Download presentation
Presentation is loading. Please wait.

1
Assessment thorax & lungs
by Mrs. Hamdia Mohammed

2
Assessment thorax & lungs
Learning Objectives: Describe the normal shape and size of the thorax. List the deformities in the chest. Describe the normal breath sounds. Differentiate between adventitious breath sounds. Determine the normal and abnormal findings in ass. of thorax &lunges.

3
Assessment thorax & lungs
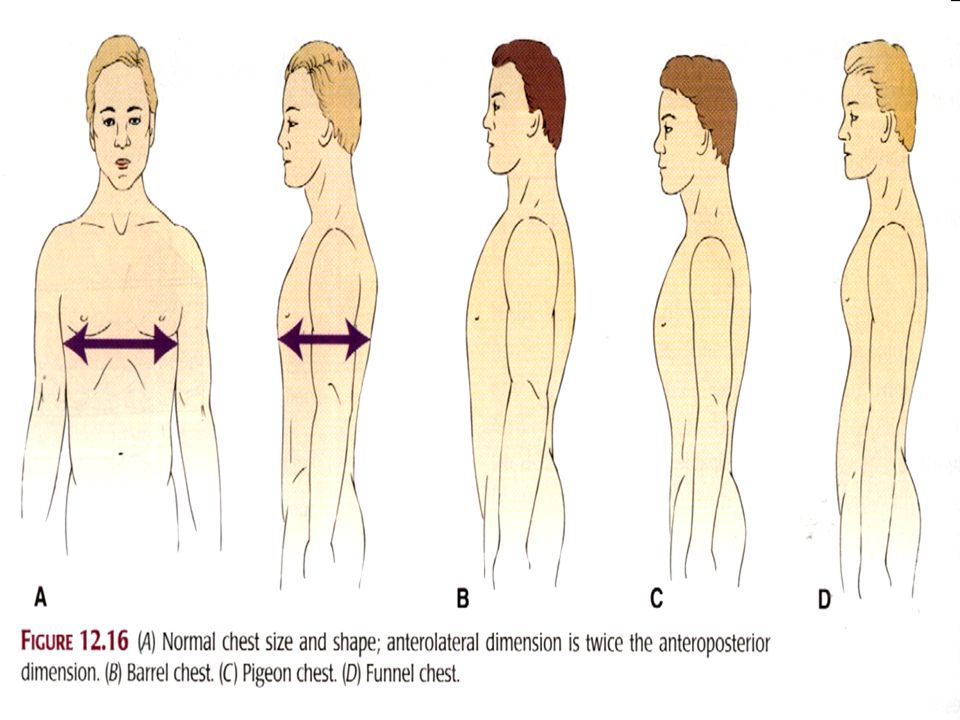
Chest shape and size: The thorax is oval. Its anteroposterior diameter is half its transverse diameter. Its diameter is smaller at the top than at the base. Deformities of the chest: Pigeon chest: a permanent deformity, may be caused by rickets. Characteristics: Narrow transverse diameter. Increased anteroposterior diameter. Protruding sternum.

4
Assessment thorax & lungs
A funnel chest, a congenital defect, is the opposite of pigeon chest. Characteristics: Narrow anteroposterior diameter. Depressed sternum. Depressed sternum make abnormal pressure on the heart may result in altered function.

5
Assessment thorax & lungs
A barrel chest: the ratio of the anteroposterior diameter and transverse diameter is 1:1 e.g., in clients with kyphosis and emphysema. Scoliosis: is a lateral deviation of the spine.

7
Funnel chest

8
Factors may be affecting on patient’s respiratory function.
Pregnancy. Age. Circulatory problems( anemia). Trauma. Environment . Path physiology ( COPD ). Allergy.
. Trauma. Environment . Path physiology ( COPD ). Allergy.")
9
Normal Breathing Sounds
types Description Location Characteristics Vesicular Soft intensity Low pitched. Sounds created by air moving through small airways Over peripheral lung, best heard at the base of the lungs. The inspiratory phase is 2.5 times longer than expiratory phase. Broncho-vesicular Moderate intensity Moderate pitched “blowing” sounds created by air moving through larger airway. Between the scapulae & the lateral to the sternum at the first and second intercostal space. Equal inspiratory and expiratory phase. Bronchial (tubular) High pitched. Loud “harsh” sounds created by air moving through the trachea. Anteriorly over the trachea not normally heard over the lungs tissue. Have a short inspiratory phase and long expiratory phase.
 High pitched. Loud harsh sounds created by air moving through the trachea. Anteriorly over the trachea not normally heard over the lungs tissue. Have a short inspiratory phase and long expiratory phase.")
11
Abnormal Breathing Sounds
Types Description Cause Location Crackles (rales) Fine, short, interrupted. Sound can be stimulate by rolling a lock of hair near the ear. Air passing through fluid or mucus in any air passage. Heard in the bases of lower lung lobes. Gurgles (rhonchi) Continuous, low pitched, gurgling, harsh, louder sounds with moaning (complaining). Air passing throw a narrow air passage due to secretion, tumors, swelling. Heard over most lung areas but predominate over the trachea and bronchi. Friction rub Superficial grating (harsh) or creaking. Rubbing together of inflamed pleural surfaces. Heard over the areas of greatest thoracic expansion. Wheeze (expiration) High pitched, squeaky (noisy) musical sounds. Air passing throw constricted bronchus. Heard over all lung field.
 Fine, short, interrupted. Sound can be stimulate by rolling a lock of hair near the ear. Air passing through fluid or mucus in any air passage. Heard in the bases of lower lung lobes. Gurgles (rhonchi) Continuous, low pitched, gurgling, harsh, louder sounds with moaning (complaining). Air passing throw a narrow air passage due to secretion, tumors, swelling. Heard over most lung areas but predominate over the trachea and bronchi. Friction rub. Superficial grating (harsh) or creaking. Rubbing together of inflamed pleural surfaces. Heard over the areas of greatest thoracic expansion. Wheeze. (expiration) High pitched, squeaky (noisy) musical sounds. Air passing throw constricted bronchus. Heard over all lung field.")
13
Assessing the thorax and lungs:
Anterior thorax: Assess respiratory excursion . Palpate tactile fremitus Percussion sounds on the anterior chest. Posterior thorax Assess respiratory excursion

14
A) Inspection:
 Inspection:")
15
Assessment thorax & lungs
Ass. Of posterior chest Normal findings Deviations from normal Inspect the shape and symmetry of posterior and lateral views. Compare the anteroposterior diameter to the transverse diameter. Anteroposterior to the transverse diameter in ratio of 1:2 Chest symmetric Barrel chest, increased anteroposterior diameter to the transverse diameter. Chest a symmetric

16
Assessment thorax & lungs
Ass. Of posterior chest Normal findings Deviations from normal Inspect the spinal alignment for deformities. Have the client stand from a lateral position, observe the three normal curvatures: cervical, thoracic, and lumbar. Spine vertically aligned Exaggerated spinal curvatures (kyphosis, lordosis).
.")
17
Assessment thorax & lungs
Ass. Of posterior chest Normal findings Deviations from normal To assess for lateral deviation of spine (scoliosis), observe the standing clients from the rear (back). The client bend forward at the waist and observe from behind Spinal column is straight, right and left shoulders and hips are at the same height Spinal column deviates to one side, often accentuated when bending (twisting) over. Shoulders or hips not even (constant)
, observe the standing clients from the rear (back). The client bend forward at the waist and observe from behind. Spinal column is straight, right and left shoulders and hips are at the same height. Spinal column deviates to one side, often accentuated when bending (twisting) over. Shoulders or hips not even (constant)")
18
b) Palpation:
 Palpation:")
19
Assessment thorax & lungs
Ass. of posterior chest Normal findings Deviations from normal Palpate the posterior thorax: Assess the temperature and integrity of all chest skin. Skin intact, uniform T. Skin lesions, areas of hyperthermia.

20
Assessment thorax & lungs
Ass. Of posterior chest Normal findings Deviations from normal If the clients have R. complaints: Palpate all chest areas for bulges, tenderness, or abnormal movements. Avoid deep palpation for painful areas, especially if a fractured rib is suspected. Chest wall intact, no tenderness, no masses. Lumps, bulges, depressions, areas of tenderness, movable structures (e.g., rib).
.")
21
Assessment thorax & lungs
Ass. Of posterior chest Normal findings Deviations from normal Palpate the posterior chest for respiratory excursion (thoracic expansion). Place the palms of both your hands over the lower thorax with your thumbs adjacent (next) to the spine and your fingers stretched laterally. Ask the client to take a deep breath while you observe the movement of your hands and any lag in movement. Full and symmetric chest expansion (i.e., when the clients takes a deep breath, your thumbs should move apart an equal distance and at the same time, normally the thumbs separate 3 to 5 cm. A symmetric and/or decreased chest expansion.
. Place the palms of both your hands over the lower thorax with your thumbs adjacent (next) to the spine and your fingers stretched laterally. Ask the client to take a deep breath while you observe the movement of your hands and any lag in movement. Full and symmetric chest expansion (i.e., when the clients takes a deep breath, your thumbs should move apart an equal distance and at the same time, normally the thumbs separate 3 to 5 cm. A symmetric and/or decreased chest expansion.")
22
Assessment thorax & lungs

23
Assessment thorax & lungs
Ass. Of posterior chest Normal findings Deviations from normal Palpate the chest for tactile fremitus, vibration felt through the chest wall when the clients speaks. Bilateral symmetry of tactile fremitus. Fremitus is heard most clearly at the apex of the lungs Decreased or absent fremitus. Increased fremitus as in pneumonia.

24
Assessment thorax & lungs
Ass. Of posterior chest Normal findings Place the palmar surfaces of your fingertips, starting near the apex of the lungs. *Ask the client to repeat such words as “blue moon” or “one, two,…… *Repeat the two steps, moving your hands sequentially to the base of the lungs. Low pitched voices of males are more readily palpated than higher pitched voices of males

25
Areas and sequence of palpating tactile fremitus
Assessing tactile fremitus

26
Assessment thorax & lungs
Ass. Of posterior chest Normal findings Deviations from normal Compare the fremitus on both lungs and between the apex and the base of each lung.

27
C)Percussion:
Percussion:")
28
Assessment thorax & lungs
Ass. Of posterior chest Normal findings Deviations from normal Objective of percussion: *To determine whether underlying lung tissue is filled with air, liquid, or solid material. *To determine the positions & boundaries of certain organs to a depth of 5 : 7 cm., it detects superficial rather than deep lesions Percussion notes resonance A symmetry Areas of dullness over the lung (associated with consolidation of lung tissue or a mass).
.")
30
Percussion elicits 5 types’ sounds:-
Flatness. Dullness. Resonance. Hyper resonance. Tympany.

31
Assessment thorax & lungs
Ass. Of posterior chest percuss the intercostal spaces in a systematic sequence. compare one side of the lung with the other. Percuss the lateral thorax starting at the axilla and working down to the eight rib.

32
Assessment thorax & lungs
Ass. of posterior chest Normal findings Deviations from normal Percuss for diaphragmatic excursion (movements of the diaphragm during maximal inspiration and expiration). Ask the clients to take a deep breath and hold it while you percuss downward along the scapular line until dullness is produced at the level of diaphragm. Repeat the procedure on the other side of the chest. *Excursion is 3:5 cm. bilaterally in women and 5:6cm. In men. *Diaphragm is usually slightly higher on the right side Restricted excursion associated with lung disorders
. Ask the clients to take a deep breath and hold it while you percuss downward along the scapular line until dullness is produced at the level of diaphragm. Repeat the procedure on the other side of the chest. *Excursion is 3:5 cm. bilaterally in women and 5:6cm. In men. *Diaphragm is usually slightly higher on the right side. Restricted excursion associated with lung disorders.")
33
d)Auscultaion:
Auscultaion:")
34
Auscultation Is the process of listening to sounds produced within the body. Done by: Unaided ear. Stethoscope. Types of auscultation: Direct auscultation. Indirect auscultation.

35
Assessment thorax & lungs
Ass. Of posterior chest Normal findings Deviations from normal Auscultate the chest using the flat disc diaphragm of the stethoscope. Use the systematic zigzag procedure used in percussion. Ask the client to take slow, deep breaths through the mouth. Listen at each point to the breath sounds during a complete inspiration and expiration. Vesicular and bronchovesicular breath sounds. Crackles, gurgles, wheeze, friction rub. Absence of breath sounds.

36
Assessment thorax & lungs
Ass. Of posterior chest Normal findings Deviations from normal Compare findings at each point with the corresponding point on the opposite side of the chest.

37
Assessment thorax & lungs
Ass. Of anterior thorax Normal findings Deviations from normal Anterior thorax: Inspect breathing patterns. Inspect the costal angle. Palpate the anterior chest (as in posterior chest) Quiet, rhythmic, and effortless respirations. Costal angle is less than 90 degree, and the ribs insert into the spine at approximately a 45 angle. Abnormal breathing patterns and sounds. Costal angle is widened associated with COPD
 Quiet, rhythmic, and effortless respirations. Costal angle is less than 90 degree, and the ribs insert into the spine at approximately a 45 angle. Abnormal breathing patterns and sounds. Costal angle is widened associated with COPD.")
38
Assessment thorax & lungs
Ass. of anterior thorax Normal findings Deviations from normal Palpate the anterior chest excursion (outing). Palpate the tactile fremitus Full symmetric excursion, thumbs normally separate 3 : 5 cm. Same as posterior vocal fremitus A symmetric and/or decreased respiratory excursion.
. Palpate the tactile fremitus. Full symmetric excursion, thumbs normally separate 3 : 5 cm. Same as posterior vocal fremitus. A symmetric and/or decreased respiratory excursion.")
39
Assessment thorax & lungs
Ass. of anterior thorax Normal findings Deviations from normal Percuss the anterior chest systematically. Begin above the clavicles in the supraclavicular space, and proceed downward to the diaphragm Compare one side of the lung to the other. Percussion notes: Resonance. Flatness. Dullness. Tympanic. A symmetry in percussion notes Areas of dullness or flatness over lung tissue

40
Assessment thorax & lungs
Ass. Of anterior thorax Normal findings Deviations from normal Auscultate the trachea. Auscultate the anterior chest (beginning over the bronchi between the sternum and the clavicles . Document findings. Bronchial and tubular breath sounds. Bronchovesicular breath sounds. Adventitious breath sounds.

41
Best Wishes Best Wishes

Similar presentations






















>")