Download presentation
Presentation is loading. Please wait.

1
Anesthesia for Cardiothoracic Trauma Charles E. Smith, MD Department of Anesthesia MetroHealth Medical Center Case Western Reserve University Cleveland, Ohio Email: csmith@metrohealth.org

2
Objectives Incidence Pathophysiology Specific injuries

3
ATLS Provider Manual Trauma Leading cause of death, ages 1 - 44 yrs 60 million injuries annually in USA –30 million require medical care –3.6 million require hospitalization –9 million are disabling 300 k = permanent; 8.7 million= temporary Costs are staggering: > $100 billion annually, or 40% of health care $

5
Cardiothoracic Injuries Accounts for 20% trauma deaths in US Contributing factor in additional 25% Immediate deaths: massive injury heart, great vessels, lungs Early deaths: airway, hypoxia, hemorrhage, tamponade, aspiration

6
Pathophysiology Respiratory insufficiency + hypoxia –chest wall injury, rib fx, flail, airway –hemothorax, pneumo, contusion, aspiration Hemodynamic collapse + shock –massive hemothorax –cardiogenic shock: tamponade or blunt cardiac –mediastinal shock: tension pneumo

7
Siegel JH et al: Trauma: Emergency Surgery + Critical Care, 1987:201-284

8
Devitt: CJA 1991;38:506. Incidence of injuries in patients presenting to OR emergently Blunt Chest Injuries

9
Besson + Saegesser 1983; Switzerland, N= 1485 chest injuries Blunt Chest Trauma: Extra-thoracic Injuries

10
Initial Evaluation History of traumatic event: –mechanism of injury: mva, mca, assault, fall, blasts, pedestrian struck, gsw, stab –energy exchange: speed of vehicle, distance of fall, weapon caliber, entry + exit wounds Review of systems: –allergies, meds, PMH, last meal, events before + after injury: AMPLE

11
1 o Survey Airway + c-spine control Breathing, O 2 sat Circulation, pulse, stop external bleeding Disability: Rapid neuro exam –alert, v. responds to verbal, to pain, unresponsive Exposure/ environmental control

12
2 o Survey Rest of vital signs Physical exam Xrays: lat c-spine, chest, pelvis FAST, DPL, CT, other studies Done only after 1 o survey completed + resuscitation begun

13
Case: Hemopneumothorax 26 yo female, initially stable after high speed MVA During CT, had dyspnea, tachypnea, tachycardia, hypotension, BS left Transferred emergently to OR

15
Hemothorax Which is true? 1.Bleeding usually continues after chest tube insertion + lung re-expansion 2.Respiratory failure + shock may occur 3.Hypoxia, breath sounds + hyper-resonance to percussion are usual findings 4.Hemothorax is unlikely to occur in the setting of penetrating thoracic trauma 5.Emergency thoracotomy + OLV often required

16
Blunt thoracoabdominal trauma, hemopneumo, fx ribs

17
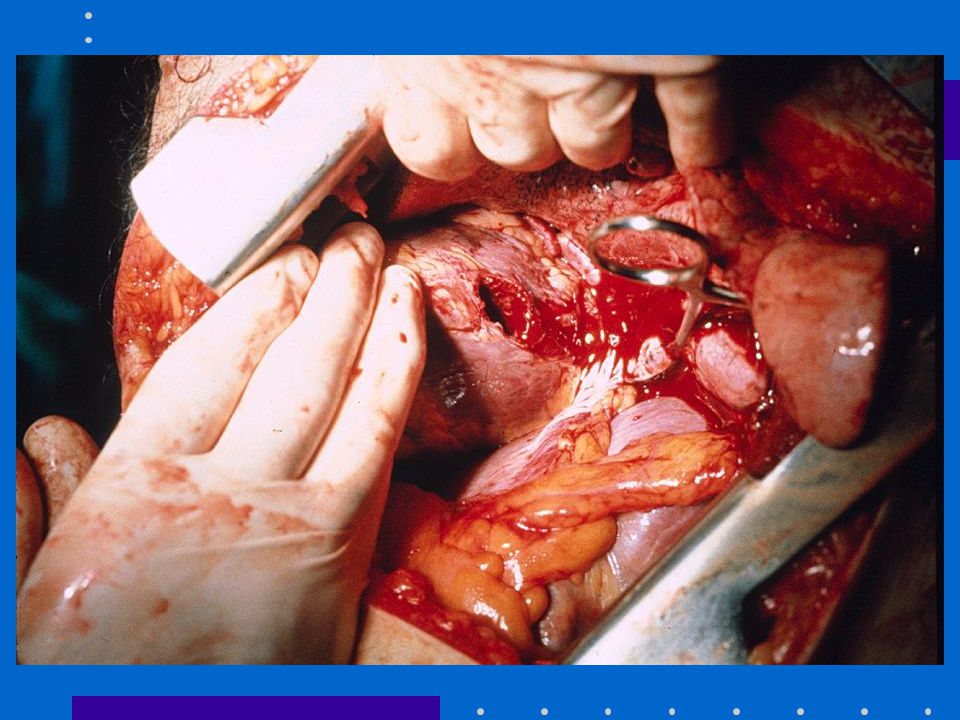
Grade IV splenic laceration, ruptured diaphragm, contrast in stomach

18
Case Management Transferred to OR: –RSI: ketamine, succinylcholine –Chest tube –Fluid + blood resuscitation (type specific uncrossmatched, Level 1 warmer) –Splenectomy, repair of ruptured diaphragm –ICU x 24 hours Full recovery
 –Splenectomy, repair of ruptured diaphragm –ICU x 24 hours Full recovery")
20
Tension Pneumothorax Which is true? 1.Hypoxia, BS, BP, dullness to percussion, + Paw are diagnostic clues 2.N2O is contraindicated 3.ETCO2 is with bilateral tension px 4.Thoracic decompression with a large-bore needle is best done in the 4rth intercostal space, mid-clavicular line

21
Tension Pneumothorax Pathophysiology: –accumulation of air under pressure –compression of contralateral lung, vena cava, cavo-atrial junction Dx: –hypoxia, BS, hyper-resonance, hypotension, tracheal deviation, JVD – Paw (volume controlled ventilation)
")
23
Management Tension Pneumo Large bore needle –2nd IC space, mid-clavicular line –Converts to simple px Chest tube –5th IC space, mid-axillary line Avoid N 2 O + PEEP High index suspicion, especially with PPV

24
Avoid N 2 O

25
Dietrich: Anesthesiology 2001;95:1028 Case: Undiagnosed Traumatic Diaphragmatic Hernia 19 yo parturient, active labor, term, transferred to MHMC, non-reassuring FH trace Anesthesia preop assessment: LUQ pain, dyspnea, tachypnea, tachycardia, BS left, tracheal deviation to right PMH: stab wound left chest 3 yrs prior, no rx required Surgery delayed: trauma/thoracic consult

26
Traumatic Diaphragmatic Rupture Which is true? 1.It is self-limiting + heals spontaneously 2.Stomach and abdominal viscera may herniate, collapse the lung, and risk of aspiration 3.It is more common after blunt than after penetrating thoraco-abdominal trauma 4.It is more common on the right than left side

27
Daiphragmatic hernia in a parturient at term

28
Saggital reconstrcution showing diaphragmatic hernia

29
Dietrich: Anesthesiology 2001;95:128 Management C-section w spinal anesthesia Complicated postop course b/c collapsed lung, pericardial effusion, compression of heart, strangulated + perforated bowel Tx: Pericardial window, antibiotics, prolonged mechanical ventilation, ARDS, repair of bowel + hernia after improved pulmonary fct Discharge to home 4 months post delivery

30
Lim et al: Ann Thorac Surg 2001;71:1714 + 2002;73:342 Case: Penetrating Cardiac Trauma 29 yo male, stab wound to heart RSI ED thoracotomy: 1 inch entry wound in LV Transferred to OR, BP 80/50, HR 130-150

32
Lim et al: Ann Thorac Surg 2001;71:1714 Management Art line Scopolamine, muscle relaxant, PPV Adenosine 12 mg IV bolus (x 3) to HR Transient asystole: allowed accurate placement of sutures; bypass avoided Full recovery
 to HR Transient asystole: allowed accurate placement of sutures; bypass avoided Full recovery")
33
Cardiac Injuries Which is true? 1.Tamponade is best treated by pericardiocentesis in the ED 2.JVD is an important clue for tamponade 3.Echo is reliable method for detecting functional + structural cardiac abnormalities 4.CPB is frequently (>50%) required to repair cardiac injuries
 required to repair cardiac injuries.")
34
Penetrating Cardiac Injuries GSW: usually die Stab: usually present with tamponade Dx: history, JVD, BP, pulsus, echo JVD- may be absent if hypovolemic Tx: surgical drainage + repair, + bypass

35
www.trauma.org/thoracic/index.html Blunt Cardiac Injury (Myocardial Contusion) Spectrum of problems –enzyme abnormalities, ST segment –arrhythmias: PVCs, RBBB, VT –wall motion abnormalities –cardiac failure –cardiac rupture Dx: history, ECG, echo
 Spectrum of problems –enzyme abnormalities, ST segment –arrhythmias: PVCs, RBBB, VT –wall motion abnormalities –cardiac failure –cardiac rupture Dx: history, ECG, echo")
37
Echo

38
Flancbaum L: J Trauma 1986;26:795; Ross P: Arch Surg 1989;124:506 Risk of Surgery with BCI: No Deaths, but...

39
Malangoni et al: Surgery 1994;116:628 Serious BCI @ MHMC Specific injuries –acute myocardial rupture –valve disruption –contusion w CHF or complex arrhythmias –delayed myocardial rupture (44 d) –coronary art thrombosis ECG suggested cardiac injuries in all Echo useful for dx
 –coronary art thrombosis ECG suggested cardiac injuries in all Echo useful for dx")
40
Pitfalls in Cardiothoracic Trauma Failure to appreciate severity of –pulmonary contusion –cardiac injury (blunt + penetrating) –blood loss –other injuries Simple pneumo tension pneumo with PPV Endobronchial intub can mimic tension pneumo Failure to optimize ventilation, oxygenation, organ perfusion, + circulating blood volume
 –blood loss –other injuries Simple pneumo tension pneumo with PPV Endobronchial intub can mimic tension pneumo Failure to optimize ventilation, oxygenation, organ perfusion, + circulating blood volume")
Similar presentations







 advance ET tube B) needle thoracostomy.>")


, FCCP>")













