Download presentation
Presentation is loading. Please wait.

1
Asthma, Rhinitis & Sinusitis A review NYSAFP Winter Weekend & Scientific Assembly
Dr. Sunil Sood Chair, Dept of Pediatrics, Southside Hospital Professor, Pediatrics; Hofstra-North Shore LIJ School of Medicine Dr. Tochi Iroku-Malize Program Director, FM Residency, Southside Hospital Chair, Dept of Family Medicine Hofstra-North Shore LIJ School of Medicine

2
SINUSITIS

6
AAP Clinical Practice Guideline: Management of Sinusitis
Pediatrics 108:798, 2001

7
Background Children have 6 to 8 viral upper respiratory infections each year; 5% to 13% of these may be complicated by a secondary bacterial infection of the paranasal sinuses. Acute bacterial otitis media and acute bacterial sinusitis are the most common indications for the prescription of antibiotics The middle ear cavity connects to the nasopharynx via the eustachian tube. In a sense the middle ear cavity is also a paranasal sinus.

8
Sinus Anatomy by Age ethmoid and maxillary sinuses form in the third to fourth gestational month and, accordingly, are present at birth sphenoid sinuses are generally pneumatized by 5 years of age frontal sinuses appear at age 7 to 8 years but are not completely developed until late adolescence

9
Recommendation 1 The diagnosis of acute bacterial sinusitis is based on clinical criteria in children …… with upper respiratory symptoms that are either persistent or severe Persistent symptoms longer than 10 to 14, but less than 30 days. include nasal or postnasal discharge (of any quality), or daytime cough (which may be worse at night) Severe symptoms temp. at least 102°F (39 C) purulent nasal discharge present concurrently for at least 3 to 4 consecutive days in a child who seems ill
, or daytime cough (which may be worse at night) Severe symptoms. temp. at least 102°F (39 C) purulent nasal discharge present concurrently for at least 3 to 4 consecutive days. in a child who seems ill.")
10
Clinical tips (children)
Unreliable/infrequent: Facial pain, tenderness Transillumination Very likely (ethmoid) Periorbital swelling
 Periorbital swelling.")
11
Recommendation 2a Imaging studies are not necessary to confirm a diagnosis of clinical sinusitis in children <=6 years “For children 6 years of age or younger, the history predicted abnormal sinus radiographs in 88% of children” Therefore… (and because history plus abnormal radiographs results in a positive sinus aspirate in 75% of cases), radiographs can be safely omitted”
, radiographs can be safely omitted")
12
Recommendation 2a continued The need for radiographs as a confirmatory test of acute sinusitis in children older than 6 years with persistent symptoms and for all children (regardless of age) with severe symptoms is controversial. “Some practitioners may elect to perform sinus radiographs with the expectation or suspicion that the study may be normal. A normal radiograph is powerful evidence that bacterial sinusitis is not the cause of the clinical syndrome.”

13
Recommendation 2b CT scans of the paranasal sinuses should be reserved for patients in whom surgery is being considered as a management strategy Also valuable in children with FUO, recurrent febrile illnesses, chronic fatigue, unexplained headaches, to rule out sinusitis and avoid unnecessary antibiotics.

14
Recommendation 3 Antibiotics are recommended to achieve a more rapid clinical cure
“To promote the judicious use of antibiotics, it is essential that children diagnosed as having acute bacterial sinusitis meet the defining clinical presentations of "persistent" or "severe" disease. This will minimize the number of children with uncomplicated viral upper respiratory tract infections who are treated with antimicrobials.”

15
ACUTE UNCOMPLICATED SINUSITIS Pathogens

16
Recommendation 3 AMOXICILLIN STILL DRUG OF CHOICE
In the absence of any risk factors* for penicillin resistant Strep. pneumoniae, approximately 80% will respond to conventional dose * day care, recent (<90 days) antibiotics, age less than 2 years Duration 10 days or 7 days after symptom free
 antibiotics, age less than 2 years. Duration 10 days or 7 days after symptom free.")
17
Recommendation 3 continued SECOND-LINE THERAPY
If do not improve in h high-dose amoxicillin-clavulanate (80-90 mg/kg/d of amoxicillin component, with 6.4 mg/kg/d of clavulanate in 2 divided doses) cefdinir, cefuroxime, or cefpodoxime or a single dose of ceftriaxone (50 mg/kg/d) followed by PO antibiotic
 cefdinir, cefuroxime, or cefpodoxime or a single dose of ceftriaxone (50 mg/kg/d) followed by PO antibiotic.")
18
Recommendation 4 Children with complications or suspected complications of acute bacterial sinusitis should be treated promptly and aggressively. This should include consultation with ENT / ID / ophthalmology/ neurosurgery Mild periorbital cellulitis (eyelid <50% closed) -- treat with oral antibiotic as an outpatient with daily encounters
 -- treat with oral antibiotic as an outpatient with daily encounters.")
19
Recommendation 4 continued
If not improved in hours or if progressing rapidly, proptosis, impaired visual acuity, or impaired extraocular mobility, CT scan (preferably coronal thin cut with contrast) of the orbits/sinuses is essential to exclude a suppurative complication IV antibiotics in hospital
 of the orbits/sinuses is essential to exclude a suppurative complication. IV antibiotics in hospital.")
21
RHINITIS

22
Team Based Learning… Let’s Start!!! Split into teams
Solve the questions Battle of the teams Let’s Start!!!

23
#1 Rhinitis affects between 10 and 30 % of adults and 40 % of children in the US. Nasal symptoms: congestion, rhinorrhea (anterior and posterior), sneezing, & itching. Can cause: fatigue, headache, cognitive impairment, and sleep disturbance;
, sneezing, & itching. Can cause: fatigue, headache, cognitive impairment, and sleep disturbance;")
24
#2 Differentiating allergic rhinitis from other causes of rhinitis can be difficult because the diagnostic criteria for various forms of rhinitis are not always clear-cut. Accurate diagnosis is important because therapies that are effective for allergic rhinitis (i.e., antihistamines and nasal corticosteroids) may be less effective for other types of rhinitis
 may be less effective for other types of rhinitis.")
25
Allergic rhinitis Nonallergic rhinitis
Episodic rhinitis Occupational rhinitis (allergen) Perennial rhinitis Seasonal rhinitis Atrophic rhinitis Chemical- or irritant-induced rhinitis Drug-induced rhinitis Emotional rhinitis Exercise-induced rhinitis Gustatory rhinitis Hormone-induced rhinitis Infectious rhinitis Nonallergic rhinitis with eosinophilia syndrome Occupational rhinitis (irritant) Perennial nonallergic rhinitis Postural reflexes Primary ciliary dyskinesia Reflux-induced rhinitis or gastroesophageal reflux disease
 Perennial rhinitis. Seasonal rhinitis. Atrophic rhinitis. Chemical- or irritant-induced rhinitis. Drug-induced rhinitis. Emotional rhinitis. Exercise-induced rhinitis. Gustatory rhinitis. Hormone-induced rhinitis. Infectious rhinitis. Nonallergic rhinitis with eosinophilia syndrome. Occupational rhinitis (irritant) Perennial nonallergic rhinitis. Postural reflexes Primary ciliary dyskinesia. Reflux-induced rhinitis or gastroesophageal reflux disease.")
26
Conditions that may mimic symptoms of rhinitis
Cerebrospinal fluid rhinorrhea Inflammatory or immunologic conditions Midline granuloma Nasal polyposis Sarcoidosis Sjögren’s syndrome Systemic lupus erythematosus Wegener’s granulomatosis Relapsing polychondritis Structural or mechanical conditions Choanal atresia Deviated septum Enlarged adenoids Foreign bodies Hypertrophic turbinates Nasal tumors

27
Since 1998, three expert panels have published reviews of rhinitis.
The first report American Academy of Allergy, Asthma, and Immunology (AAAAI) as a complete guideline for the diagnosis and management of rhinitis. The second report, World Health Organization (WHO) 2001, Focuses on allergic rhinitis and asthma Includes differential diagnosis of rhinitis, proposed a new classification for allergic rhinitis, seasonal and perennial were not satisfactory. suggested a classification system based on the symptoms of intermittent, persistent, mild, and moderate-severe rhinitis. The third report, Agency for Healthcare Research and Quality (AHRQ) with the American Academy of Family Physicians and the AAAAI. not a clinical guideline but an evaluation of the evidence on rhinitis. The report did not identify any studies differentiating allergic rhinitis and nonallergic rhinitis based on clinical symptoms, physical examination findings, or associated
 as a complete guideline for the diagnosis and management of rhinitis. The second report, World Health Organization (WHO) 2001, Focuses on allergic rhinitis and asthma. Includes differential diagnosis of rhinitis, proposed a new classification for allergic rhinitis, seasonal and perennial were not satisfactory. suggested a classification system based on the symptoms of intermittent, persistent, mild, and moderate-severe rhinitis. The third report, Agency for Healthcare Research and Quality (AHRQ) with the American Academy of Family Physicians and the AAAAI. not a clinical guideline but an evaluation of the evidence on rhinitis. The report did not identify any studies differentiating allergic rhinitis and nonallergic rhinitis based on clinical symptoms, physical examination findings, or associated.")
28
#3 Differentiate via a thorough and comprehensive history
symptoms (i.e., duration, exposures, magnitude of reaction, patterns, and chronicity); triggers; seasonal variation; environmental influences; allergies; medical history (i.e., trauma, family, and treatment histories); and current treatments
; triggers; seasonal variation; environmental influences; allergies; medical history (i.e., trauma, family, and treatment histories); and current treatments.")
29
#4 Physical Examination Findings That Suggest Rhinitis
General Constitutional symptoms suggest allergic rhinitis. Mouth versus nose breathing is a symptom of chronic congestion. Eyes Allergic shiners (i.e., dark areas under the eyes) Conjunctivitis Ears Air fluid levels can suggest chronic congestion. Nose A deviated or perforated septum and polyps are structural causes of rhinitis. Purulent or bloody discharge can be a sign of sinusitis. Fiberoptic visualization can detect structural causes of rhinitis. Adapted from Dykewicz MS, Fineman S, Skoner DP, Nicklas R, Lee R, Blessing-Moore J, et al. Diagnosis and management of rhinitis: complete guidelines of the Joint Task Force on Practice Parameters in Allergy, Asthma and Immunology. American Academy of Allergy, Asthma, and Immunology. Ann Allergy Asthma Immunol 1998;81(pt 2):492. Mouth Enlarged tonsils and pharyngeal postnasal discharge are associated with nonallergic rhinitis. Neck Lymphadenopathy suggests an infectious cause of rhinitis. Chest Allergic or atopic disease (e.g., asthma) supports the diagnosis of allergic rhinitis. Skin Allergic or atopic disease (e.g., eczema)
 Conjunctivitis. Ears. Air fluid levels can suggest chronic congestion. Nose. A deviated or perforated septum and polyps. are structural causes of rhinitis. Purulent or bloody discharge can be a sign. of sinusitis. Fiberoptic visualization can detect structural. causes of rhinitis. Adapted from Dykewicz MS, Fineman S, Skoner DP, Nicklas R, Lee R, Blessing-Moore J, et al. Diagnosis and management of rhinitis: complete guidelines of the Joint Task Force on Practice Parameters in Allergy, Asthma and Immunology. American Academy of Allergy, Asthma, and Immunology. Ann Allergy Asthma Immunol 1998;81(pt 2):492. Mouth. Enlarged tonsils and pharyngeal postnasal. discharge are associated with nonallergic. rhinitis. Neck. Lymphadenopathy suggests an infectious. cause of rhinitis. Chest. Allergic or atopic disease (e.g., asthma) supports the diagnosis of allergic rhinitis. Skin. Allergic or atopic disease (e.g., eczema)")
30
#5 Allergy Testing None of the three reports1-3 on rhinitis provides specific recommendations on when to perform allergy testing for patients with rhinitis. Diagnostic Testing The most common diagnostic tests for allergic rhinitis are the percutaneous skin test and the allergen-specific immunoglobulin E (IgE) antibody test.
 antibody test.")
33
#6 Allergic Rhinitis Episodic Occupational Perennial Seasonal

34
#7 Non Allergic Rhinitis
Atrophic Chemical or irritant Durg Emotional Exercise Gustatory Hormone Infectious Nonallergic with eosinophilia Irritant occupational Perennial nonallergic Postural reflex Primary ciliary dyskinesia GERD

35
#8 Environmental Control Measures
Pollens, fungi, dust mites, furry animals, and insect emanations are the most common triggers of allergic rhinitis. avoid going outdoors during periods of high pollen counts. reduce their fungi exposure by removing sources of moisture, replacing contaminated materials, and cleaning nonporous surfaces with a diluted bleach solution. control the humidity in their home, cover bedding with dust mite covers, clean floors with a high-efficiency particulate air vacuum, and use acaricides. Avoiding all contact with animals

36
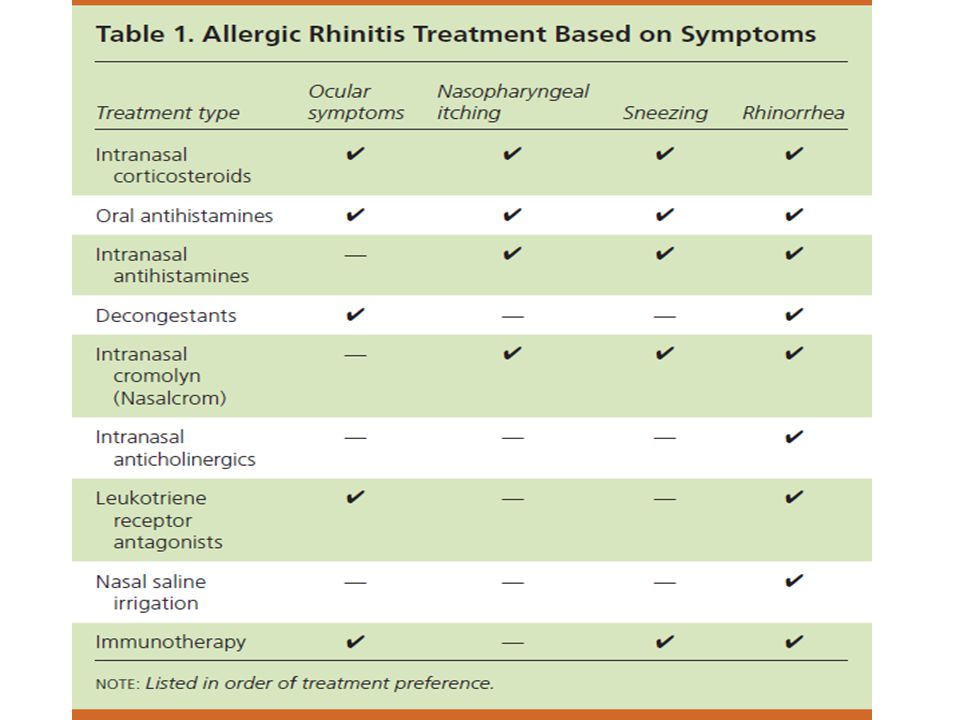
#9 Treatment

39
#10 Rhinitis and Asthma Occupational asthma merits special consideration in all cases of new adult asthma or recurrence of childhood asthma after a significant asymptomatic period (SOR C). Occupational asthma is often preceded by the development of rhinitis in the workplace and should be considered in patients whose symptoms improve away from work. Ref: Nicholson PJ, Cullinan P, Newman Taylor AJ, et al: Evidence based guidelines for the prevention, identification, and management of occupational asthma. Occup Environ Med 2005;62(5); ) Taiwo OA, Cantley L, Mobo BP Jr: Recognizing occupational illnesses and injuries. Am Fam Physician (2):
. Occupational asthma is often preceded by the development of rhinitis in the workplace and should be considered in patients whose symptoms improve away from work. Ref: Nicholson PJ, Cullinan P, Newman Taylor AJ, et al: Evidence based guidelines for the prevention, identification, and management of occupational asthma. Occup Environ Med 2005;62(5); ) Taiwo OA, Cantley L, Mobo BP Jr: Recognizing occupational illnesses and injuries. Am Fam Physician (2):")
40
ASTHMA

41
Class Work Multiple choice questions Discussion of Answers

42
When prescribing an inhaled corticosteroid for control of asthma, the risk of oral candidiasis can be decreased by A) using a valved holding chamber B) limiting use of the inhaled corticosteroid to once daily C) adding nasal fluticasone propionate (Flonase) D) adding montelukast (Singulair) E) adding salmeterol (Serevent)
 using a valved holding chamber B) limiting use of the inhaled corticosteroid to once daily C) adding nasal fluticasone propionate (Flonase) D) adding montelukast (Singulair) E) adding salmeterol (Serevent)")
43
You have just diagnosed mild persistent asthma in a 13-year-old African-American female. Along with patient education, your initial medical management should be A) a short-acting inhaled beta-agonist to be used only as needed B) a long-acting inhaled beta-agonist daily C) a low-dose inhaled corticosteroid daily, along with a short-acting inhaled beta-agonist as needed D) a low-dose inhaled corticosteroid daily, along with a long-acting inhaled beta-agonist daily E) montelukast (Singulair) daily
 a short-acting inhaled beta-agonist to be used only as needed B) a long-acting inhaled beta-agonist daily C) a low-dose inhaled corticosteroid daily, along with a short-acting inhaled beta-agonist as needed D) a low-dose inhaled corticosteroid daily, along with a long-acting inhaled beta-agonist daily E) montelukast (Singulair) daily .")
44
Because of safety concerns, which one of the following asthma medications should be used only as additive therapy and not as monotherapy? A) Inhaled corticosteroids B) Leukotriene-receptor antagonists C) beta-agonists D) Long-acting beta-agonists E) Mast cell stabilizers
 Inhaled corticosteroids. B) Leukotriene-receptor antagonists. C) beta-agonists. D) Long-acting beta-agonists. E) Mast cell stabilizers.")
45
A 7-year-old female with a history of asthma is brought to your office for a routine follow-up visit. She has a history of exercise-induced asthma, but also has had exacerbations in the past that were unrelated to exercise. In the past month, she has premedicated herself with albuterol (Proventil, Ventolin) with a spacer before recess 5 days/week as usual. She has also needed her albuterol to treat symptoms (wheezing and/or shortness of breath) once or twice per week and had one exacerbation requiring medical treatment in the past year. She has had no nighttime symptoms. Albuterol as needed is her only medication. After reinforcing asthma education, which one of the following would be most appropriate? A) Referral to an asthma specialist B) Addition of a low-dose inhaled corticosteroid C) Addition of a long-acting beta-agonist D) Elimination of premedication with albuterol, restricting use to an as-needed basis E) No changes to her regimen
 Referral to an asthma specialist. B) Addition of a low-dose inhaled corticosteroid. C) Addition of a long-acting beta-agonist. D) Elimination of premedication with albuterol, restricting use to an as-needed basis. E) No changes to her regimen.")
46
Which one of the following is true concerning the use of short-acting inhaled beta-agonists for asthma? A) They should be given before any inhaled corticosteroid to facilitate lung delivery B) They are ineffective in patients taking beta-blockers C) They are less effective than oral beta-agonists D) They are less effective than anticholinergic bronchodilators when given with inhaled corticosteroids E) Their effects begin within 5 minutes and last 4–6 hours
 They should be given before any inhaled corticosteroid to facilitate lung delivery. B) They are ineffective in patients taking beta-blockers. C) They are less effective than oral beta-agonists. D) They are less effective than anticholinergic bronchodilators when given with inhaled corticosteroids. E) Their effects begin within 5 minutes and last 4–6 hours.")
47
When treating acute adult asthma in the emergency department, using a metered-dose inhaler (MDI) with a spacer has been shown to result in which one of the following, compared to use of a nebulizer? A) Higher hospitalization rates B) Shorter stays in the emergency department C) Higher relapse rates D) Less improvement in peak-flow rates E) Increases in the total dose of albuterol
 Higher hospitalization rates. B) Shorter stays in the emergency department. C) Higher relapse rates. D) Less improvement in peak-flow rates. E) Increases in the total dose of albuterol.")
48
You see a 9-year-old female for evaluation of her asthma
You see a 9-year-old female for evaluation of her asthma. She and her mother report that she has shortness of breath and wheezing 3–4 times per week, which improves with use of her albuterol inhaler. She does not awaken at night due to symptoms, and as long as she has her albuterol inhaler with her she does not feel her activities are limited by her symptoms. About once per year she requires prednisone for an exacerbation, often triggered by a viral infection. Based on this information you classify her asthma severity as A) intermittent B) mild persistent C) moderate persistent D) severe persistent
 intermittent. B) mild persistent. C) moderate persistent. D) severe persistent.")
49
A 14-year-old female with a history of asthma is having daytime symptoms about once a week and symptoms that awaken her at night about once a month. Her asthma does not interfere with normal activity, and her FEV is >80% of predicted. Which one of the following is the most appropriate treatment plan for this patient? A) A short-acting inhaled beta-agonist as needed B) Low-dose inhaled corticosteroids daily C) A leukotriene receptor antagonist daily D) Medium-dose inhaled corticosteroids daily E) Low-dose inhaled corticosteroids plus a long-acting inhaled beta-agonist daily
 A short-acting inhaled beta-agonist as needed. B) Low-dose inhaled corticosteroids daily. C) A leukotriene receptor antagonist daily. D) Medium-dose inhaled corticosteroids daily. E) Low-dose inhaled corticosteroids plus a long-acting inhaled beta-agonist daily.")
50
Overview of Changes to Asthma Guidelines

57
Thank You Any Questions?

Similar presentations














>")












>")




