Download presentation
Presentation is loading. Please wait.

1
Chapter 11 Blood vessels

2
TOPICS Vascular wall responses Congenital Anomalies Atherosclerosis
Arteriosclerosis Hypertension Aneurysms Vasculitides Raynaud “phenomenon” Veins Lymphatics Tumors Interventions

3
NORMAL VESSELS Arterial walls are thicker than veins To accommodate pulsatile flow and higher blood pressures.

4
Structure of blood vessels
Tunica intima Endothelium and connective tissue Tunica media Smooth muscle and elastic tissue Tunica externa or tunica adventitia Connective and elastic tissue

5
Arteries Large arteries are elastic (conducting) arteries – pressure reservoirs Medium arteries are muscular (distributing) arteries – more smooth muscle Contraction or relaxation of muscle changes the size of the lumen, and so controls the blood pressure in the vessel.
 arteries – more smooth muscle. Contraction or relaxation of muscle changes the size of the lumen, and so controls the blood pressure in the vessel.")
6
Capillaries Only a single layer of endothelium and a basement membrane
Connect arterioles and venules Functional part of system True capillaries begin at a precapillary sphincter which controls blood flow through the capillary

7
Veins Relatively thin; less elastic Larger in diameter than arteries
Have valves to prevent backflow of blood Flow to heart is assisted by contraction of skeletal muscles

8
Veins have larger diameters, larger lumina, and thinner, less well-organized walls
veins are more prone to dilation, compression, and easy penetration by tumors and inflammatory processes.

9
Lymphatics are thin-walled, endothelium-lined channels that drain excess interstitial tissue fluid eventually returning it to blood via the thoracic duct. Lymphatic flow also contains mononuclear inflammatory cells and a host of proteins; by passing through lymph nodes,

10
Functions of the lymphatics
1. lymphatics constitute an important pathway for continuous sampling of peripheral tissues for infection. 2.These channels can also disseminate disease by transporting microbes or tumor cells from distant sites to lymph nodes and eventually to the systemic circulation

11
The main cellular components of the walls of vessels are:
1) endothelial cells 2) smooth muscle cells 3) pericytes (the cells normally arranged along capillaries and venules)
 endothelial cells. 2) smooth muscle cells. 3) pericytes (the cells normally arranged along capillaries and venules)")
12
Endothelial cells: a) serve as a semipermeable membrane, b) regulate thrombosis, thrombolysis and platelet adherence, c) influate vascular tone and blood flow, d) metabolize hormones, e) regulate immune and inflammatory reactions, f) modify lipoptoteins in the artery wall, g) regulate the growth of other cell types, including smooth muscle cells.
 influate vascular tone and blood flow, d) metabolize hormones, e) regulate immune and inflammatory reactions, f) modify lipoptoteins in the artery wall, g) regulate the growth of other cell types, including smooth muscle cells.")
13
Endothelial injury is critical to the formation of thrombi, to the initiation of atherosclerosis and the vascular effects of hypertension and other disorders !!

14
Endothelial dysfunction
Endothelial activation

15
Pathology of blood and lymphatic vessels
The term endothelial dysfunction is often used to describe several types of potentially reversible changes in the functional state of endothelial cells that occur in response to environmental stimuli.

16
The term endothelial activation reflects alterations in gene expression and protein synthesis.
Inducers of endothelial activation include cytokines and bacterial products (which cause inflammatory injury and septic shock), hemodynamic stress and lipid products (involved in pathogenesis of atherosclerosis), advanced glycosylation of end products (involved in pathogenesis of diabetes), as well as viruses, complement components and hypoxia..
, hemodynamic stress and lipid products (involved in pathogenesis of atherosclerosis), advanced glycosylation of end products (involved in pathogenesis of diabetes), as well as viruses, complement components and hypoxia..")
17
Activated endothelial cells also elaborate adhesion molecules, other cytokines and chemokines, growth factors, molecules of the major histocompatibility complex (MHC), procoagulant or anticoagulant factors and vasoactive molecules that are involved either in vasoconstriction or in vasodilatation
, procoagulant or anticoagulant factors and vasoactive molecules that are involved either in vasoconstriction or in vasodilatation")
18
2) Smooth muscle cells are capable:
a)to mediate vasoconstriction, By Nitric oxide b) to mediate vasodilatation, c) to synthesize the collagen, elastin, and proteoglycans, d) to elaborate the growth factors and cytokines, e) to proliferate, and f) to migrate to the intima. 3) Pericytes have role as supportive and connective elements.
to mediate vasoconstriction, By Nitric oxide. b) to mediate vasodilatation, c) to synthesize the collagen, elastin, and proteoglycans, d) to elaborate the growth factors and cytokines, e) to proliferate, and. f) to migrate to the intima. 3) Pericytes have role as supportive and connective elements.")
19
Diseases of arterias A) Congenital anomalies B) Atherosclerosis C) Hypertensive vascular disease D) Inflammatory disease – Arteritides (Vasculitides) E) Raynaud disease F) Aneurysms a dissections
 Inflammatory disease – Arteritides (Vasculitides) E) Raynaud disease. F) Aneurysms a dissections.")
20
Congenital anomolies AVM Arterio Venous malformations Abnormal communication between the high pressure arteries and low pressure veins. Usually congenital but acquried by trauma or inflammation. Most often described in Brain as AVM Asymptomatic or hemorrhage or pressure effect.

21
Diseases of arterias B. Atherosclerosis
It is a generic term for three patters of vascular disease that have in common thickening and loss of elasticity of arterial walls: 1) Atherosclerosis – characterized by the formation of intimal fibrous plaques that often have a central core rich in lipid (fibrofatty plaques). 2) Mönckeberg medial calcific sclerosis – characterized by calcific deposits in medium-sized muscular arteries in persons older than 50 years. These medial lesions forming irregular medial plates or discrete transverse rings have much less clinical importance. 3) Arteriosclerosis – the hyaline and hyperplastic thickening of small arteries and arterioles which causes luminal narrowing and down stream ischemic injury.
 Atherosclerosis – characterized by the formation of intimal fibrous plaques that often have a central core rich in lipid (fibrofatty plaques). 2) Mönckeberg medial calcific sclerosis – characterized by calcific deposits in medium-sized muscular arteries in persons older than 50 years. These medial lesions forming irregular medial plates or discrete transverse rings have much less clinical importance. 3) Arteriosclerosis – the hyaline and hyperplastic thickening of small arteries and arterioles which causes luminal narrowing and down stream ischemic injury.")
22
Monckeberg arteriosclerosis (medial calcific sclerosis) involves the media of medium sized muscular arteries, most typically the radial and ulnar arteries, persons older than 50 years of age. It does not obstruct arterial flow because the intima is not involved. a. Ring-like calcifications in the media of the arteries are characteristic. b. Stiff, calcific "pipestem" arteries result. c. This form of arteriosclerosis may coexist with atherosclerosis, but it is distinct from and unrelated to it.

23
ARTERIO-SCLEROSIS GENERIC term for ANYTHING which HARDENS arteries
Atherosclerosis (99%) Mönckeberg medial calcific sclerosis (1%) Arteriolosclerosis, involving small arteries and arterioles, generally regarded as NOT strictly being part of atherosclerosis, but more related to hypertension and/or diabetes Atherosclerosis and arteriosclerosis are often used so interchangeably, it is hardly worth differentiating them anymore, other than to know they are different!
 Mönckeberg medial calcific sclerosis (1%) Arteriolosclerosis, involving small arteries and arterioles, generally regarded as NOT strictly being part of atherosclerosis, but more related to hypertension and/or diabetes. Atherosclerosis and arteriosclerosis are often used so interchangeably, it is hardly worth differentiating them anymore, other than to know they are different!")
24
Hyaline Arteriolosclerosis
Hyaline Arteriolosclerosis. This vascular lesion consists of a homogeneous pink hyaline thickening of the walls of arterioles with loss of underlying structural detail and with narrowing of the lumen. Present in Elderly patients, whether normotensive or hypertensive, patients with hypertension. It is also common as part of the characteristic microangiography in diabetes .

25
HISTOPATHOLOGY of ESSENTIAL HYPERTENSION
Often, benign or “malignant” hypertension is described as two different types of changes in arterioles, usually renal. Benign: Hyalization of arteriole wall Malignant: Fibrinoid necrosis and “onion skinning” of arteriole wall “HYALINE” = BENIGN HTN. “HYPERPLASTIC” = MALIGNANT HTN. SYS> ) ONION SKIN 2) “FIBRINOID” NECR.
 ONION SKIN 2) FIBRINOID NECR.")
26
Hyperplastic Arteriolosclerosis. Seen in
Malignant hypertension (typically, diastolic pressures over 120 mm Hg associated with acute cerebral and/or renal injury). Hyperplastic arteriolosclerosis is associated with "onion-skin," concentric, laminated thickening of the walls of arterioles with luminal narrowing The laminations consist of SMCs and thickened, duplicated basement membrane.
. Hyperplastic arteriolosclerosis is associated with onion-skin, concentric, laminated thickening of the walls of arterioles with luminal narrowing The laminations consist of SMCs and thickened, duplicated basement membrane.")
27
In malignant hypertension, these hyperplastic changes are accompanied by fibrinoid deposits and vessel wall necrosis (necrotizing arteriolitis), particularly prominent in the kidney.
, particularly prominent in the kidney.")
29
HYPERTENSION “ESSENTIAL” % “SECONDARY” 5%

30
Primary hypertension Also called essential or idiopathic hypertension
% of all cases No specific cause identified Can happen with retention of sodium and water → increased blood volume. Also low dietary potassium, calcium and magnesium intakes

31
Suspected causes Interaction of genetics and environment
Overactivity of sympathetic nervous system Overactivity of renin / angiotensin/ aldosterone system Salt and water retention by kidneys And others

32
SECONDARY Renal Endocrine
Acute glomerulonephritis Chronic renal disease Polycystic disease Renal artery stenosis Renal artery fibromuscular dysplasia Renal vasculitis Renin-producing tumors Endocrine Adrenocortical hyperfunction (Cushing syndrome, primary aldosteronism, congenital adrenal hyperplasia, licorice ingestion) Exogenous hormones (glucocorticoids, estrogen [including pregnancy-induced and oral contraceptives], sympathomimetics and tyramine-containing foods, monoamine oxidase inhibitors) Pheochromocytoma, Acromegaly, Hypothyroidism (myxedema), Hyperthyroidism Pregnancy-induced Cardiovascular: Coarctation of aorta, Polyarteritis nodosa (or other vasculitis) Increased intravascular volume MISC: Increased cardiac output, Rigidity of the aorta, Neurologic, Psychogenic, Increased intracranial pressure, Sleep apnea, Acute stress, including, surgery
 Exogenous hormones (glucocorticoids, estrogen [including pregnancy-induced and oral contraceptives], sympathomimetics and tyramine-containing foods, monoamine oxidase inhibitors) Pheochromocytoma, Acromegaly, Hypothyroidism (myxedema), Hyperthyroidism. Pregnancy-induced Cardiovascular: Coarctation of aorta, Polyarteritis nodosa (or other vasculitis) Increased intravascular volume. MISC: Increased cardiac output, Rigidity of the aorta, Neurologic, Psychogenic, Increased intracranial pressure, Sleep apnea, Acute stress, including, surgery.")
33
Always know that hypertension can be understood best by remembering the simple BP=COxPR equation.

34
ReninAngiotensinAldosterone AXIS (RAAS)
If the perfusion of the juxtaglomerular apparatus in the kidneys decreases, then the juxtaglomerular cells release the enzyme renin. Renin cleaves an inactive peptide called angiotensinogen, converting it into angiotensin I. Angiotensin I is then converted to angiotensin II by angiotensin-converting enzyme (ACE), which is found mainly in lung capillaries. Angiotensin II is the major bioactive product of the renin-angiotensin system. Angiotensin II acts as an endocrine, autocrine/ paracrine, and intracrine hormone. Sometimes this is called RAAS Renin Angiotensin (but angiotensis does SO MUCH MORE than just activate aldosterone) Aldosterone Sodium
, which is found mainly in lung capillaries. Angiotensin II is the major bioactive product of the renin-angiotensin system. Angiotensin II acts as an endocrine, autocrine/ paracrine, and intracrine hormone. Sometimes this is called RAAS. Renin Angiotensin (but angiotensis does SO MUCH MORE than just activate aldosterone) Aldosterone Sodium.")
35
GENETIC ACQUIRED A little more thorough diagram of RAAS pathology---- genetic and acquired.

36
GENETIC vs. ENVIRONMENTAL
GENETIC UN-CONTROLLABLE ENVIRONMENTAL CONTROLLABLE STRESS OBESITY SMOKING PHYSICAL ACTIVITY NaCl INTAKE

37
ATHEROSCLEROSIS (classical)
Etiology/Risk Factors Pathogenesis Morphology Clinical Expression

38
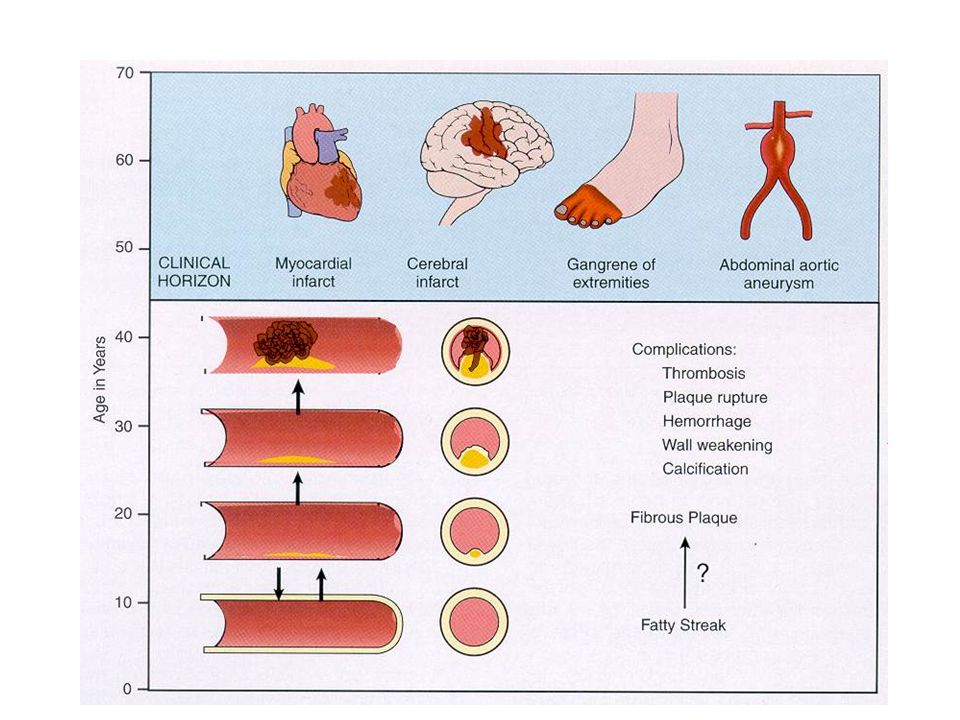
FATTY STREAK (non-palpable, but a visible YELLOW streak)
2) ATHEROMA (plaque) (palpable) 3) THROMBUS (non-functional, symptomatic) Atherosclerosis is a LIFELONG, even childhood, process. This chart is worth knowing.
 ATHEROMA (plaque) (palpable) 3) THROMBUS (non-functional, symptomatic) Atherosclerosis is a LIFELONG, even childhood, process. This chart is worth knowing.")
39
Risk Factors for Atherosclerosis
Major Minor NON-modifiable Modifiable Increasing age Obesity Male gender Physical inactivity Family history Stress ("type A" personality) Genetic abnormalities Postmenopausal estrogen deficiency High carbohydrate intake Modifiable Hyperlipidemia Alcohol Hypertension Lipoprotein Lp(a) Cigarette smoking Hardened (trans)unsaturated fat intake Diabetes Chlamydia pneumoniae
 Genetic abnormalities. Postmenopausal estrogen deficiency. High carbohydrate intake. Modifiable. Hyperlipidemia. Alcohol. Hypertension. Lipoprotein Lp(a) Cigarette smoking. Hardened (trans)unsaturated fat intake. Diabetes. Chlamydia pneumoniae.")
40
MAJOR factors Hyperlipidemia Hypertension Cigarette Smoking
Diabetes Milletus “Framingham” data. Please remember that these are the ONLY four MAJOR risk factors. If somebody tells you there is anything else which is a MAJOR risk factor, nominate that joker for a Nobel prize.

41
PATHOGENESIS “atherosclerosis is a chronic inflammatory response of the arterial wall initiated by injury to the endothelium”

42
PATHOGENESIS Chronic endothelial injury
LDL, Cholesterol in arterial WALL OXIDATION of lipoproteins Monocytes migrate endothelium* Platelet adhesion and activation Migration of SMOOTH MUSCLE from media to intima to activate macrophages (foam cells) Proliferation of SMOOTH MUSCLE and ECM Accumulation of lipids in cells and ECM Like the sequence of events described in acute inflammation, atherosclerosis is its own Cecil B. DeMille saga! Not only should you all be familiar with these processes, but their ORDER as well. * This may be the first (i.e., earliest) microscopic and gross finding.
 Proliferation of SMOOTH MUSCLE and ECM Accumulation of lipids in cells and ECM. Like the sequence of events described in acute inflammation, atherosclerosis is its own Cecil B. DeMille saga! Not only should you all be familiar with these processes, but their ORDER as well. * This may be the first (i.e., earliest) microscopic and gross finding.")
43
This is the VERY VERY best diagram of atherosclerosis you will ever see. The nice thing about diagrams is that you really do not have to memorize them, but just visually “recall” the concepts!

44
A very well constructed graphic understanding of the pathogenesis of atherosclerosis. Please be expected to not only KNOW these five items, but their correct ORDER too.

45
The mechanism of Hyperlipidemia contributing to Atherosclerosis
Endothelial impairment by chronic hyperlipidemia by increasing o2 free radicles production Decay in NO Impair vaso dilation Impair endothelial functiuon Oxidise the LDL

46
Fatty streak is the earliest lesion in Atherosclerosis
Composition Atherosclerotic plaques Components Smoothmuscle cells macrophages and t cells ECM Intracellualr and extracellular lipids.

47
Fatty STREAKS can be SEEN as YELLOW, but NOT palpated, ATHEROMAS can be palpated, thrombi are symptomatic often. A rule of thumb is that stenosis is symptomatic if > 90%.

48
MORPHOLOGIC CONCEPTS Macrophages (really monocytes) infiltrate
Intimal Thickening Lipid Accumulation Streak Atheroma Smooth Muscle Hyperplasia and Migration Fibrosis Calcification Aneurysm Thrombosis These are also, generally, in order of severity.

49
Cholerterol (really cholesterol esters) makes macrophages “foamy” and cause “clefts” extracellularly. PLAQUE

50
MILD ADVANCED

51
ADVANCED FEATURES RUPTURE ULCERATION EROSION ATHEROEMBOLI HEMORRHAGE
THROMBOSIS ANEURYSM These should all be household words in your vocabulary.

52
ANEURYSMS TRUE vs. FALSE ATHEROSCLEROTIC NON-ATHEROSCLEROTIC
CONGENITAL LUETIC (SYPHILITIC) TRAUMATIC “MYCOTIC” (MIS-leading term) 2° to VASCULITIS SACCULAR (i.e., “Berry”) vs. FUSIFORM DISSECTION vs. NON-DISSECTION
 TRAUMATIC. MYCOTIC (MIS-leading term) 2° to VASCULITIS. SACCULAR (i.e., Berry ) vs. FUSIFORM. DISSECTION vs. NON-DISSECTION.")
53
An aneurysm is a localized abnormal dilation of a blood vessel or the heart
When an aneurysm involves all three layers of the arterial wall (intima, media, and adventitia) or the attenuated wall of the heart, it is called a "true" aneurysm false aneurysm (also called pseudoaneurysm) is a breach in the vascular wall leading to an extravascular hematoma that freely communicates with the intravascular space ("pulsating hematoma").
 or the attenuated wall of the heart, it is called a true aneurysm. false aneurysm (also called pseudoaneurysm) is a breach in the vascular wall leading to an extravascular hematoma that freely communicates with the intravascular space ( pulsating hematoma ).")
54
Know the difference between a TRUE (endothelial expansion) and FALSE (NO endothelial expansion) aneurysm
 and FALSE (NO endothelial expansion) aneurysm")
55
True Aneurysms Atherosclerotic. Syphilitic,Congenital Ventricular False aneurysms Ventricular ruptuture after MI

56
They are of 2 types Saccular Fusiform <ost common causes of aneurysm Atherosclerosis Hypertension

57
Pathogenesis 1.The intrensic quality of the vascular wall conncetive tissue is poor Eg Marfan syndrome Loeys Deitz syndrome Ehlers Danlos syndrome

58
2.The balance of collagen synthesis and degradation is altered by inflammatory. Infiltration and destructive proteolytic enzymes. Increaesed production of MMP by macrophages in atherosclerosis or vasculitis Also decreased in tissue MMP inhibitors

59
3.The vascular wall weakend through loss of smooth muscle cells.
Hypoxia due to athermanous plaque and leads to ischemia and HT in turn leads to smooth muscle loss and scarring and decreased synthesis of ECM and increased amount of gycosaminoglycons called as cystic medial degeneration seen in Marfan syndrome and scurvy.

60
Most abdominal aortic aneurysms (AAA) occur between the renal arteries and the bifurcation of the aorta
 occur between the renal arteries and the bifurcation of the aorta")
61
Abdominal Aortic Aneurysm
Atherosclerosis, the most common cause of aneurysms, causes thinning and weakening of the media secondary to intimal plaques. Site-. Atherosclerotic aneurysms occur most frequently in the abdominal aorta (abdominal aortic aneurysm, often abbreviated AAA), but the common iliac arteries, the arch, and descending parts of the thoracic aorta can also be involved.
, but the common iliac arteries, the arch, and descending parts of the thoracic aorta can also be involved.")
62
Pathogenesis AAA occurs more frequently in men and rarely develops before age 50. Atherosclerosis is a major cause of AAA, but there are clearly other contributors, since the incidence is less than 5% in men older than 60 years,

63
Two AAA variants Inflammatory AAAs are characterized by dense periaortic fibrosis containing abundant lymphoplasmacytic infiltrate with many macrophages and often giant cells. Their cause is uncertain.

64
Mycotic AAAs are atherosclerotic lesions infected by lodging of circulating microorganisms in the wall, particularly in the setting of bacteremia from a primary Salmonella gastroenteritis. In such cases, suppuration further destroys the media, potentiating rapid dilation and rupture.

65
Syphilitic ( luetic) aneurysm
a. This aneurysm is a manifestation of tertiary syphilis, which has become rare with better treatment and control of the disease. It is caused by syphilitic aortitis, which is characterized by obliterative endarteritis of the vasa vasorum and necrosis of the media. Grossly, these changes result in a "tree-bark" appearance

66
The narrowing of the lumina of the vasa vasorum causes ischemic injury of the aortic media, with patchy loss of the medial elastic fibers and muscle cells, followed by inflammation and scarring, the aorta loses its elastic recoil producing an aneurysm. Contraction of fibrous scars may lead to wrinkling of intervening segments of aortic intima, grossly reminiscent of "tree bark."

67
Unlike atherosclerotic aneurysms, syphilitic aneurysms characteristically involve the
ascending aorta. Dilation of the ascending aorta may widen the aortic commissures, leading to aortic valve insufficiency

68
Clinical features The clinical features depend on the consequences of the AAA Rupture into peritoneal cavity leads to fatal hemorrhage Obstruction into the branch leads to ischemic injury Embolsim

69
Compression of the adjucent structures like urter or vertebral erosion
the risk of ruture depends upon the sizes a abdominal mass.

70
THORACIC ANEURYSMS Hypertnesion is common cause
Marfan syndrome and loeys Dietz syndrome Encroachment Respiratory difficulties Dysphagia Cough Pain Aortic valve dilatation Rupture

71
Dissection (i.e., blood or hemorrhage disrupting the wall of a large artery) can be both a cause or an effect of an aneurysm. DISSECTION

72
Aorrtic Dissection Blood splays apart the laminar planes of the media to form a blood-filled channel within the aortic wall this channel often ruptures through the adventitia and into various spaces, where it causes either massive hemorrhage or cardiac tamponade

73
(1) men aged 40 to 60 years, with antecedent hypertension (more than 90% of cases of dissection), and (2) younger patients with systemic or localized abnormalities of connective tissue affecting the aorta. 3.Iatrogenic following catheterization or bypass surgery. During and after pregnancy.
 younger patients with systemic or localized abnormalities of connective tissue affecting the aorta. 3.Iatrogenic following catheterization or bypass surgery. During and after pregnancy.")
74
Hypertension is the major risk factor.
There is medial hypertrophy of the vasa vasorum. Degenerative changes in the aortic media Loss of smoioth muscle cells The medial weakness trigger the intimal tear. There is cystic medial degeneration.

75
Clinical features. The more common (and dangerous) proximal lesions (called type A dissections), involving either the ascending aorta only or both the ascending and descending aorta. (types I and II of the DeBakey classification)Distal lesions not involving the ascending part and usually beginning distal to the subclavian artery (called type B dissections or DeBakey type III).
 proximal lesions (called type A dissections), involving either the ascending aorta only or both the ascending and descending aorta. (types I and II of the DeBakey classification)Distal lesions not involving the ascending part and usually beginning distal to the subclavian artery (called type B dissections or DeBakey type III).")
76
The classic clinical symptoms of aortic dissection are the sudden onset of excruciating pain, usually beginning in the anterior chest, radiating to the back between the scapulae, and moving downward as the dissection progresses; the pain can be confused with that of myocardial infarction.

77
The most common cause of death is rupture of the dissection into body cavities (i.e., pericardial, pleural, or peritoneal). Retrograde dissection into the aortic root can cause disruption of the aortic valvular apparatus. cardiac tamponade, aortic insufficiency, and myocardial infarction or extension of the dissection into the great arteries of the neck or into the coronary, renal, mesenteric, or iliac arteries

78
VASCULITIS Vasculitis, or inflammation of vessel walls 1.Immune mediated 2.Direct invasion by infectious agents.

79
an result from infections, but it more commonly has an immunologic basis such as immune complex deposition, ANCAs, or anti-EC antibodies.Different forms of vasculitis tend to specifically affect vessels of a particular caliber and location.

82
Patients with Vasculitis have circulating antibodies that react with the Neutrophil cytoplasmic antigens.

83
GIANT CELL ARTERITIS. It is the most common form of Vasculitis seen in elderly patients and It is a chronic typically granulomatous inflammation of large and small sized arteries.

84
“TEMPORAL” ARTERITIS Giant Cell Arteritis, GCA
ADULTS Mainly arteries of the head and temporal arteries are the most visibly, palpably, and surgically accessible BLINDNESS most feared sequelae GRANULOMATOUS WALL inflammation diagnostic OFTEN associated with marked ESR elevation to be then known as POLYMYALGIA RHEUMATICA Anti-NEUTROPHIL AB’s often POSITIVE

88
TAKAYASU ARTERITIS Involves aortic arch and other heavilly elastic arteries, i.e., chief thoracic aorta branches, most commonly young Asian women FEMALES <40 “PULSELESS” disease Granulomatous lesion.

89
TAKAYASU ARTERITIS Involves aortic arch and other heavilly elastic arteries, i.e., chief thoracic aorta branches, most commonly young Asian women FEMALES <40 “PULSELESS” disease Granulomatous lesion.

90
POLY-(Peri-) ARTERITIS NODOSA (PAN)
ANY MEDIUM or SMALL artery OFTEN visceral arteries NECROTIZING (fibrinoid) inflammation involving renal. coronary, mesenteric arteries spares pulmonary arteries
 inflammation. involving renal. coronary, mesenteric. arteries spares. pulmonary arteries.")
93
KAWASAKI DISEASE CHILDREN <4 years. CORONARY ARTERIES
LEADING cause of ACQUIRED heart disease in children USA and JAPAN Fatal in only 1%

94
Also it is Mucocutaneous lymphnode syndrome as it involves oral, conjuctival erythema and edema of hands and cervical lymphnode enlargement. It is associated with Mycoplasma and HIV infection in some cases. Untreated develop cardiovascular complications like pericarditis ,MI and aneurysm. Immunoglobulin and ASA is the treatment.

95
MICROSCOPIC POLYANGIITIS HYPERSENSITIVITY VASCULITIS LEUKOCYTOCLASTIC VASCULITIS
SMALL VESSELS OF ALL TYPES, e.g., capillaries and veins too FRAGMENTED NEUTROPHILS Called PAUCI IMMUNE INJURY Iittle or no immunoglobulins in most lesions. Necrotising GLOMERULONEPHRITIS in 90% of the patients. Most are ALLERGIC reactions to allergens like penicillin or strep DERMATOLOGIST’s DISEASE

96
WEGENER GRANULOMATOSIS
M>F, often in 40’s ACUTE NECROTIZING GRANULOMAS OF UPPER an LOWER respiratory tract NECROTIZING GRANULOMATOUS VASCULITIS of SMALL vessels of ALL types Often renal involvement, “crescentic” glomerulonephritis ANTI-NEUTROPHIL-CYTOPLASMIC-AB’s usually present Mortality has improved significantly, but flare-ups, i.e., recurrences, are still the main concern.

97
Clinical Features Patients present with Chronic Sinusitis, Pnemonitis, Hemoptysis and Hematuria, mucosal ulcerations of the nasopharynx Epistaxis,nasal crusting. Nodular infiltration and Glomerular nephritis .

98
Pathologically Wegener's Granulomatosis is characterized by three features: Necrotizing granulomatous inflammation of the upper and lower respiratory tracts. Disseminated small vessel necrotizing vasculitis that affects both arteries and veins. Focal necrotizing glomerulonephritis.

99
Diagnostic criteria for Wegener's Granulomatosis are, 1) Abnormal urine sediments, like red blood cells or casts, 2) An abnormal chest radiograph. 3) Oral ulcers or nasal discharge and 4) granulomatous inflammation on biopsy. Pathogenesis is believed to be a hypersensitivity reaction to infection with staphylococcus aureus and parvovirus B-19 [1
 Oral ulcers or nasal discharge and 4) granulomatous inflammation on biopsy. Pathogenesis is believed to be a hypersensitivity reaction to infection with staphylococcus aureus and parvovirus B-19 [1.")
101
necrosis granulomas necrosis granulomas necrosis granulomas
Why is the “necrosis” of Wegener’s not called “caseating”? Ans: Because, by tradition, rather than objectivity or logic, “caseation” has been attributed to tuberculosis. Yes, we know this is not fair.

102
CHURG - STRAUSS SYNDROME
Called as Allergic granulomatosis and Angitis. Associated with Asthma, rhinitis,lung infiltrates peripheral Eosinophilia,and Necrotising granulomas. Present with cutaneous purpura bleeding frm GIT and Focal and glomerulo sclerosis

103
Allergic granulomatosis and angiitis strong association with allergic rhinitis, bronchial asthma, and peripheral eosinophilia; p-ANCAs are present in roughly half the patients. In Churg-Strauss syndrome, and perivascular tissues by eosinophils. Unlike Wegener granulomatosis, severe renal disease is infrequent in Churg-Strauss syndrome; instead, coronary arteritis and myocarditis

104
THROMBOANGIITIS OBLITERANS BUERGER(‘s) Disease
100% caused by cigarette smoking MEN>>>F, 30’s, 40’s Often arteries are 100% obliterated, hence the name “obliterans” EXTREMITIES most often involved.

105
acute and chronic inflammation of medium-sized and small arteries, principally the tibial and radial arteries, with occasional secondary extension into extremity veins and nerves.

106
intravenous prostaglandin analogue.
Clinical Features The early manifestations are a superficial nodular phlebitis, Resting pain on the forefoot is characteristic, with possible ischemic ulcers or gangrene of foot/ toes; upper limb ischemia [40% to 50% of patients) with ulceration and gangrene; Raynaud's phenomenon. Treatment: smoking cessation essential; intravenous prostaglandin analogue.
 with ulceration and. gangrene; Raynaud s phenomenon. Treatment: smoking cessation essential; intravenous prostaglandin analogue.")
107
FINAL TOPICS Raynaud Phenomenon Veins and Lymphatics
Varicosities Thrombophlebitis/Phlebothrombosis SVC/IVC syndromes Lymphangitis Lymphedema Tumors: Benign, Intermediate (Borderline), Malignant Vascular Interventions: Angioplasty, Stents, Grafts
, Malignant. Vascular Interventions: Angioplasty, Stents, Grafts.")
108
RAYNAUD’S PHENOMENON. It is a vasospasm in the peripheral arteries due to cold and emotional stimuli. Pallor due to vasospasm Cynosis due to Rubor due to reactive hyperemia.

109
Raynaud “Phenomenon” PRIMARY: (formerly Raynaud “DISEASE”)
Digital PALLORCYANOSISHYPEREMIA (WHITE) (BLUE) (RED) Vasoconstriction usually triggered by COLD, emotion Can be tip of nose, not only digits Self Limited, Gangrene UN-common Arteries often do NOT show diagnostic pathology SECONDARY: (formerly Raynaud “Phenomen.”) Atherosclerosos SLE Buerger Disease
 (BLUE) (RED) Vasoconstriction usually triggered by COLD, emotion. Can be tip of nose, not only digits. Self Limited, Gangrene UN-common. Arteries often do NOT show diagnostic pathology. SECONDARY: (formerly Raynaud Phenomen. ) Atherosclerosos. SLE. Buerger Disease.")
110
RAYNAUD PHENOMENON There are two types of Raynaud phenomenon. Primary and Secondary Primary Raynaud phenomenon (previously called Raynaud disease) reflects an exaggeration of central and local vasomotor responses to cold or emotion,
 reflects an exaggeration of central and local vasomotor responses to cold or emotion,")
111
Structural changes in the arterial walls are absent except late in the course, when intimal thickening can appear. The course of primary Raynaud phenomenon is usually benign, but long-standing, chronic cases can result in atrophy of the skin, subcutaneous tissues, and muscles. Ulceration and ischemic gangrene rare.

112
WHITE BLUE RED

113
“Varicose” Veins 20% of population, Female 30% male 20%
Related to increased venous pressure, age, valve dysfunction Superficial veins of lower extremities most common PATH: 1) DILATED, 2) TORTUOUS, ) ELONGATED, 4) SCARRED (phlebosclerosis), 5) CALCIFICATIONS, 6) NON-UNIFORM SMOOTH MUSCLE Conceptually like varices or hemorrhoids
 DILATED, 2) TORTUOUS, 3) ELONGATED, 4) SCARRED (phlebosclerosis), 5) CALCIFICATIONS, 6) NON-UNIFORM SMOOTH MUSCLE. Conceptually like varices or hemorrhoids.")
114
. B. Varicose veins 1. Abnormally distended, lengthened, and tortuous veins 2. Locations a. Superficial saphenous veins (most common site) b. Distal esophagus (due to portal hypertension) c. Anorectal region (e.g.. hemorrhoids) d. Left scrotal sac (e.g., varicocele)
 c. Anorectal region (e.g.. hemorrhoids) d. Left scrotal sac (e.g., varicocele)")
115
Superficial varicosities; causes:;
a. Valve incompetence of perforator branches with reversal of blood flow from high-pressure deep venous System into superficial system. • Exacerbated by pregnancy, prolonged standing, obesity, oral contraceptives, advanced age Familial tendency c. Secondary to deep venous thrombosis • Retrograde blood How through peribrating branches into the superficial system

116
(1) Nonpharmacologic •Graded compression stockings (2) Chronic treatment (a) Compression sclerotherapy (b) Ligation and stripping (e) Endovenous obliteration using radiofreqency (diathermy) or laser.
 Ligation and stripping. (e) Endovenous obliteration using radiofreqency (diathermy) or laser.")
117
SEVERE VARICOSITIES

118
Phlebothrombosis 1. Thrombosis of vein with out inflammation. Causes Phlebothrombosis: a. Stasis of blood flow b. Hypercoagulability-(e.g.. antithrombin III deficiency) 3. Location a. Most often occurs in the deep vein of the calf b. Less common sites includes portal vein, hepatic vein, dural sinuses,
 3. Location. a. Most often occurs in the deep vein of the calf. b. Less common sites includes portal vein, hepatic vein, dural sinuses,")
119
(1) Swelling (2) Pain on dorsiflexion of foot (Homans' sign) and compression of the calf (3) Pitting edema distal to the thrombosis (increased hydrostatic pressure) Unilateral sometime bilateral either impaired venous or lymphatic return.
 Pitting edema distal to the thrombosis (increased hydrostatic pressure) Unilateral sometime bilateral either impaired venous or lymphatic return.")
120
SVC SYNDROME Usually from bronchogenic CA or mediastinal lymphoma
“DUSKY CYANOSIS” of: Head Neck Arms

121
Pathogenesis a. Extrinsic compression of the superior vena cava b. Due to a primary lung cancer (90% of cases) • Usually a small cell carcinoma of the lung 2. Clinical findings a, "Puffiness" and blue to purple discoloration of the face, arms, and shoulders b. Retinal hemorrhage, stroke 3. Treatment • Radiation; stent to bypass obstruction.

122
IVC SYNDROME Secondary to: Bilateral leg edema
NEOPLASMS (external compression) ASCENDING THROMBOSIS from FEMORALS, ILIACS AAA, Gravid uterus Bilateral leg edema Massive proteinuria if renal veins involved (like nephrotic syndrome)
 ASCENDING THROMBOSIS from FEMORALS, ILIACS. AAA, Gravid uterus. Bilateral leg edema. Massive proteinuria if renal veins involved (like nephrotic syndrome)")
123
LYMPHANGITIS From regional infections
Group-A beta-hemolytic strep most common Lymphatics dilated, filled with WBCs Cellulitis usually present too Lymphadenitis also usually follows If lymph nodes cannot filter (process) antigens enough septicemia
 antigens enough septicemia.")
124
Diseases of veins and lymphatics
E) Lymphangitis and Lymphedema Primary diseases – extremely uncommon. Secondary processes – develop in association with inflammation or cancer. Lymphangitis: bacterial infections spreading into and through the lymphatics. Obstructive lymphedema: Occlusions of lymphatic drainage by tumor, by postradiation fibrosis, by filariasis, trauma or by inflammatory thrombosis which is accompanied by abnormal accumulation of interstitial fluid in the affected part.
 Lymphangitis and Lymphedema. Primary diseases – extremely uncommon. Secondary processes – develop in association with inflammation or cancer. Lymphangitis: bacterial infections spreading into and through the lymphatics. Obstructive lymphedema: Occlusions of lymphatic drainage by tumor, by postradiation fibrosis, by filariasis, trauma or by inflammatory thrombosis which is accompanied by abnormal accumulation of interstitial fluid in the affected part.")
125
LYMPHANGIOMA Small 1-2 mm Simple or capillary type and Cavernous
90% Head and neck region in kids <2 Generally……RARE When large size and/or spaces present often called “CYSTIC HYGROMA”

126
Vascular TUMORS BENIGN (NEVER metastasize, in fact some are not even TRUE neoplasms, but hamartomas) INTERMEDIATE (rarely metastasize) MALIGNANT (FREQUENT and EARLY metastases, like any other sarcoma lung) Vascular tumors generally follow the same diagnostic patterns of other mesenchymal (i.e., “soft” tissue) tumors. Often the KEY difference is that “endothelium” lined blood filled spaces, or identification of endothelial cells by antigenic markers, such as factor VIII, is usually present.
 MALIGNANT (FREQUENT and EARLY metastases, like any other sarcoma lung) Vascular tumors generally follow the same diagnostic patterns of other mesenchymal (i.e., soft tissue) tumors. Often the KEY difference is that endothelium lined blood filled spaces, or identification of endothelial cells by antigenic markers, such as factor VIII, is usually present.")
127
Vascular tumors can be endothelium derived or
Arise from the cells support and or surrounds the vessel. Benign tumors produce obvious vascular channels filled with blood cells or lymph lined by normal endothelial layer Malignant are more cellular and show atypia.

128
HEMANGIOMA CAPILLARY (small vascular spaces)
Often a generic term for ANY benign blood vessel tumor very common tumor. 7% of infants and childhood tumor. CAPILLARY (small vascular spaces) Also called “juvenile”, often called “birth marks” Usually regress with age CAVERNOUS (LARGE vascular spaces) Also called “adult” Usually do NOT regress Small spaces = often small people, i.e., kids Large spaces = often large people, i.e., adults
 Also called juvenile , often called birth marks Usually regress with age. CAVERNOUS (LARGE vascular spaces) Also called adult Usually do NOT regress. Small spaces = often small people, i.e., kids. Large spaces = often large people, i.e., adults.")
129
A Hemangioma and D Pyogenic granuloma B Juvenile capillarty hemangioma C Cavernous hemangioma

130
Capillary hemangioma occurs on skin mucous membrane and oral cavity and lips
Strawberry or juvenile hemangioma of the skin is common.

131
Cavernous hemangiomas are a component of von Hippel-Lindau disease occurring within the cerebellum or brain stem and eye grounds, along with similar angiomatous lesions or cystic neoplasms in the pancreas and liver; von Hippel-Lindau disease is also associated with renal neoplasms.

132
Pyogenic granuloma It is a form of capillary hemangioma. Seen after a trauma usually reach in size about 2 to 3 cm after 6 weeks. There is also pregnancy tumor( granuloma gravidarum) They undergo fibrosis. Or need excision.
 They undergo fibrosis. Or need excision.")
133
Cystic Hygroma These lesions are typically found in the neck or axilla of children and, rarely, in the retroperitoneum; cavernous lymphangiomas of the neck are common in Turner syndrome These lesions can occasionally be enormous (≤15 cm in diameter) and may fill the axilla or produce gross deformities about the neck. Tumors are composed of massively dilated lymphatic spaces lined by ECs and separated by intervening connective tissue stroma containing lymphoid aggregates. The tumor margins are not discrete and the lesions are not encapsulated, making resection difficult.
 and may fill the axilla or produce gross deformities about the neck. Tumors are composed of massively dilated lymphatic spaces lined by ECs and separated by intervening connective tissue stroma containing lymphoid aggregates. The tumor margins are not discrete and the lesions are not encapsulated, making resection difficult.")
134
Cystic hygroma

135
Vascular Ectasias are common lesions characterized by local dilation of preexisting vessels; they are not true neoplasms. Telangiectasia is a term used for a congenital anomaly or acquired exaggeration of preformed vessels-usually in the skin or mucous membrane

136
Sturg weber syndrome

137
Nevus Flammeus Spider Telangiectasia Hereditary Hemorrhagic Telangiectasia (Osler-Weber-Rendu Disease) autosomal dominant disorder distributed over the skin and oral mucous membranes present hematuria epistaxis.

138
Capillary malformations

139
MISC. “BENIGN” TUMORS -ectasias, telangiectasias
Nevus Flammeus,, port wine stain---- Spiders (spider telangiectasias), ass. W. pregnancy, cirrhosis Osler-Weber-Rendu Disease (Hereditary Hemorrhagic Telangiectasia) Bacillary Angiomatosis, in HIV patients, caused by bacilli of Bartinella species “-ectasia” is a generic term meaning dilation and is primarily used with regard to veins rather than arteries.
, ass. W. pregnancy, cirrhosis Osler-Weber-Rendu Disease (Hereditary Hemorrhagic Telangiectasia) Bacillary Angiomatosis, in HIV patients, caused by bacilli of Bartinella species. -ectasia is a generic term meaning dilation and is primarily used with regard to veins rather than arteries.")
140
The so-called port wine stain is a special form of nevus flammeus; these lesions tend to grow with a child, thicken the skin surface, and demonstrate no tendency to fade.

141
Spider Telangiectasia non-neoplastic vascular lesion grossly resembles a spider; there is a radial, often pulsatile, dilated subcutaneous arteries or arterioles (resembling legs) about a central core (resembling a body) that blanches when pressure is applied to its center.
 about a central core (resembling a body) that blanches when pressure is applied to its center.")
142
It is commonly seen on the face, neck, or upper chest
Causes. hyperestrogenic states such as pregnancy or cirrhosis.

143
Bacillary Angiomatosis Bacillary angiomatosis is an opportunistic infection in immunocompromised persons that manifests as vascular proliferations involving skin, bone, brain, and other organs. First described in patients with acquired immunodeficiency syndrome, Causative organism gram-negative bacilli of the Bartonella hensle

144
Skin lesions are red papules or nodules rounded subcutaneous masses.
Capillary proliferation due to VEGF production by HIF 1 alpha. Nuclear atypia and mitosis also lesions contain neutrophils and bacteria

145
Kaposi Sarcoma Kaposi sarcoma (KS) common in patients with acquired immunodeficiency syndrome (AIDS) prior to the advent of effective antiretroviral therapy; indeed, its presence is used as a criterion for diagnosing AIDS.
 common in patients with acquired immunodeficiency syndrome (AIDS) prior to the advent of effective antiretroviral therapy; indeed, its presence is used as a criterion for diagnosing AIDS.")
147
1.Chronic KS also called clasiic European kS
They usually present red to purple nodules on the skin on the lower extremities. Due to malignancy or altered immunity. Not seen with AIDS pateients

148
2.Lymphedenopathic KS called African or endemic KS
Skin lesions are less. Visceral involvement is more and aggressive.

149
Pathogenesis of KS KS herpes virus KSHV proteins disrupt the cell cycle and viral genes produce P53 inhibitors and prevent apoptosis

150
Malignant tumros Angiosarcoma it is a endothelial tumor. Hepatic angio sarcoma following environmental exposure Plastic factory workers(Vinayl chloride) Arsenic pesticides Radio contrast( Thorotrast) Induced by radiation
 Arsenic pesticides. Radio contrast( Thorotrast) Induced by radiation.")
151
They present as red nodules
Locally invasive and metastasize readily. Aggressive tumors.

152
VASCULAR INTERVENTIONS
ANGIOPLASTY STENTS GRAFTS Autologous (saphenous v., internal mammary a.) Synthetic (Teflon) 152
 Synthetic (Teflon) 152.")
153
PATHOLOGY OF VASCULAR INTERVENTION morphologic changes that occur in vessels following therapeutic intervention (i.e., balloon angioplasty, stenting, or bypass surgery) typically recapitulate many of the changes that occur in the setting of any vascular insult. Local EC trauma (e.g., due to a stent), vascular thrombosis (after angioplasty), and abnormal mechanical forces (e.g., a saphenous vein inserted into the arterial circulation as a coronary artery bypass graft) all elicit similar responses characteristic of vessel wall healing. As with atherosclerosis, the traumas of vascular intervention tend to induce a concentric intimal thickening composed of recruited SMCs and their associated matrix deposition
, vascular thrombosis (after angioplasty), and abnormal mechanical forces (e.g., a saphenous vein inserted into the arterial circulation as a coronary artery bypass graft) all elicit similar responses characteristic of vessel wall healing. As with atherosclerosis, the traumas of vascular intervention tend to induce a concentric intimal thickening composed of recruited SMCs and their associated matrix deposition.")
154
STENTS Metallic mesh Permanently placed
Stays patent longer than angioplasty OFTEN DRUG COATED Goals: Prevent thrombosis Prevent spasm Delay RE-stenosis

155
What is angioplasty? PT CA Percutaneous transluminal Coronary AGP Premedications Antithrobotic Prevent Vasospasm

156
GRAFTS 400,000 CABG grafts per year in USA
Saphenous v. vs. Internal mammary a. (internal thoracic a.) 50% patent after 10 years, for saphenous v. 90% patent after 10 years, for mammary a.
 50% patent after 10 years, for saphenous v. 90% patent after 10 years, for mammary a.")
157
Vascular Replacement Synthetic or autologous vascular grafts are increasingly used to replace damaged vessels or bypass diseased arteries. Of the synthetic grafts, large-bore (12- to 18-mm) conduits function well in high-flow locations such as the aorta, while small-diameter artificial grafts (≤8 mm in diameter) generally fail because of acute thrombosis
 conduits function well in high-flow locations such as the aorta, while small-diameter artificial grafts (≤8 mm in diameter) generally fail because of acute thrombosis.")
Similar presentations

















 Dr. Raid Jastania. Vasculitis Inflammation of the walls of the vessels Causes of inflammation: –Infectious, physical, chemical,>")





 Aneurysms & Dissections Veins & Lymphatics Tumors.>")




