aldrich Syndrome Diamond – Blackfan Anemia Osteopetrosis 3. Inherited Blood Disorders Beta Thalassaemia Major 4. Severe combined immunodeficiency (SCID) 5. Pathologic States including autoimmune diseases 6. Solid Tumors (Breast cancer, Teratomas, ovarian tumors etc.)
 Hurler’s Syndrome Wiskott – Aldrich Syndrome Diamond – Blackfan Anemia Osteopetrosis 3. Inherited Blood Disorders Beta Thalassaemia Major 4. Severe combined immunodeficiency (SCID) 5. Pathologic States including autoimmune diseases 6. Solid Tumors (Breast cancer, Teratomas, ovarian tumors etc.).")
8
Stem Cell Sources

9
9 Hematopoietic Nich

10
10

11
11

12
PBSC Collection

13
BoneMarrow Harvest

15
Peripheral blood stem cell mobilization 1.G-CSF 2.G-CSF + Plerixafor (Mozobil) 3.Chemotherapy + G-CSF 4.Chemotherapy + G-CSF + Plerixafor
 3.Chemotherapy + G-CSF 4.Chemotherapy + G-CSF + Plerixafor")
19
Mobilization of Stem Cells Goal collection: > 2 x 10 6 cells/kg (auto-SCT) > 5 x 10 6 cells/kg (allo-SCT)
 > 5 x 10 6 cells/kg (allo-SCT)")
20
Factors Influencing Successful Mobilization Pelvic or abdominal irradiation Marrow hypocellularity Prior stem cell toxic agents Prior no of chemo. regimens Age Type of underlying disease

21
Autologous BMT Reinfusion of patient’s own cells Regimens do not include immunosuppression Older patients Worry about reinfusion of cancer cells Chemotherapy associated toxicity

22
Allogeneic BMT Reinfusion of someone else’s (donor) cells into patient (recipient) Regimens usually aggressive and contain immunosuppression Younger patients Finding a HLA-matched donor is difficult GVHD and infectious complications Chemotherapy toxicity
 cells into patient (recipient) Regimens usually aggressive and contain immunosuppression Younger patients Finding a HLA-matched donor is difficult GVHD and infectious complications Chemotherapy toxicity")
23
Allogeneic BMT HLA Matched sibling HLA matched unrelated donor (MUD) HLA mismatched related donor HLA mismatched unrelated donor
 HLA mismatched related donor HLA mismatched unrelated donor")
24
Compatible Donor Search - Matching HLA Family- ¼ chance Unrelated – 1/500 - 0/10 million chance of match 70% patients do not have family donor

25
Chromosome 6 Gene map of the HLA region Class II Class III Class I 1.8 Mb 40 % of which have assumed immune functions tel. Long arm cen. short arm tel. tel. Long arm cen. short arm tel. 6p 21.3 HLA region Bf DPDMDQDR C4 C2Hsp70TNF B C E A G F B C E A G F 128 functional genes Most polymorphic Ag presentation, crucial in organ and HSCT

28
Syngeneic BMT Reinfusion of identical twin’s cells Need to insure twins are identical

29
Deciding on type of SCT Type and stage of disease Availability of stem cells Age Performance status Clinical condition of patient

31
Preparative Regimen Purpose Kill tumor cells Provide space in marrow Suppress immune system

32
Components of Ideal Regimen Myeloablative Immunosuppressive Non-overlapping toxicities

33
Myeloablative Regimens Cyclophosphamide/TBI Busulfan/Cyclophosphamide Carmustine/Etoposide/Cytarabine/Cyclophosph amide Carmustine/Etoposide/Cytarabine/Melphalan Melphalan

34
Nonmyeloablative Regimens Fludarabine/Melphalan Fludarabine/cyclophosphamide Fludarabine/busulfan

36
Regimen Related Toxicities Nausea/vomiting Diarrhea Mucositis Myelosuppression Electrolyte abnormalities Pulmonary Hemorrhagic cystitis Sterility Cardiomyopathy Hepatotoxicity Nephrotoxcitiy Peripheral neuropathies Ototoxicity Secondary malignancies Infections

38
Hepatic Veno-occlusive Day +14 - 28 Hyperbilirubinemia Weight gain Ascites Hepatomegaly

39
Infectious Complications Bacterial Fungal CMV VZV PCP

42
Graft Versus Host Disease (GVHD) Reaction of donor T-cells against host tissues PBSCT or BMT Blood transfusions Billingham criteria Graft must contain immunocompetent cells Recipient must express antigens not present in donor Recipient incapable of mounting immune response against graft
 Reaction of donor T-cells against host tissues PBSCT or BMT Blood transfusions Billingham criteria Graft must contain immunocompetent cells Recipient must express antigens not present in donor Recipient incapable of mounting immune response against graft")
43
Pathophysiology Afferent phase Recipient tissues active donor T lymphocytes Antigen presentation T cell activation Proliferation and differentiation of T cells Efferent phase Attack of donor cells on host target tissues Activated T cells secrete cytokines Secondary effector cells damage tissues

44
Acute GVHD Occurs in 25-70% of all BMT patients Graded based on combination of severity of presentation Survival based on grade (0-90%) Death usually due to infections, hemorrhage or organ failure
 Death usually due to infections, hemorrhage or organ failure")
45
Risk Factors MHC disparity (Histocompatibility) Age Sex mismatch CMV serology Intensity of preparative regimen Prior donor transfusions Disease stage
 Age Sex mismatch CMV serology Intensity of preparative regimen Prior donor transfusions Disease stage")
46
aGVHD Prevention Cyclosporine Tacrolimus Methylprednisolone Methotrexate Cyclophosphamide ATG

47
aGVHD Treatment Methylprednisolone Antithymocyte globulin Supportive care Monoclonal antibodies PUVA Thalidomide

48
Chronic GVHD Incidence 15-60% Increased risk if AGVHD Skin Mucosal changes Esophageal strictures Liver disease Thrombocytopenia

49
cGVHD Treatment Prednisone Cyclosporine Supportive care Other PUVA Photopheresis Thalidomide Mycophenolate mofetil

50
Late BMT Complications Endocrine dysfunction Pulmonary fibrosis Sterility Cataract formation Infections

52
Otolog Hematopoetik Kök Hücre nakli endikasyonları Malign hastalıklar: AML, HL, NHL, KLL Myeloma, Germ hücreli tümör, nöroblastoma, medullablastoma Malign hastalıklar dışı: Otoimmün hastalıklar, Amiloidozis

53
Allojeneik Hematopoetik Kök Hücre nakli endikasyonları Malign hastalıklar: AML,ALL, MDS HL, NHL, KML, KLL Myeloma, Malign hastalıklar dışı: Otoimmün hastalıklar, orak hücreli anemi, aplastik anemi, fankoni anemi, thal majör, wiskot aldrich, PNH, osteopetrozis, ciddi kombine immün yetmezlik

54
HKHN neyi sağlar? Kemik iliği yetmezliği durumlarında normal hematopoezin oluşmasını sağlar Hastalıklı kemik ilğinin yerini sağlıklı kemik iliği alır Kemik ilği ablasyonu sonrası tekrar hematopoezi sağlar Konjenital immün yetmezlikleri düzeltir Graft versus tümör etkisi sağlar 08.05.2015 54

55
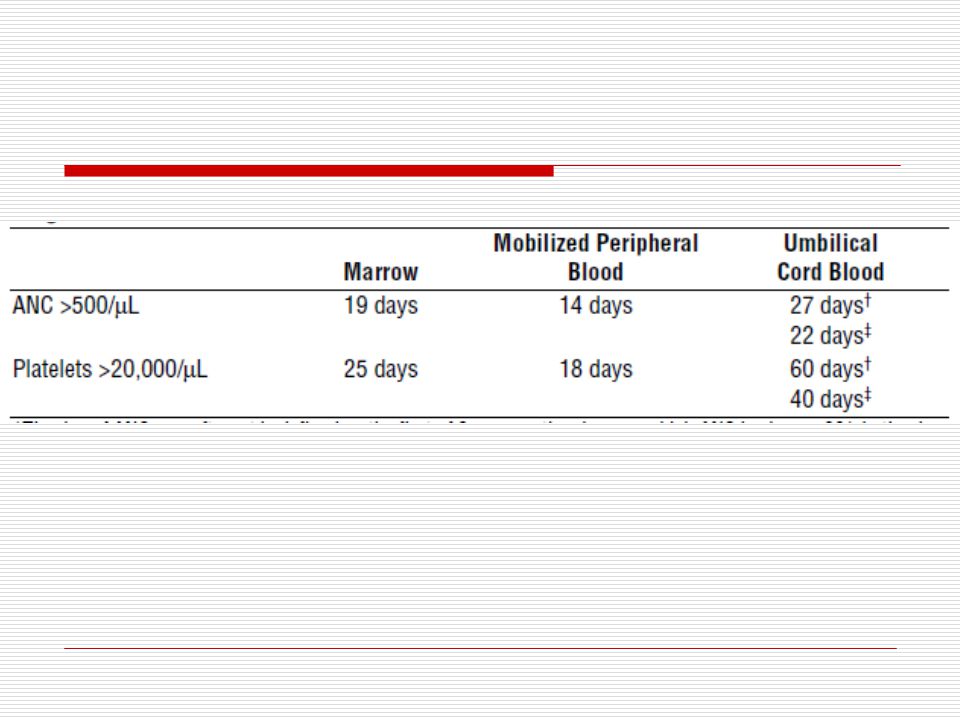
Bone Marrow Engraftment Transfusion support Longer hospital stay # stem cells # T cells Acute GVHD Chronic GVHD

56
PBSC Engraftment Transfusion support Shorter hospital stay # stem cells # T cells Acute GVHD Chronic GVHD

58
Reinfusion of Cells

Similar presentations























 Overview Willis H Navarro, MD Medical Director, Transplant Services, NMDP Associate Clinical Professor,>")


 the immunology goes two ways. There is host vs. graft.>")


 Medical Director Cancer Transplant Institute Virginia G. Piper Cancer Center Everything You Ever Wanted to Know About Transplant.>")


