Download presentation
Presentation is loading. Please wait.

1
OHSU Updates in Hematology and Breast Cancer Conference CML ASH Update Michael J. Mauro, MD

2
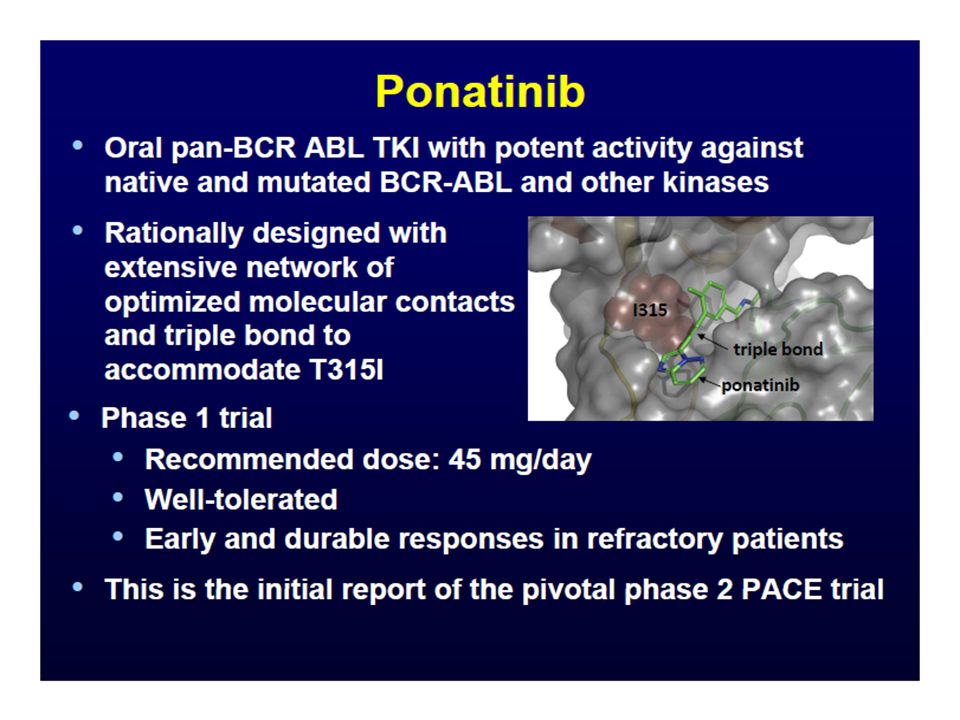
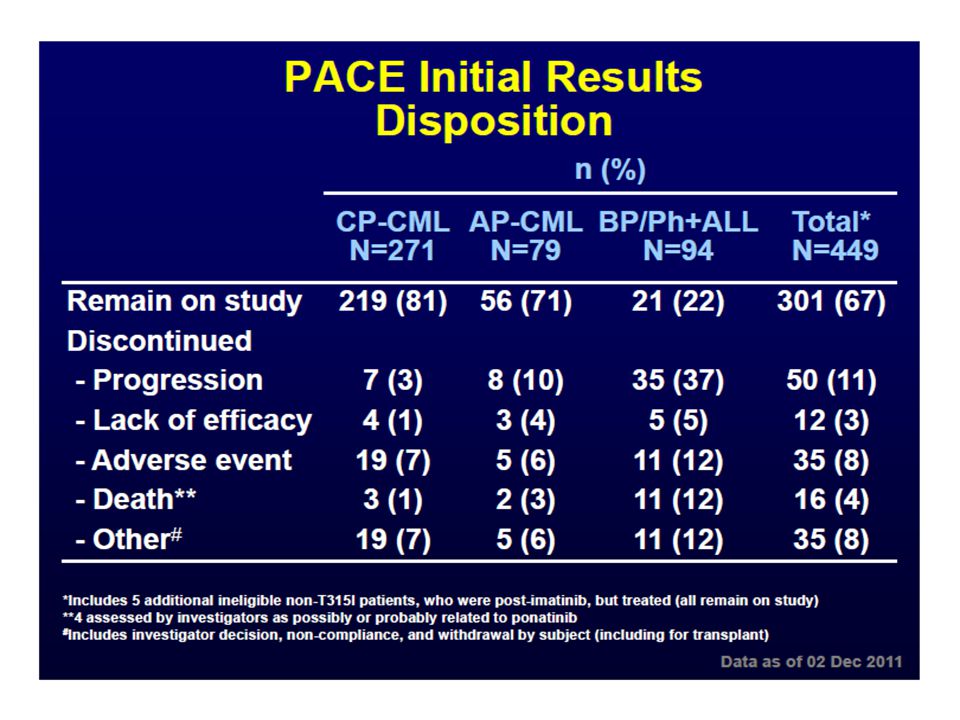
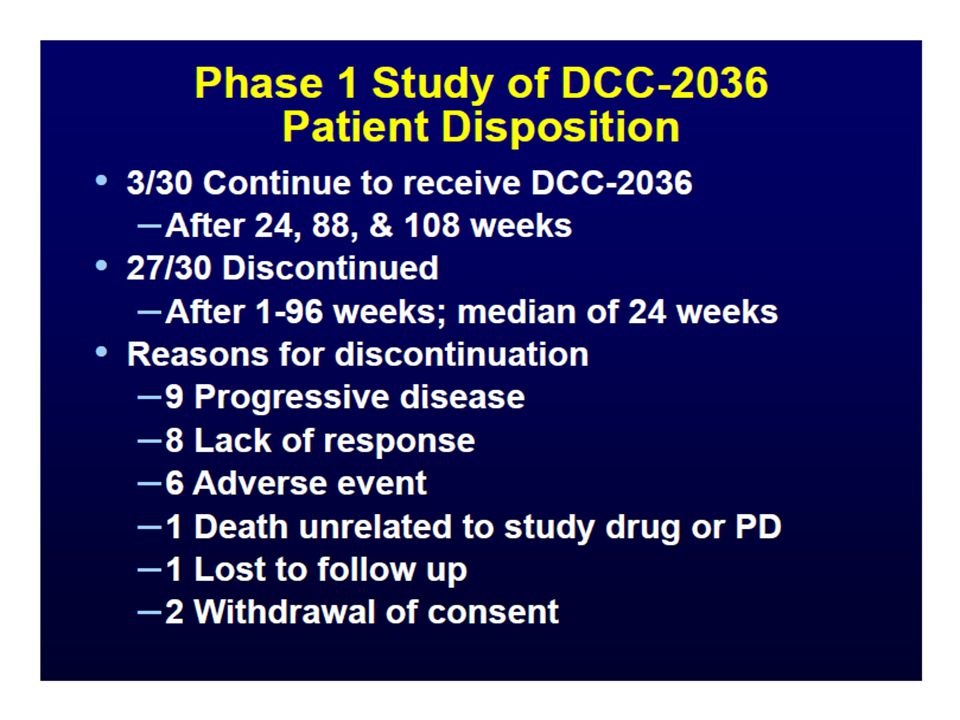
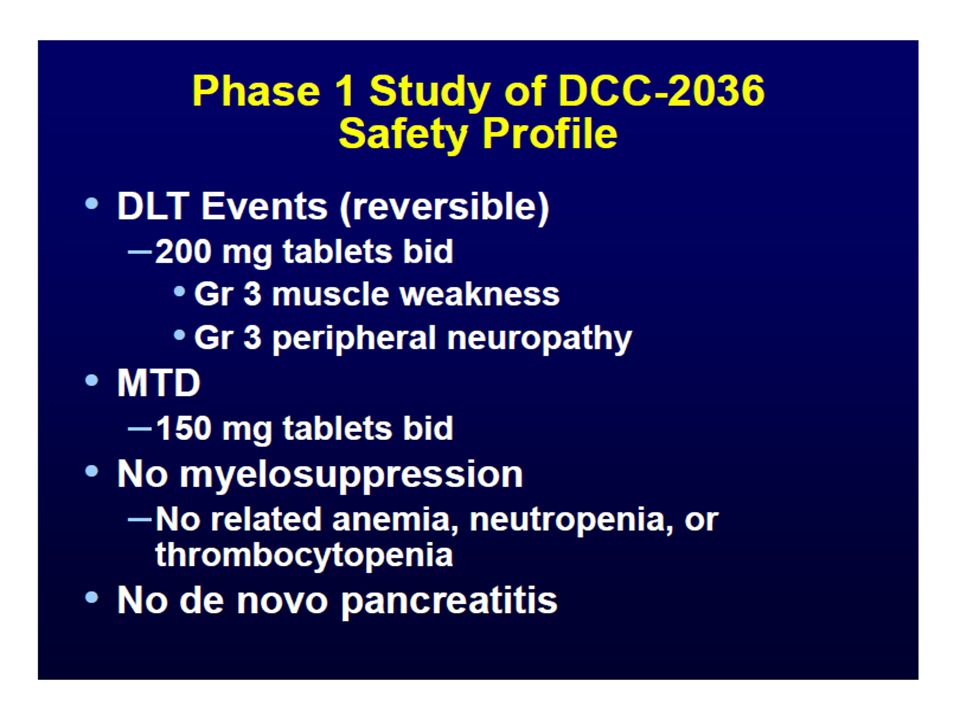
CML Abstracts Novel Agents Abstract # 109 : A Pivotal Phase 2 Study of Ponatinib in Patients with CML and Ph+ ALL Resistant or Intolerant to Dasatinib or Nilotinib or with the T315I Mutation Abstract # 601: A Phase 1 Study of DCC-2036, a Novel Oral Inhibitor of BCR-ABL1 Kinase, in Patients with Ph+ Leukemia, including Patients withT315I Mutation Path to Cure Abstract # 604: Discontinuation of Dasatinib or Nilotinib in Chronic Myeloid Leukemia Patients with Stable Undetectable BCR-ABL Transcripts: Results from the French CML Group Response Prediction Abstract # 112: Validation of the New ELN Recommendations for BCR-ABL KD Mutation Analysis in CML: an Analysis of the CML GIMEMA WP Studies Abstract # 783: Molecular and Cytogenetic Response at 3 Months of Imatinib Predicts Progression-free Survival (PFS) and Overall Survival (OS) – a Follow-Up Analysis of the Randomized CML-Study IV Longer-Term Follow-Up Abstract # 452: Nilotinib versus Imatinib in Patients with Newly Diagnosed Philadelphia Chromosome- Positive (Ph+) Chronic Myeloid Leukemia in Chronic Phase (CML-CP): ENESTnd 3-Year Follow-Up Abstract # 455 : Bosutinib versus Imatinib in Newly Diagnosed Chronic Phase Chronic Myeloid Leukemia-- BELA Trial: 24-Month Follow-up
 and Overall Survival (OS) – a Follow-Up Analysis of the Randomized CML-Study IV Longer-Term Follow-Up Abstract # 452: Nilotinib versus Imatinib in Patients with Newly Diagnosed Philadelphia Chromosome- Positive (Ph+) Chronic Myeloid Leukemia in Chronic Phase (CML-CP): ENESTnd 3-Year Follow-Up Abstract # 455 : Bosutinib versus Imatinib in Newly Diagnosed Chronic Phase Chronic Myeloid Leukemia-- BELA Trial: 24-Month Follow-up")
3
Abstract #109

11
Abstract #601

17
DISCONTINUATION OF DASATINIB OR NILOTINIB IN CHRONIC MYELOID LEUKEMIA PATIENTS WITH STABLE UNDETECTABLE BCR-ABL TRANSCRIPTS: Results from the French CML group (FI-LMC) Delphine Rea*, Philippe Rousselot, Franck Nicolini, Laurence Legros, Michel Tulliez, Stéphane Giraudier, Pascale Cony-Makhoul, François Guilhot, François-Xavier Mahon Selected by the ASH Program Session Name: 632. Chronic Myeloid Leukemia - Therapy: New Drugs, New Procedures Session Date: Monday, December 12, 2011 Session Time: 2:45 PM - 4:15 PM Presentation Time: 3:30 PM Room: San Diego Convention Center, Ballroom 20BC Abstract #604

18
DESIGN AND ENDPOINTS Primary endpoint: stable MMR by 6 months Main secondary endpoints: –Stable MMR by 12, 18 and 24 months –Risk of progression to AP/BP –Undetectable BCR-ABL by 12 months upon reintroduction of treatment M6M12M18M24D1 STOP 2G-TKI Monthly RQ-PCR every 2-3 months Undetectable BCR-ABL ≥ 24 months

19
TRIAL DETAILS: ELIGIBILITY Age ≥ 18 years CP- or AP-CML at diagnosis M-BCR transcripts Ongoing dasatinib or nilotinib treatment No prior progression to AP/BC while on therapy Treatment with TKI for at least 36 months Undetectable BCR-ABL* for at least 24 months MONITORING AND TREATMENT RESUMPTION POLICY Blood counts and RQ-PCR monthly during the first 12 months, and every 2-3 months thereafter Bone marrow smears, cytogenetic and mutational analysis recommended in case of a rise in BCR-ABL above 1% IS 2G-TKI reintroduction triggered by the loss of MMR (BCR- ABL/ABL ratio > 0.1% IS) * Undetectable BCR-ABL at local laboratories with at least 20 000x2 copies of the ABL1 control gene
 * Undetectable BCR-ABL at local laboratories with at least x2 copies of the ABL1 control gene")
20
TREATMENT HISTORY Imatinib n=31 12/31: post IFN 19/31: frontline Nilotinib n=2 2/2 frontline Dasatinib n=19 Nilotinib n=12 Dasatinib n=1 Nilotinib n=2 Switch n=31 23/31: intolerance 8/31: resistance/suboptimal response Switch n=3 2/3: intolerance 1/3: resistance/suboptimal response Dasatinib n=17 Nilotinib n=11 No switch n=28 STOP 2G-TKI

21
STABLE MMR BY 6 MONTHS Following 2G-TKI cessation, 8 pts lost MMR after a median time off-therapy of 2 months (2-5) 6 month: 72.8% (95% CI: 55.4-90.1) Kaplan-Meier estimate of stable MMR after 2G-TKI cessation 0 20 40 60 80 100 0612182430 Months since 2G-TKI cessation Survival without loss of MMR %
 6 month: 72.8% (95% CI: ) Kaplan-Meier estimate of stable MMR after 2G-TKI cessation Months since 2G-TKI cessation Survival without loss of MMR %")
22
PATTERNS OF BCR-ABL IN PATIENTS REMAINING OFF-THERAPY 25/33 pts are currently off-therapy (median 6, range: 0-25) 15/25 pts have a follow-up of at least 6 months (median 13, range: 6-25) 3 different patterns of molecular residual disease: Sustained undetectable BCR-ABL n=3 Persistently detectable BCR-ABL n=1 Occasionally detectable BCR-ABL Below the MMR threshold n=11
 15/25 pts have a follow-up of at least 6 months (median 13, range: 6-25) 3 different patterns of molecular residual disease: Sustained undetectable BCR-ABL n=3 Persistently detectable BCR-ABL n=1 Occasionally detectable BCR-ABL Below the MMR threshold n=11")
23
Abstract #112

25
Factor AnalyzedNN positive for KD mutation (%) De novo CP CML 581 (2%) De novo AP/BC CML 122 (17%) IM Failure (ELN criteria) 16645 (27%) Suboptimal IM Response (ELN) 23311 (5%) Rise in PCR without loss of MMR 700 (0%) Rise in PCR with loss of MMR 894 (5%) NIL/DAS ‘Failure’ (ELN criteria) 1911 (58%) NIL/DAS ‘Suboptimal’ (ELN criteria) 194 (21%)
 De novo CP CML 581 (2%) De novo AP/BC CML 122 (17%) IM Failure (ELN criteria) (27%) Suboptimal IM Response (ELN) (5%) Rise in PCR without loss of MMR 700 (0%) Rise in PCR with loss of MMR 894 (5%) NIL/DAS ‘Failure’ (ELN criteria) 1911 (58%) NIL/DAS ‘Suboptimal’ (ELN criteria) 194 (21%)")
27
Molecular and Cytogenetic Response at 3 Months of Imatinib Predicts Progression-free Survival (PFS) and Overall Survival (OS) – a Follow-Up Analysis of the Randomized CML-Study IV Abstract #783 Benjamin Hanfstein, MD, Martin C. Müller, MD, Philipp Erben, MD, Michael Lauseker, Susanne Saussele, MD, Ulrike Proetel, MD, Susanne Schnittger, PhD, Claudia Haferlach, MD, Hans-Jochem Kolb, MD, Stefan W. Krause, MD, Christoph Nerl, MD, Dominik Heim, MD, Gabriela M. Baerlocher, MD, Jörg E. A. Schubert, MD, Hermann Einsele, MD, Mathias Hänel, MD, Jolanta Dengler, MD, Christiane Falge, MD, Lothar Kanz, MD, Andreas Neubauer, MD, Michael Kneba, MD, Frank Stegelmann, MD, Michael Pfreundschuh, MD, Cornelius F. Waller, MD, Markus Pfirrmann, PhD, Jörg Hasford, MD, Wolf-Karsten Hofmann, MD, Rüdiger Hehlmann, MD, Andreas Hochhaus, MD, for The SAKK and for The German CML Study Group

28
N = 1,223 (assigned by April 30, 2010) Median age 52 years (16-85), 39% female Median observation time 4.8 years Treatment: Imatinib 400 mg/d n = 335 (27%) Imatinib 400 mg/d + Interferon alphan = 366 (30%) Imatinib + Cytarabinen = 149 (12%) Imatinib 800 mg/dn = 373 (30%) Patients and samples
 Median age 52 years (16-85), 39% female Median observation time 4.8 years Treatment: Imatinib 400 mg/d n = 335 (27%) Imatinib 400 mg/d + Interferon alphan = 366 (30%) Imatinib + Cytarabinen = 149 (12%) Imatinib 800 mg/dn = 373 (30%) Patients and samples")
29
Progression-free Survival (PFS) BCR-ABL IS at 3 months ≤10% vs. >10% >10% ≤10% BCR-ABL IS n 5Y-PFS ≤10% 49993% >10% 18987% 0.003 p-value

30
Overall Survival (OS) BCR-ABL IS at 3 months ≤10% vs. >10%
 BCR-ABL IS at 3 months ≤10% vs. >10%")
31
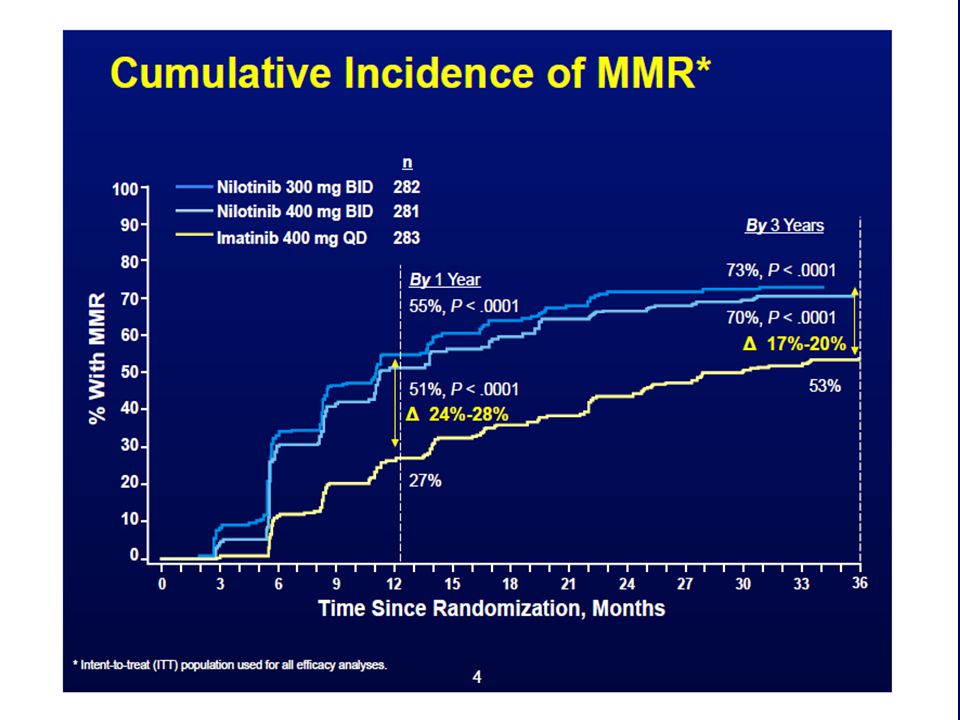
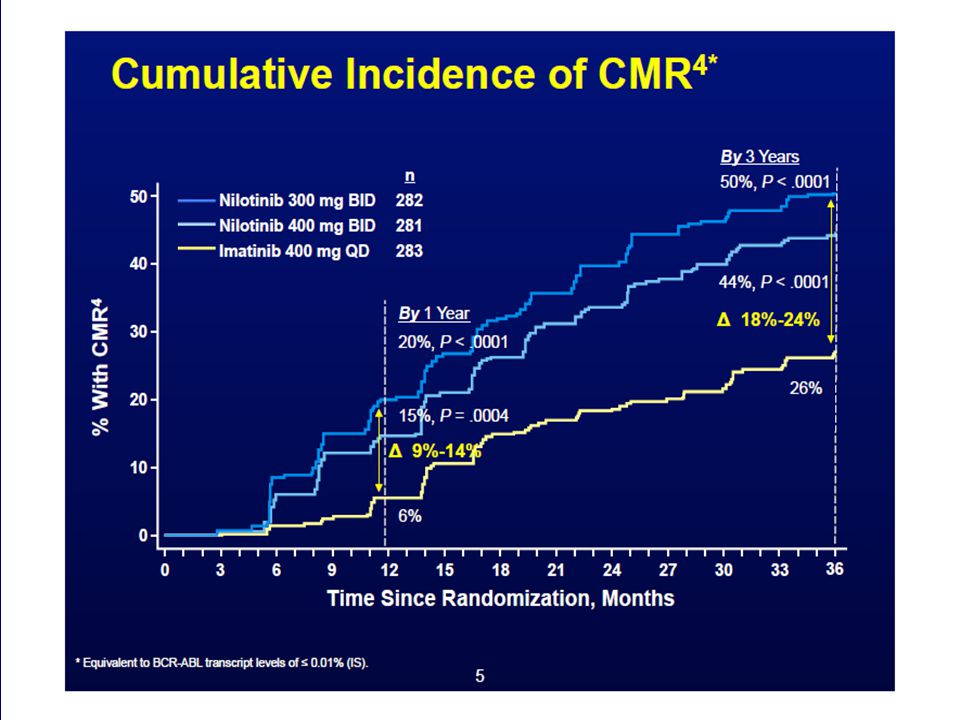
Abstract #452

36
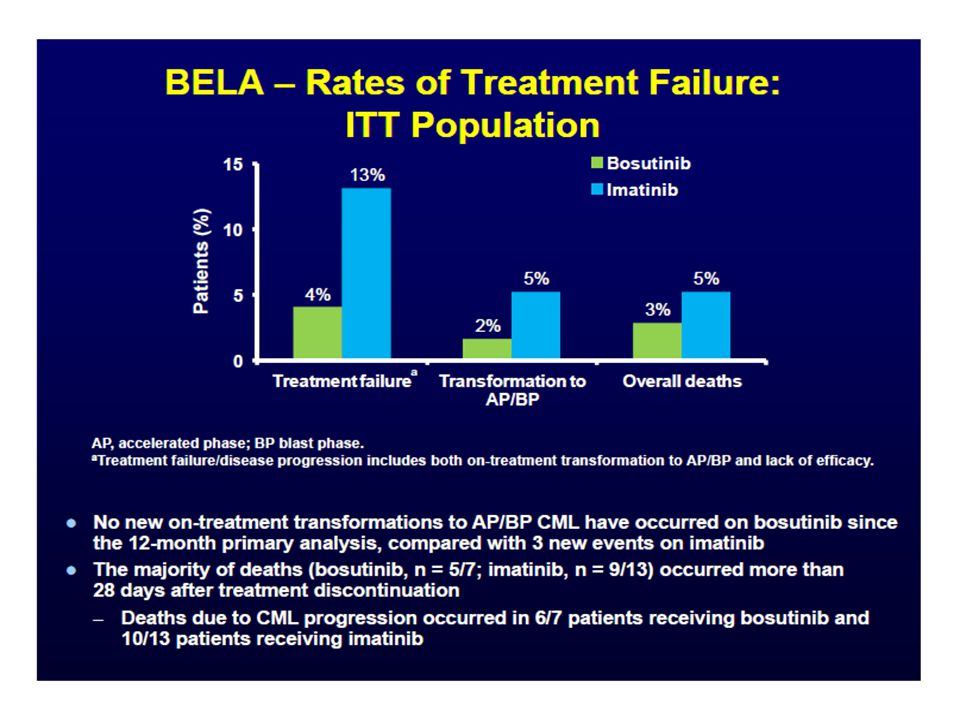
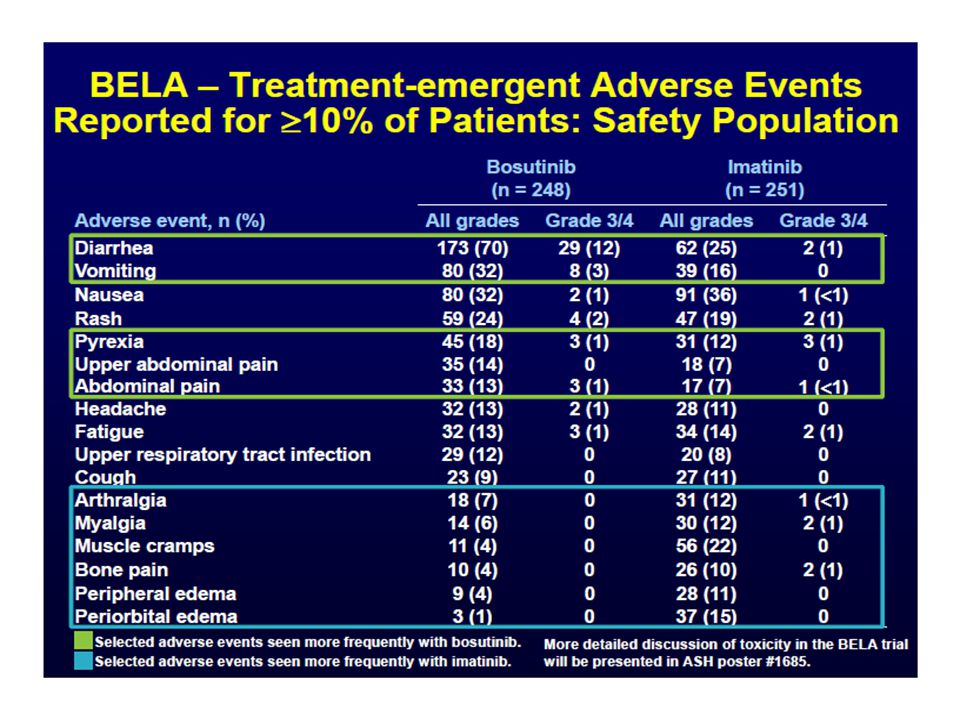
Abstract #455

44
CML ASH Highlights: Summary (I) Ponatinib, a 3 rd generation Abl kinase inhibitor, has remarkable activity in high-level resistant Ph+ leukemia confirmed in phase II data, particularly T315I mutation bearing and multidrug resistant chronic phase CML DCC-2036, an oral ABL switch pocket inhibitor, shows good tolerability and activity in high-level resistant Ph+ leukemia and a novel mechanism Discontinuation of therapy in patients on second-generation (nilotinib / dasatinib) Abl kinase inhibitors after imatinib shows similar pattern of early relapse but may lead to a higher fraction of stable, intermittent trace MRD+ patients sustained off therapy; longer follow-up is needed
 Ponatinib, a 3 rd generation Abl kinase inhibitor, has remarkable activity in high-level resistant Ph+ leukemia confirmed in phase II data, particularly T315I mutation bearing and multidrug resistant chronic phase CML DCC-2036, an oral ABL switch pocket inhibitor, shows good tolerability and activity in high-level resistant Ph+ leukemia and a novel mechanism Discontinuation of therapy in patients on second-generation (nilotinib / dasatinib) Abl kinase inhibitors after imatinib shows similar pattern of early relapse but may lead to a higher fraction of stable, intermittent trace MRD+ patients sustained off therapy; longer follow-up is needed")
45
CML ASH Highlights: Summary (II) Timing and utility of Abl kinase mutation testing is clarified and incudes initial AP/BC disease, suboptimal and failure responses, and molecular relapse that leads to loss of MMR Multiple reports, including the large German CML IV study, point towards 3mo molecular response- 10% Bcr-Abl levels- as predictive for outcome Nilotinib as primary therapy for CP CML shows superior cytogenetic and molecular response and protection from progression in longer follow-up (3y) Bosutinib, although challenged by early GI toxicity, shows improvement in molecular response and cumulative cytogenetic response over imatinib at 2y
 Timing and utility of Abl kinase mutation testing is clarified and incudes initial AP/BC disease, suboptimal and failure responses, and molecular relapse that leads to loss of MMR Multiple reports, including the large German CML IV study, point towards 3mo molecular response- 10% Bcr-Abl levels- as predictive for outcome Nilotinib as primary therapy for CP CML shows superior cytogenetic and molecular response and protection from progression in longer follow-up (3y) Bosutinib, although challenged by early GI toxicity, shows improvement in molecular response and cumulative cytogenetic response over imatinib at 2y")
46
OHSU clinical trials in CML/MPN Imatinib/other TKI resistant: Nilotinib + LDE (smoothend inhibitor) Imatinib/other TKI resistant: Observational registry (OHSU) Newly diagnosed CML: Nilotinib FL->elimination of MRD strategy/discontinuation Newly diagnosed CML: Observational registry (SIMPLICITY) CMML: 5-Azacitadine MF with thrombocytopenia: ruxolitinib All patients: sequenome/other diagnostic research studies 46
 Imatinib/other TKI resistant: Observational registry (OHSU) Newly diagnosed CML: Nilotinib FL->elimination of MRD strategy/discontinuation Newly diagnosed CML: Observational registry (SIMPLICITY) CMML: 5-Azacitadine MF with thrombocytopenia: ruxolitinib All patients: sequenome/other diagnostic research studies 46")
47
Thank you for your attention! Thank you to all the research and clinical staff Thank you to RNs Linda Chalmers and Bashi Ratterree Please do not hesitate to call for questions, clinical trial availability, collaboration, diagnostics: 503-494-0376 / maurom@ohsu.edu Center for Hematologic Malignancies is committed to lead in OHSU’s vision and mission of specialized/personalized care for leukemia, lymphoma, myeloma.. 47

Similar presentations





















 with Chronic Myeloid Leukemia (CML) and Philadelphia Chromosome-Positive Acute Lymphoblastic Leukemia (Ph+ ALL) Resistant or.>")

 Trial (DASISION, CA180-056)1.>")



>")
: ENESTnd Beyond One Year Larson.>")


 Cortes JE et al. Proc ASH 2013;Abstract 1483.>")


 vs Imatinib (IM) in Patients (pts) with Newly Diagnosed Chronic Myeloid Leukemia in Chronic Phase (CML-CP) and the Impact.>")
